
Abstract
Introduction:
Sepsis poses a substantial global health threat, accounting for approximately 20% of all deaths worldwide. In Australia, available reports indicate a rising incidence, with over 84,000 hospital admissions each year. Although in-hospital survival has improved, many survivors continue to experience long-term physical, psychological, cognitive, and health-related quality-of-life (HRQoL) challenges, collectively known as post-sepsis syndrome (PSS). However, research examining these long-term outcome trajectories remains fragmented and has not been comprehensively synthesised. This scoping review aims to map current evidence, clarify key concepts, and identify gaps in knowledge regarding PSS and related post-sepsis outcomes within the Australian context.
Methods:
A scoping review was carried out in accordance with the updated methodological framework provided by the Joanna Briggs Institute (JBI). A comprehensive search across multiple databases was conducted, including both peer-reviewed and grey literature. Two reviewers independently screened and extracted data. Narrative thematic analysis was employed to identify key themes and knowledge gaps. Reporting followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist, and the review protocol was published on the Open Science Framework (OSF): https://doi.org/10.17605/osf.io/xhzfq.
Result:
Eighteen studies, primarily observational cohort designs, investigated outcomes among a total of 542,599 sepsis survivors. Less than half (39%) of the studies provide nationwide data. Six key themes emerged: long-term mortality risk, hospital readmissions, reduced HRQoL, long-term physical impairments, cognitive dysfunction, and mental health challenges. The most frequently reported outcomes were elevated post-hospital mortality and reduced HRQoL. Notably, 1-year mortality rates ranged from 12.5% to 36.9%. HRQoL was consistently impaired across all domains when compared to the general population. Despite ongoing needs in survivors, post-discharge rehabilitation and support services were reported to be inadequate
Conclusion and recommendations:
This scoping review shows that sepsis survivors in Australia experience multidimensional long-term complications and increased mortality risk. Stakeholders need to provide greater emphasis on the development of tailored post-sepsis care models and follow-up strategies to improve life after experiencing sepsis. Moreover, methodological limitations in the existing literature—including inconsistent case definitions, limited outcome measurement, short follow-up, and insufficient exploration of factors—highlight the need for robust, longitudinal research to strengthen evidence bases.
Introduction
Sepsis constitutes life-threatening organ dysfunction precipitated by a dysregulated host response to infection. 1 The World Health Organisation (WHO) identifies sepsis as a major global health threat. 2 In 2017, an estimated 49 million people worldwide developed sepsis, and approximately 11 million died, accounting for nearly 20% of global mortality. 3 In Australia, recent reports show a rising incidence of sepsis,4,5 with more than 84,000 hospitalisations recorded in 2022–23—substantially higher than earlier estimates of approximately 55,000 cases. 3 Cumulatively, this rising incidence has resulted in over 936,000 sepsis-related hospitalisations over the 10-year period from 2013–14 to 2022–23. 6 In contrast to this increasing hospitalisation rate, advancements in sepsis management have led to improvements in in-hospital survival.7,8 Correspondingly, the trend of sepsis mortality in Australia is decreasing.4,9 However, hospital discharge marks the beginning—not the end—of recovery trajectories for sepsis survivors. 10
Evidence showed that sepsis survivors often face a range of long-term complications collectively referred to as post-sepsis syndrome (PSS).11,12 Although there is no universally accepted definition, PSS is widely described as an evolving, multifaceted condition encompassing persistent physical, medical, psychological, cognitive, and health-related quality of life (HRQOL) impairments that may last from weeks to decades following hospital discharge.11 –13 While approximately half of survivors recover fully within 2 years,7,14 a substantial proportion continue to experience ongoing complications, including recurrent infections, chronic pain, fatigue, disabling muscles, ongoing organ dysfunction, poor concentration, difficulty in intellectual functions, and mental health disorders, that puts survivors at increased risk of rehospitalisation, mortality, and diminished HRQoL.11,12,15 For instance, a systematic review of epidemiological studies reported that 16.1% of sepsis survivors die within 1 year, 16 and other studies have shown that 5-year mortality rates range from 43.8% to 62.1%.17 –20 Besides, sepsis survivors also face recurrent hospital readmission, with 18%–26% returning within 30 days21 –27, 30%–40% within 90 days,22,28 and over 40% within 1 year of survival.11,22,29 Physical symptoms like fatigue, 13 chronic pain,13,30 and gastrointestinal issues 13 were also commonly experienced by sepsis survivors. Notably, chronic pain affects 14%–77% of ICU survivors, including sepsis patients, during the first year after discharge.31,32
Furthermore, sepsis survivors face an elevated risk of chronic conditions, particularly cardiovascular, pulmonary, liver, and renal diseases. Cardiovascular disease is now widely recognised as both a risk factor and a potential consequence of sepsis.33,34 Accordingly, a systematic review and meta-analysis study reported a higher rate of cardiovascular events among sepsis survivors compared to non-septic controls, with an incidence of myocardial infarction, stroke, and heart failure ranging from 3% to 9% and corresponding hazard ratios of 1.77, 1.67, and 1.65, respectively. 34 The kidney is also one of the commonest organs affected in sepsis patients. Sepsis-associated acute kidney injury (S-AKI) occurs in approximately two-thirds of septic shock patients, 35 with a quarter requiring renal replacement therapy. 36 S-AKI, in turn, increases the risk of permanent kidney damage, causing chronic kidney diseases (CKD) in survivors. 37
Additionally, cognitive impairments such as memory loss, attention deficits, poor concentration, and executive dysfunction are also common among sepsis survivors,12,38 with an estimated prevalence of 12.5%–21%. 39 Similarly, sepsis survival is linked to a higher chance of all causes of dementia. 40 The long-term effects of sepsis significantly compromise survivors’ HRQoL,12,41 with a growing body of global literature showing that HRQoL remains impaired for months to years following recovery.41 –44
More importantly, the impact of PSS extends to families, caregivers, health care providers, and policymakers. 44 For example, sepsis survivors had higher healthcare costs and healthcare utilisation compared to individuals without sepsis.11,45
In this context, PSS has emerged as a significant global public health priority and a complex clinical challenge due to its enduring and multidimensional impact on sepsis survivors.11,12,46 Although PSS shares some similarities with post-intensive care syndrome (PICS)— which refers to new or worsening physical, cognitive, or mental health impairments following ICU admission of critical illnesses 47 —important distinctions exist. PSS affects only sepsis survivors, including those who were not admitted to the ICU, whereas PICS is limited to critically ill patients who required ICU admission. 11 As such, a thorough understanding of PSS and its associated outcomes warrants focussed investigation from clinicians and researchers. In Australia, although sepsis incidence is rising and in-hospital mortality rate is declining, research on post-sepsis outcomes remains fragmented, and no comprehensive synthesis currently maps the scope, quality, and gaps in the existing evidence base. To address this, the present study aims to conduct a scoping review to summarise current knowledge on PSS and related long-term outcomes, clarify concepts, and highlight gaps to inform future research and policy development. The Supplemental Material (Item S1) further illustrates the rationale for the scoping review.
