
Abstract
This study aims to describe the gradient and the frequency with which the end tidal carbon dioxide (EtCO2) misclassifies the arterial carbon dioxide (PaCO2) in the prehospital environment. This retrospective observational study included 53 adult patients (aged ⩾ 18 years) who underwent prehospital arterial catheterisation following a traumatic mechanism who were conveyed to the regional Major Trauma Centre (MTC), 01.02.2015–17.04.2023. The PaCO2–EtCO2 gradient was more than >1 kPa difference in most patients (43/53 (81.1%)) and the ETCO2 misclassified the PaCO2 in over two-thirds of patients (38/53 (71.7%)). Overall, EtCO2 is not a reliable surrogate for PaCO2 during trauma.
Introduction
Tight arterial carbon dioxide (CO2) control is fundamental to reducing the impact of secondary brain injury in patients with traumatic brain injury. 1 Unintentional hypercapnia and hypocapnia may worsen outcomes for patients, particularly those with a traumatic brain injury (TBI). 1 Current guidance recommends using end-tidal carbon dioxide (EtCO2) as a surrogate for PaCO2 to guide ventilation strategy when arterial blood gas (ABG) sampling is less readily available. 1 The EtCO2 is recommended to be maintained between 4.0 and 4.5 kPa, and the accepted gradient between the PaCO2–ETCO2 is considered to be 0.5–1.0 kPa; however, reappraisals have demonstrated heterogeneity in the agreement between the PaCO2 and EtCO2, as well as variability in the gradient.1–3
This study aims to describe the gradient and the frequency with which the EtCO2 misclassifies the PaCO2 in the prehospital environment.
Methods
This retrospective observational study included adult patients (aged ⩾ 18 years) who underwent prehospital arterial catheterisation following a traumatic mechanism who were conveyed to the regional Major Trauma Centre (MTC), 1st February 2015–17th April 2023. Data were obtained from both the East Anglian Air Ambulance (EAAA) electronic medical record system (HEMSbase, Medic One Systems Ltd, UK) and the hospital electronic medical record system (Epic Hyperspace Production®, Epic Systems Corporation, Verona, WI, USA).