Methods and materials
A scoping review was carried out in accordance with the updated methodological framework provided by the Joanna Briggs Institute (JBI). 48 Given the broad and complex nature of post-sepsis syndrome (PSS), the heterogeneity of the evidence, and the objective of mapping findings from the existing literature, a scoping review approach was deemed appropriate. A review protocol was developed and registered with the Open Science Framework: https://doi.org/10.17605/OSF.IO/XHZFQ. We also followed the EQUATOR Network’s reporting guidelines, specifically the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR), to ensure transparent and comprehensive reporting (Supplemental Material, Item S2).
Inclusion and exclusion criteria
Eligible studies for the scoping review were selected based on the Population, Concept, and Context (PCC) framework. The detailed inclusion and exclusion criteria are provided in the Supplemental Material (Item S3).
Search strategy
To identify relevant literature for the scoping review, a comprehensive search strategy was created for each database in consultation with a research librarian and appraised using the Peer Review of Electronic Search Strategies (PRESS) 2015 checklist.49,50 Both published and grey literature were searched to minimise publication bias. Published literature was identified from several online databases, including MEDLINE (Ovid), CINHAL Complete (EBSCOhost), Web of Science (Clarivate), and Scopus (Elsevier) from inception to June 2025. A composite of keywords and Medical Subject Heading (MeSH) terms was used to construct the search strategy. Boolean logic and proximity operators (AND, OR, NOT) were applied to connect the search terms and enhance the searching strategy. The key search terms for the review include sepsis, severe sepsis, septic shock, sepsis survivorship outcomes, long-term outcomes, post-sepsis syndrome, and Australia (Supplemental File, Item S4).
Evidence selection and screening
All identified articles were imported to Covidence software for deduplication and screening. Duplicates were automatically identified and manually verified before removal. The remaining unique records were reviewed in two phases. First, the title and abstract were screened for inclusion by two reviewers (BB, AM). Then, the full text was also reviewed by both reviewers, with discrepancies resolved through discussion. The study selection process was charted using a PRISMA flow diagram.
Data extraction and quality assessment
A bespoke data-charting form was developed, piloted on five studies, and refined before use. Data extraction was performed by the primary author (BB) with the extracted data validated for its completeness, consistency, and accuracy by the other authors (DC, JS, and AM). Extracted information included study characteristics, participant socio-demographic details, and detailed outcome findings (Supplemental File, Item S5).
Although optional for scoping reviews, JBI critical appraisal checklists were applied according to enhanced transparency in evidence interpretation. 51 We used a diverse JBI checklist according to the study design, and most included studies (14, 78%) were assessed as high quality (Supplemental file, Item S6).
Data processing, analysis, and reporting
Basic descriptive statistics—including frequencies, means, and proportions—were used to summarise key characteristics of the included studies, such as study setting, study design, population demographics, and outcome measures. A narrative thematic analysis was then employed. Data were organised thematically through a hybrid deductive–inductive approach, using the Shankar-Hari et al. PSS conceptual framework. 15 Findings are presented through narrative summaries, tables, and visual tools such as charts
Ethical considerations
As the study involves the synthesis of publicly available data and does not involve human participants, ethics approval was not required.
Results
Overview of the studies
The systematic search retrieved 2533 citations from 4 databases: MEDLINE (n = 678), Scopus (n = 1085), CINAHL (n = 234), and Web of Science (n = 536). An additional 67 records were recovered through grey literature sources: Google, Google Scholar, Trove, and ProQuest Thesis and Dissertations. In total, 2600 references were imported into Covidence for deduplication and screening. After removing 694 duplicates, 1906 unique titles and abstracts were screened, followed by full-text review. Eighteen (18) studies met the inclusion criteria. The PRISMA flow diagram presents the detailed selection process (Figure 1).
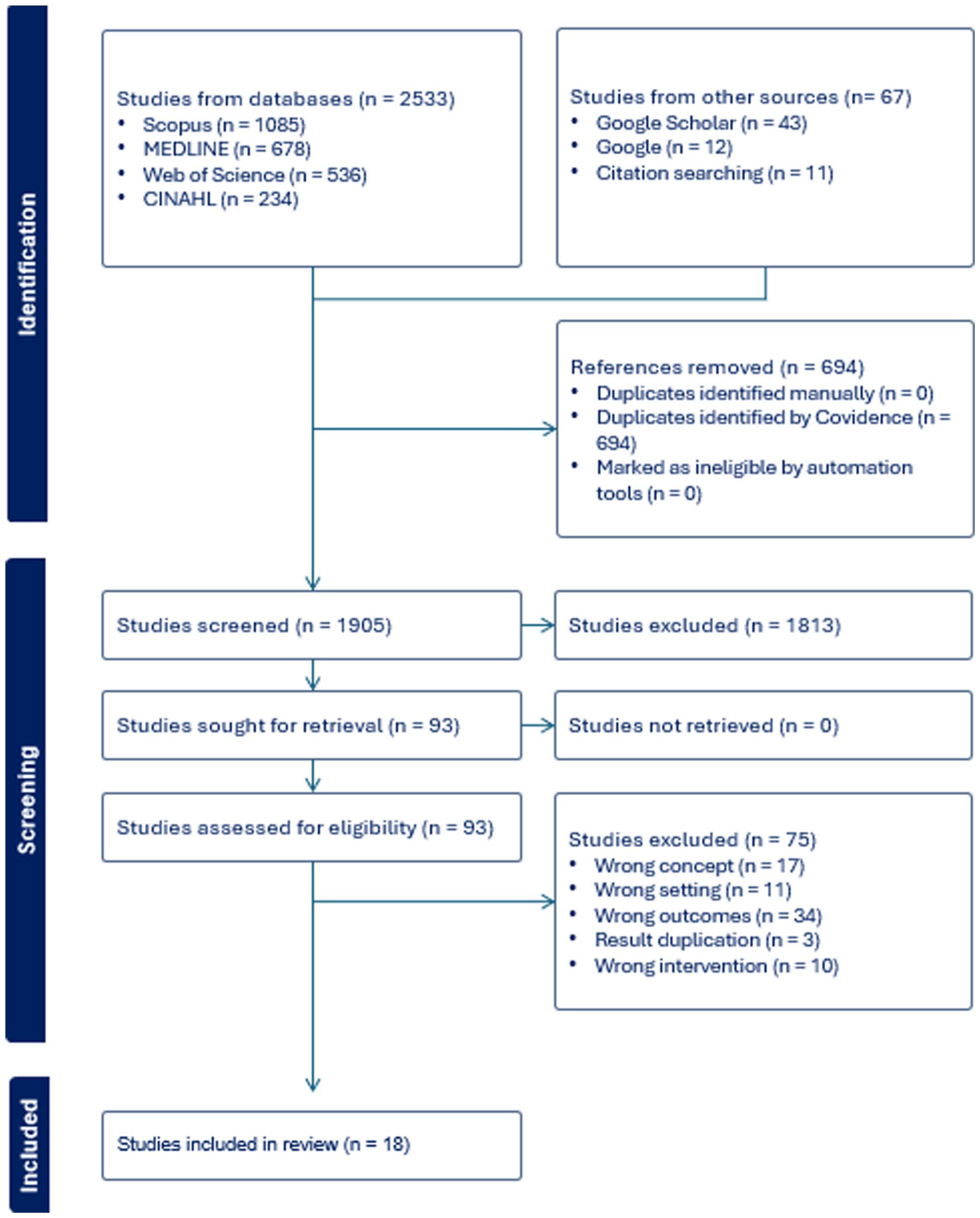
The PRISMA flow diagram of the scoping review of trajectories of sepsis survivors in Australia, 2025.
Socio-demographic characteristics of study participants
Of the 18 studies, only 14 peer-reviewed articles reported participant-level sociodemographic data; the 4 grey literature documents (standards and reports) did not provide such details.52 –55 Collectively, these 14 studies included 542,599 individuals. The smallest sample size was 39 participants in a qualitative study 56 ; the largest was 264,678 in cohort studies conducted in New South Wales.57,58 In the included studies, the mean age of participants was generally above 40,56,57,59 –69 ranging from 46.9 64 to 65.5 years. 61 Male participants predominated in the majority (10/14) of studies57,58,60,61,64 –69 (Supplemental File, Item S5).
Characteristics and key PSS outcome findings of the included studies
Regarding the key PSS and related long-term outcome findings of the included studies, six key outcome themes were identified. Post-hospital mortality was the most frequently reported outcome (11 studies; 11 studies),57,58,60 –68 followed by HRQoL.57,59,60,62,67 –69 Conversely, the physical and cognitive sequelae of PSS were infrequently addressed: two studies quantified pain56,57; two assessed fatigues54,56; and four studies explored cognitive dysfunctions.52,54,56,60 Figure 2 further illustrates the domains of post-sepsis syndromes that were reported by Australian literature (Figure 2).
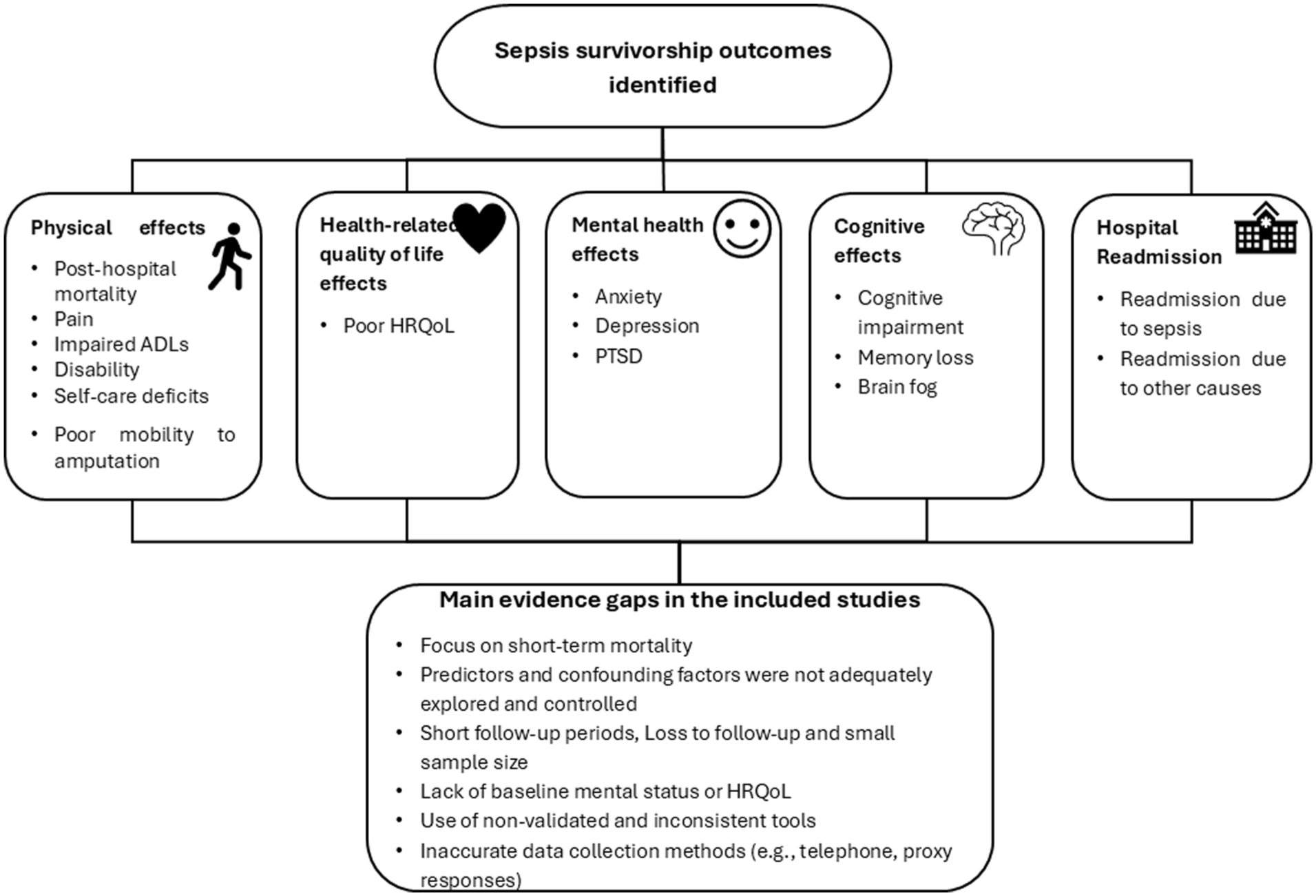
Diagrammatic presentation of trajectories of sepsis survivors in Australia, 2025.