EtCO2 measurements were matched within 5 min of the prehospital ABG sample. Hypocapnoea was defined as <4 kPa, normocapnoea as 4–6 kPa, and hypercapnoea as >6 kPa.1,3 Misclassification was defined as a discrepancy between the EtCO2 and PaCO2 categories (e.g. one indicating normocapnoea and the other hypocapnoea or hypercapnoea). Data were described as number (percentage) for categorical variables and median [interquartile range (IQR)] for continuous variables.
Results
During the study period, 53 patients with prehospital arterial catheterisation for a trauma mechanism and who had an ABG recorded prehospital were identified (Figure 1).
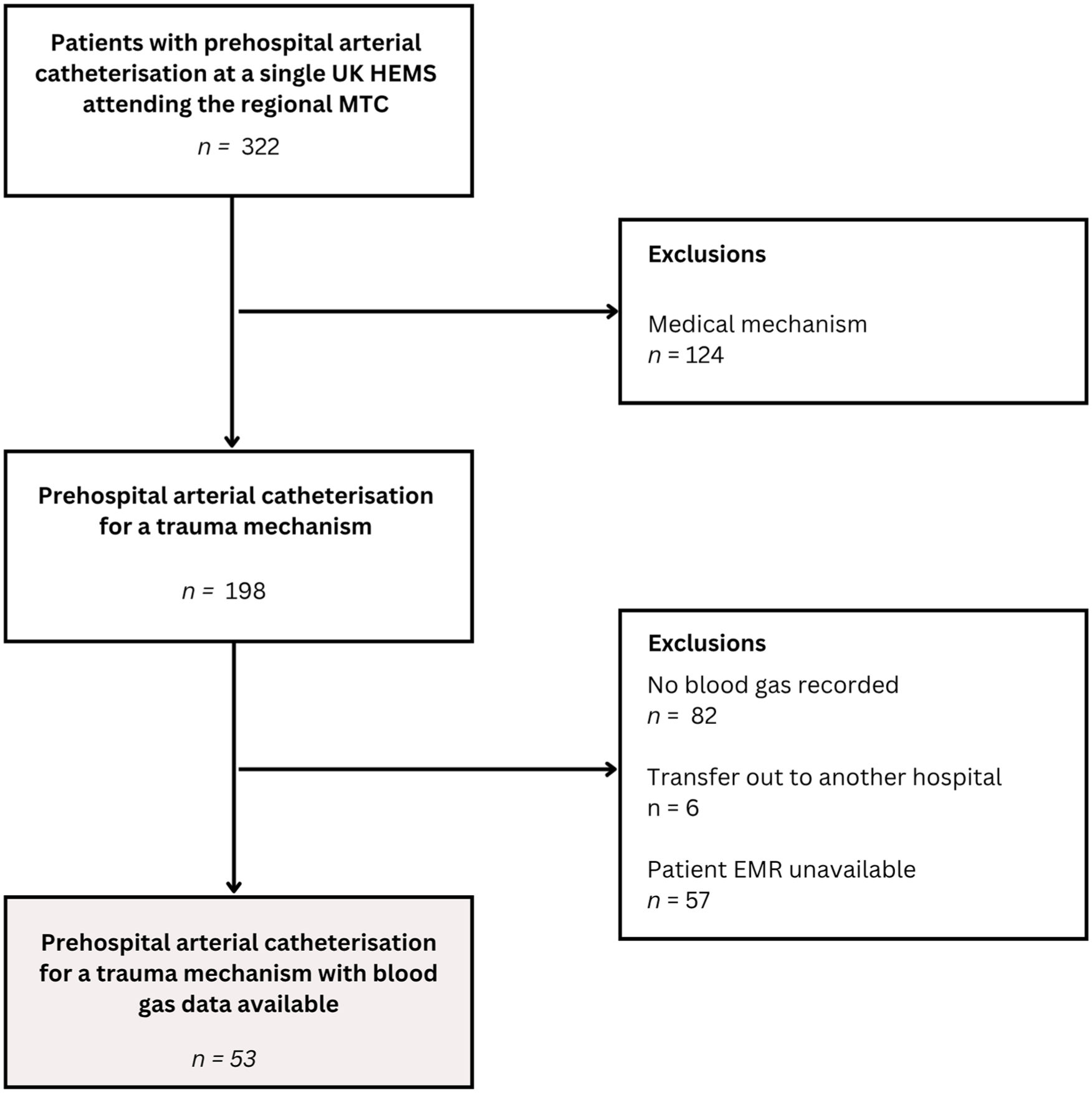
Flow diagram of included and excluded patients.
Demographics and injury characteristics are described in Table 1.
Demographics and injury characteristics.
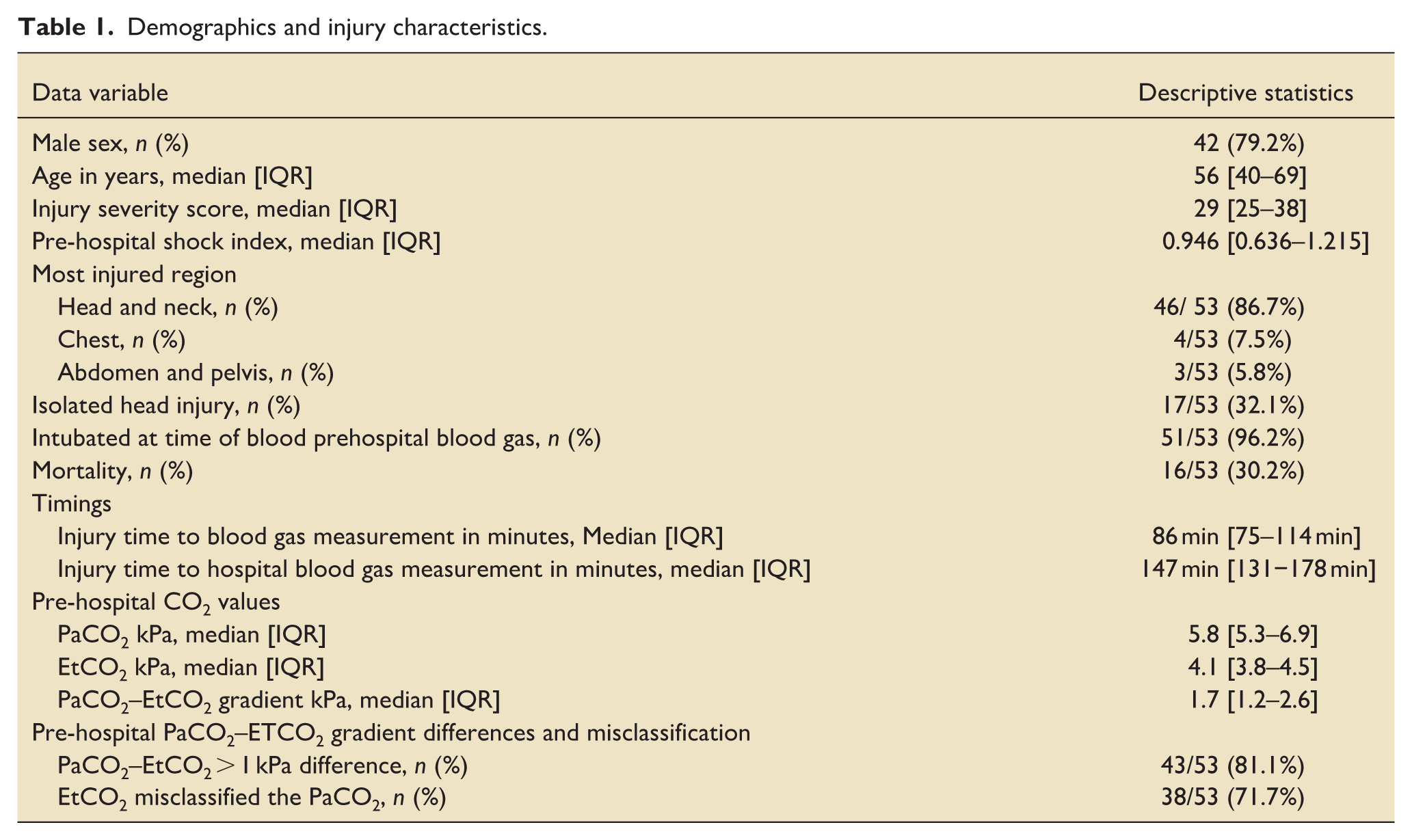
Most patients were intubated at the time of ABG sampling (51/53 (96.2%)). The PaCO2–EtCO2 gradient was more than >1 kPa difference in most patients (43/53(81.1%)) and the ETCO2 misclassified the PaCO2 in over two-thirds of patients (38/53 (71.7%)).
Discussion
This study observed that PaCO2–EtCO2 gradient was frequently more than the accepted gradient of 0.5–1.0 kPa, and the EtCO2 often misclassified the PaCO2.
This study supports previous studies demonstrating the wider gradient and its association with mortality.2–4 However, previous studies have either not focussed on trauma where targeted normocapnia is vital, or been undertaken later in the injury journey in the emergency department or intensive care unit.2–4 Given the differences in methodology between this paper and smaller, previously published papers utilising the same database, only one patient was found to overlap.2,3 Moreover, this study is advantageous in closely matching the EtCO2 and PaCO2 to within 5 min, which is particularly important given the variability in gradient demonstrated in prior studies.2–4