Long-term mortality risks in sepsis survivors
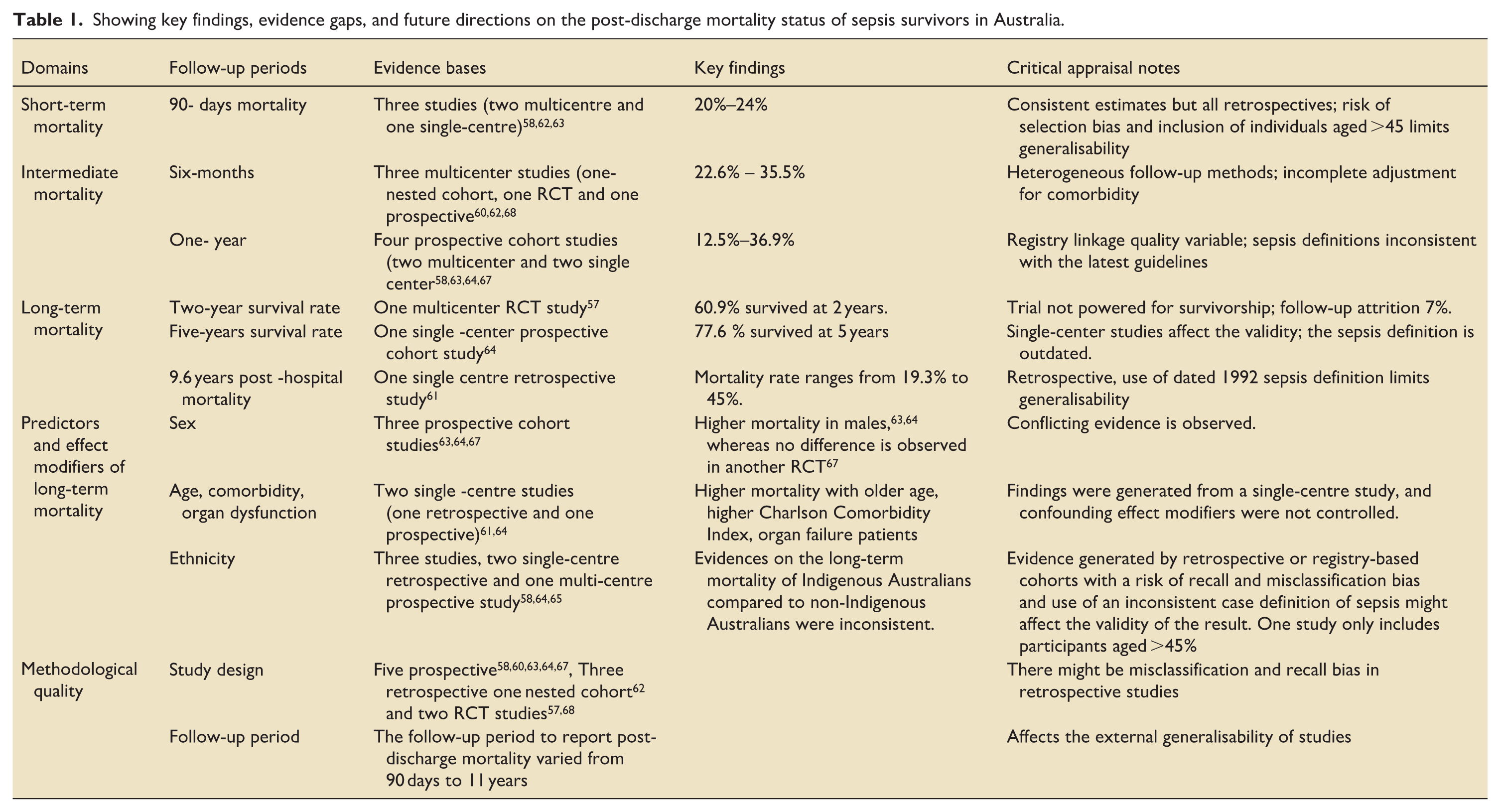
Post-ICU or hospital mortality in sepsis survivors has been reported across 11 Australian studies. Nevertheless, follow-up intervals and mortality ascertainment windows were heterogeneous, ranging from 90 days58,62,63 to 11 years. 66 Most studies assessed outcomes at 6 months60,62,68 and 1 year post-discharge,58,63,64,67 while only two studies extended follow-up to 5 years or more.61,66 Across studies, the mortality rates at 90 days, 6 months, and 1 year ranged from 20%–24%, 22.6%–35.5%, and 12.5%–36.9%, respectively.58,60 –63,68 While international evidence suggests that excess mortality may persist for a decade or longer,70,71 longer-horizon data were sparse in Australia. A multicentre clinical trial reported survival rate of 60.9% at 2 years of the post-sepsis period, 57 whereas another population-based cohort study estimated a 5-year crude survival of 77.6%. 64 Furthermore, the only decade-long evidence indicated that, after 9.6 years of follow-up, post-hospital mortality was 45% for community-acquired sepsis and 42% for nosocomial sepsis. 61
The review also divulged that, across the included studies, long-term survival among sepsis survivors was frequently reported to be poorer than that of comparator groups, including the general population and non-sepsis ICU patients. 66
Evidence on the determinants of long-term mortality after sepsis is limited and inconsistent. Findings related to sex are mixed, with some studies reporting higher 90-day mortality (25.3% vs 22.5%; p < 0.001) and 1 year mortality (39.3% vs 33.7%; p < 0.001) among male survivors,63,64 whereas a prospective multicentre trial found no significant sex-based difference in 1-year mortality. 67 The role of ethnicity also remained debatable. One study reported higher long-term mortality among Indigenous Australians, 64 while others show comparable rates.58,65 Notably, even when mortality rates are similar, a study conducted in northern Queensland concluded that Indigenous Australians died at a significantly younger age than non-Indigenous patients (58 vs 70 years: p < 0.0001). 65 Other factors more consistently associated with increased long-term mortality include older age, higher comorbidity burden, and greater severity of sepsis61,64 (Supplemental File, Item S5, and Table 1).
Showing key findings, evidence gaps, and future directions on the post-discharge mortality status of sepsis survivors in Australia.
Hospital re-admissions following surviving sepsis
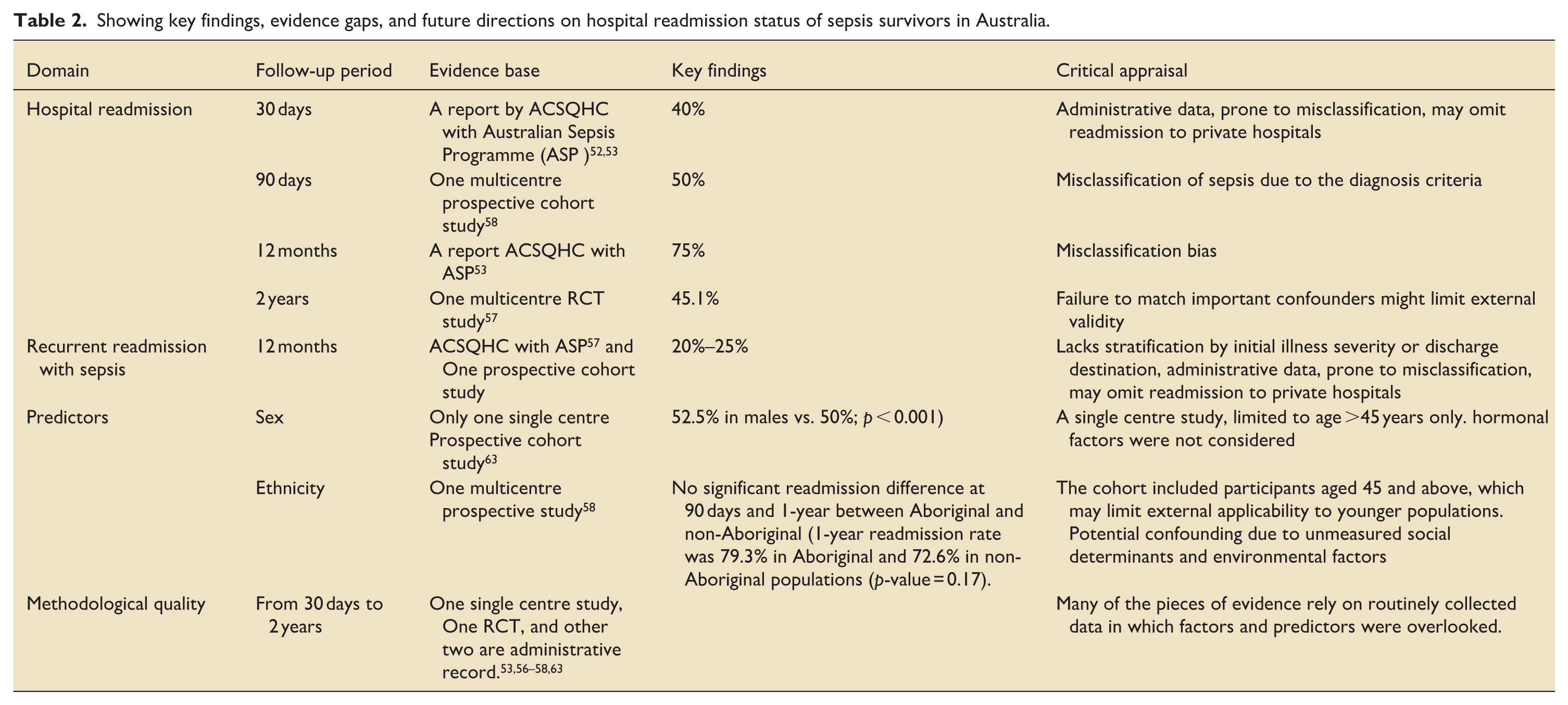
Five Australian studies have quantified hospital readmissions following survival of an index sepsis admission, with follow-up horizons spanning from 30 days to 2 years.52,53,57,58,61 The most comprehensive data come from a report by the ACSQHC, in partnership with the Australian Sepsis Network, which showed that 40% of sepsis survivors were readmitted within 30 days and 75% within 12 months. 53 Similarly, Thompson et al. showed that about half and 75% of sepsis survivors were readmitted to the hospital within 90 days and 1 year of the follow-up. 58 Of those readmitted, 20%–25% returned due to recurrent sepsis episodes.53,58 Additionally, a multicentre follow-up study in New South Wales found that, over a 2-year period, 71.7% of sepsis survivors were readmitted to the hospital, a rate comparable to that observed in non-sepsis survivors. 57
Limited evidence exists on what drives readmission risk in sepsis survivors in Australia. A single-centre prospective study revealed that male sepsis survivors had significantly higher odds of readmission within 90 days compared to females (52.5% vs. 50%; p < 0.001). 63 With respect to ethnicity, although data remain scarce, Thompson et al. found no significant difference in readmission rates between Indigenous and non-Indigenous patients 58 (Supplemental File, Item S5 and Table 1 and Table 2).
Showing key findings, evidence gaps, and future directions on hospital readmission status of sepsis survivors in Australia.
Poor HRQol outcome in sepsis survivors
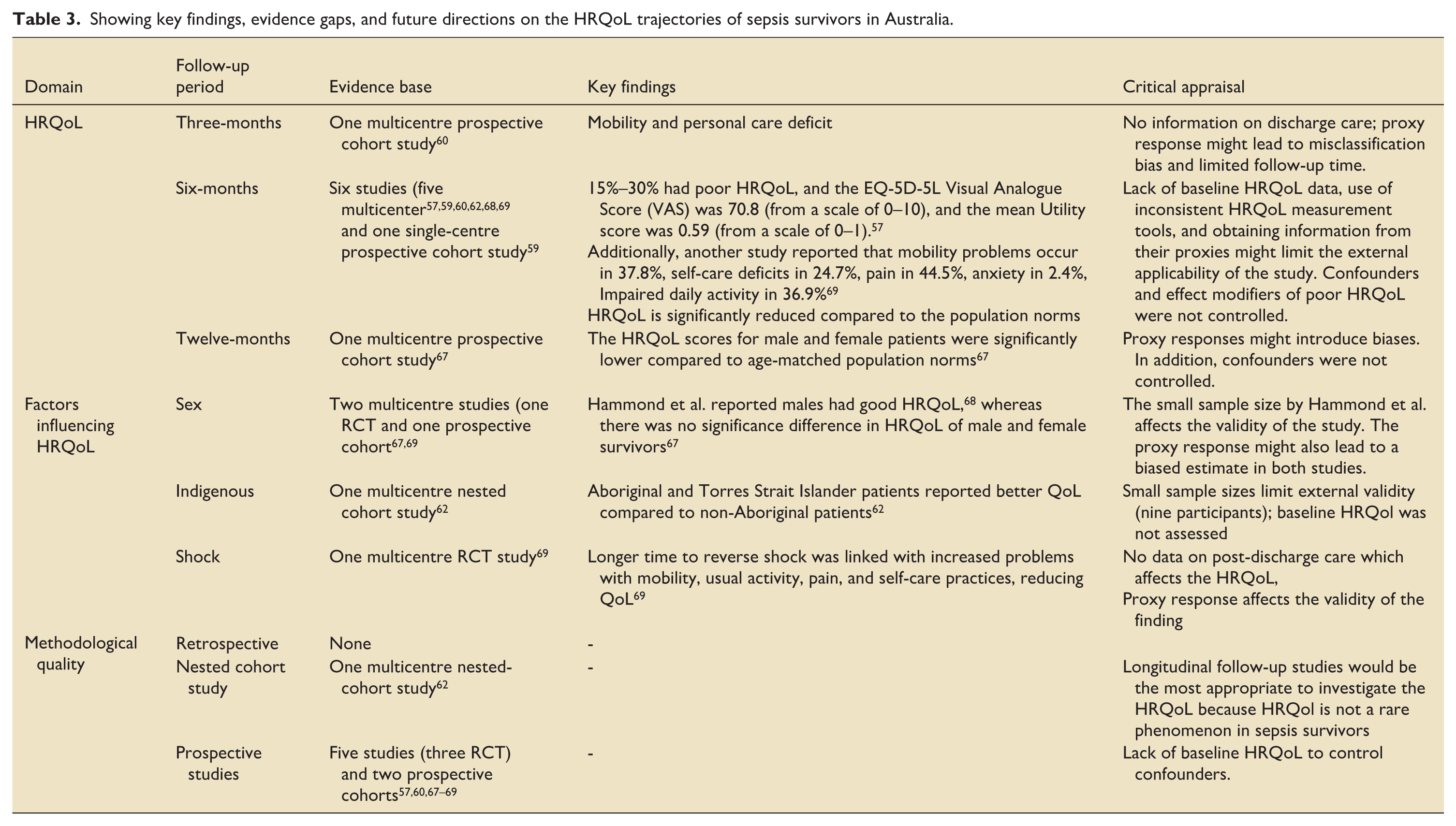
Seven studies evaluated HRQoL among Australian sepsis survivors, with follow-up durations ranging from 3 months to 2 years.57,59,60,62,67 –69 Most of the studies examined the HRQoL at 6 months.57,59,60,62,68,69 The EuroQol-5D (three- or five-level version) was the predominant instrument,57,60,62,67 –69 supplemented in some studies by the SF-36 or SF-12v2.60,62,68,69 In almost all studies, sepsis survivors demonstrated substantial decrements across all HRQoL domains,57,59,67 –69 with scores consistently below Australian population norms.59,67,68 For example, Hammond et al. reported moderate-to-severe HRQoL problems in 15%–30% of survivors. 