Currently, only a small proportion of critical care services in the UK can measure PaCO2 prehospital, and since the data comes from a single centre, the results may not be widely applicable. 5
Overall, EtCO2 is not a reliable surrogate for PaCO2 in guiding ventilator settings during trauma. Clinicians should be mindful of this and consider ABG sampling when available.
Footnotes
Acknowledgements
The authors wish to acknowledge Kate Lachowycz, Rob Major, and Paul Rees from the Department of Research, Audit, Innovation, and Development (RAID) at East Anglian Air Ambulance for their support of this project and their previous research into prehospital arterial catheterisation.
Ethical considerations
The UK Policy Framework for Health and Social Care Research from the NHS Health Research Authority and Medical Research Council was applied. The decision tool determined that no formal ethical approval was required.
Author contributions
Owen Hibberd: Conceptualisation, data curation, investigation, formal analysis, methodology, project administration, writing–original draft. James Price: Conceptualisation, data curation, investigation, formal analysis, methodology, writing – review & editing. Edwin Li Ping Wah-Pun Sin: Data curation, investigation, project administration, writing – review & editing. Hazel Farman: Data curation, investigation, project administration, writing – review & editing. Michael Phillips: Data curation, investigation, project administration, writing – review & editing. Muzammil Arif Din s/o Abdul Jabbar: Data curation, investigation, project administration, writing – review & editing. Ed Barnard: Conceptualisation, formal analysis, methodology, supervision, writing – review & editing. All authors have made a substantial contribution to the concept or design of the article; or to the acquisition, analysis, or interpretation of data for the article; have drafted the article or revised it critically for important intellectual content; have approved the version to be published; have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available upon reasonable request to the corresponding author following EAAA approval.