69 Severity of sepsis episode influenced outcomes: HRQoL reductions were greater after severe sepsis or septic shock than after uncomplicated sepsis. 59 Moreover, three studies in the review compared the HRQol with other non-sepsis ICU patients and revealed comparable results.57,60,68 Physical domains—particularly mobility and the ability to perform usual activities—were the most frequently and markedly impaired components.57,60,69 Notably, Thompson et al. documented mobility limitations in 37.8%, self-care deficits in 24.7%, and pain in 44.5% of survivors, respectively. 57
Regarding factors influencing HRQoL, findings on the impact of sociodemographic and clinical variables remain inconclusive. One study found that male sepsis patients experienced lower levels of pain compared to females, which was associated with better HRQol, 69 while another detected no significant gender differences. 67 Additionally, although based on a small sample (n = 9), a nested cohort study observed that, 6 months after discharge, Indigenous sepsis patients reported better HRQoL compared to non-Indigenous Australians. 62 This finding is highly indefinite due to sample size and potential selection bias. Furthermore, a multicentre RCT showed no significant HRQoL differences between patients treated with Early Goal-Directed Therapy (EGDT) and those receiving standard care 68 (Supplemental File, Item S5 and Table 3).
Showing key findings, evidence gaps, and future directions on the HRQoL trajectories of sepsis survivors in Australia.
Physical impairments in sepsis survivors
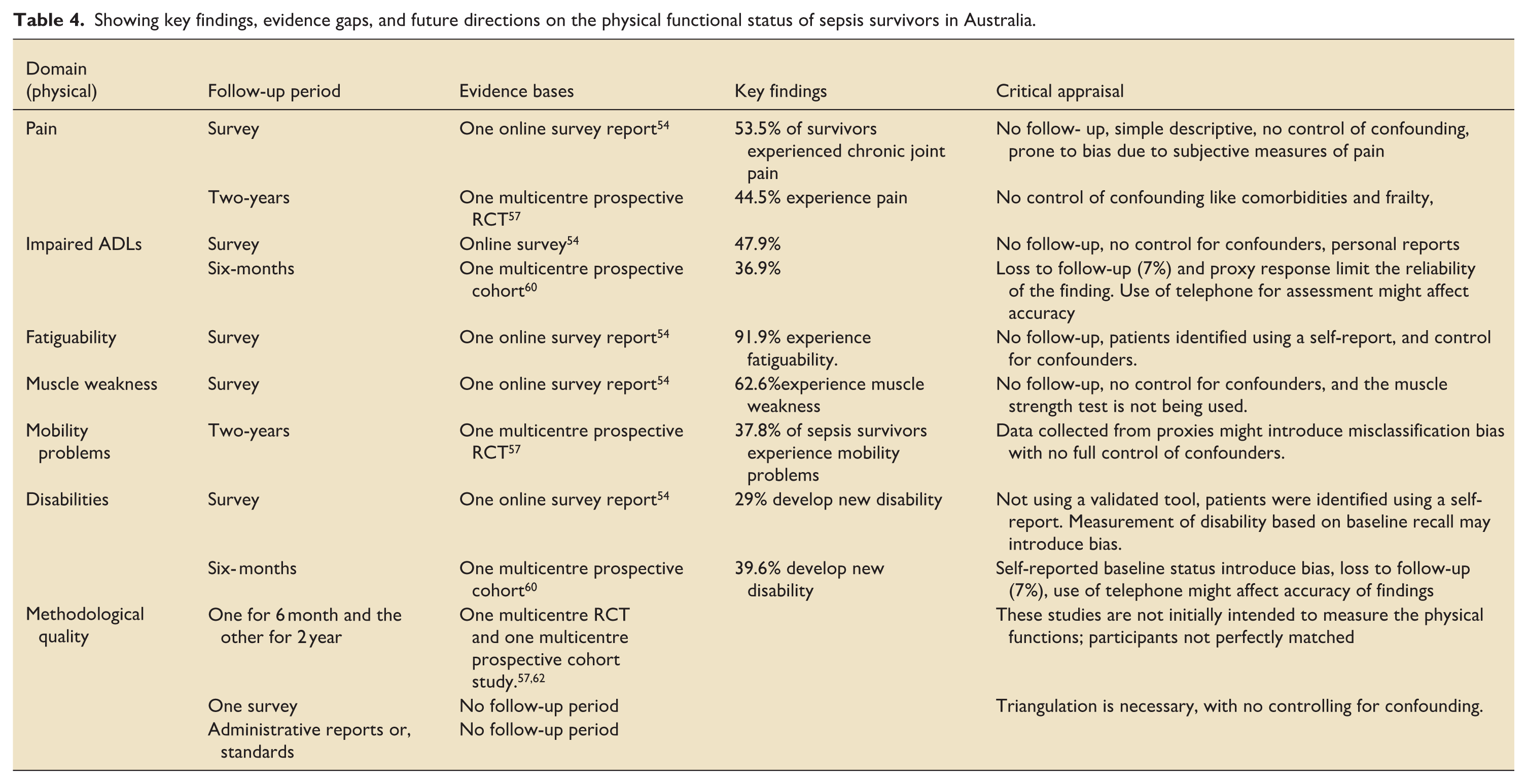
In Australia, physical impairments ranging from loss of mobility and difficulty with daily tasks like bathing and toileting to severe complications like amputations were the other domain of PSS reported in the included studies.54,56,57,62 Notably, none of the included studies used validated performance-based tools—such as the Six-Minute Walk Test (6MWT), Manual Muscle Testing (MMT), or dynamometry—which are standard measures of physical functioning in critically ill patients. Some studies also relied on proxy respondents or telephone-based assessment tools, which may introduce measurement bias.57,60 Despite being small, available studies showed that survivors may experience a wide spectrum of physical impairments. Pain and impaired ability to perform daily living activities were among the most frequently reported complaints. Two studies found that 44.5% to 53.5% of survivors experienced chronic pain.57,62 Impaired activity of daily living also happened in about 36.9% to 47.9% of sepsis survivors.54,57 Fatigue, muscle weakness, mobility problems, disability, and amputation were also commonly experienced by sepsis survivors in Australia. In this context, an online survey in Queensland detected that fatigue and weak muscles were observed in 91.9% and 62.6% of survivors, respectively. 54 New disability also occurred in nearly one-third (29%) to 39.6% of sepsis survivors54,60 (Supplemental File, Item S5, and Table 4).
Showing key findings, evidence gaps, and future directions on the physical functional status of sepsis survivors in Australia.
Cognitive dysfunction in sepsis survivors
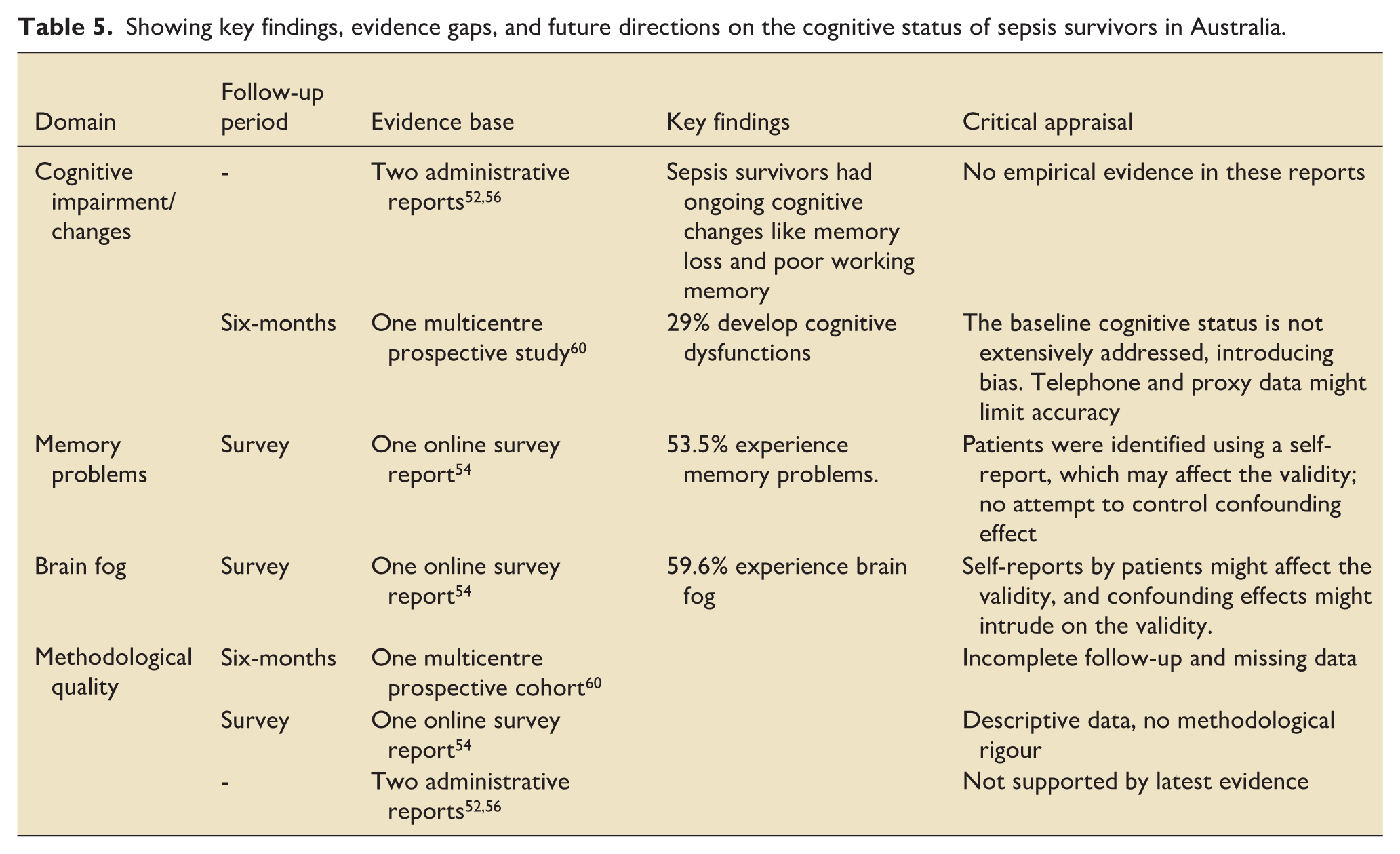
Four studies covered the cognitive aspects of sepsis survivors,52,54,56,60 whereby two of them were administrative reports or guidelines from ACSQHC.52,56 Of the four included studies, only one study by Hodgson et al. assessed the cognitive status of survivors using the validated tool, the Montreal Cognitive Assessment tool (MoCA). 60 The maximum follow-up period to assess cognitive impairment in the included studies spans 6 months. 60 Accordingly, at 6 months post-discharge, it was found that one-third (29.5%) of survivors had cognitive impairment. 60 The study also found that the prevalence of cognitive dysfunction among sepsis survivors was consistent with the matched non-sepsis ICU cohort. However, interpretation is limited by the lack of baseline cognitive data and the use of proxy and telephone-based assessment. 60 In contrast, an online survey conducted in Queensland, in northeastern Australia, reported self-perceived brain fog in 59.6% of respondents and memory loss in 53.5%. Additionally, ACSQHC reports suggest that sepsis survivors in Australia may be at increased risk of long-term cognitive impairments, including memory loss and reduced working memory capacity52,56 (Supplemental File, Item S5 and Table 5).
Showing key findings, evidence gaps, and future directions on the cognitive status of sepsis survivors in Australia.
Long-term mental health challenges in sepsis survivors
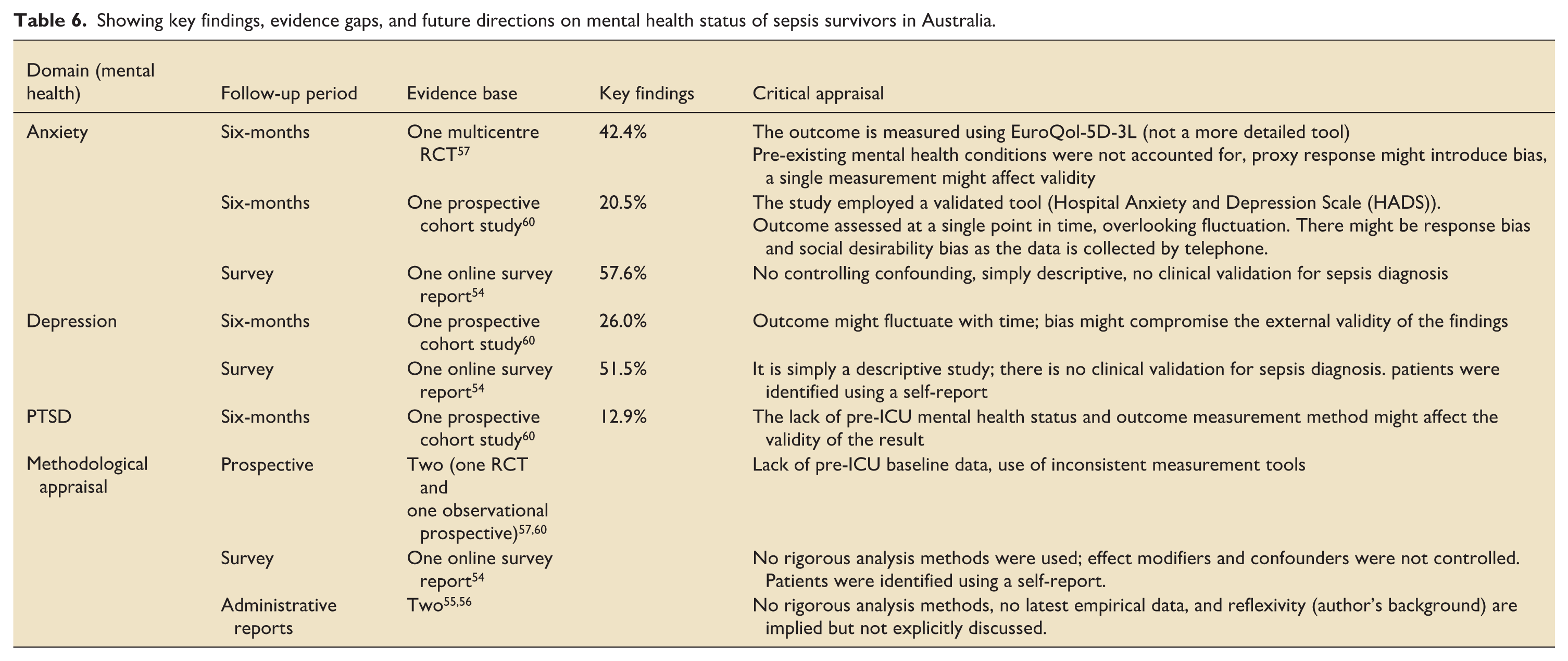
Five studies examined the mental and psychological sequelae experienced by sepsis survivors in Australia.54 –57,60 The most frequently reported mental health conditions included PTSD, generalised anxiety disorder, and depression. Concerning the outcome, only three studies reported mental health outcomes quantitatively.54,57,60 Between 20.5 and 57.6% of sepsis survivors encountered anxiety,54,60 while depression affected 26.0%–51.5% of survivors.54,57,60 An online survey in Queensland also found that 47.5% of survivors reported losing interest in their usual activities—a common symptom of depression. 54 Furthermore, a multicentre study found 12.9% of sepsis patients were at risk of PTSD 6 months after hospital discharge. 60 In addition, a nationwide report by the ACSQHC and the Sepsis Australia Network emphasised that mental health impacts extend beyond survivors themselves, affecting families, friends, and bereaved individuals, many of whom experience ongoing psychological distress and disruptions to daily life and work 56 (Supplemental File, Item S5 Table 6).
Showing key findings, evidence gaps, and future directions on mental health status of sepsis survivors in Australia.
Discussion
Summary of key findings
Although advances in acute sepsis care have improved survival, life after sepsis has become a significant public health challenge. Many survivors continue to grapple with long-lasting physical, psychological, and cognitive issues, yet these experiences have not been well explored in the Australian context. This scoping review brings together what is currently known about post-sepsis trajectories in Australia, drawing on both peer-reviewed studies and grey literature. The review organises post-sepsis outcomes into six coherent themes: (1) long-term mortality risk, (2) hospital readmissions, (3) reduced health-related quality of life, (4) long-term physical impairments, (5) cognitive dysfunction, and (6) long-term mental health challenges. This thematic structure provides a clear and comprehensive picture of the multidimensional burden faced by sepsis survivors.
Interpretation of the findings and comparison with other studies
This review highlights that a substantial proportion of sepsis survivors face an elevated risk of long-term mortality compared with the general population.57,61 –68 In Australia, 1 year post-sepsis mortality ranged from 12.5% to 36.9% across the included studies,61,63,68 which aligns with international estimates: 22.3% in a French national discharge database analysis 72 and 15% in an observation cohort study in the United Kingdom. 73 Similar trends were also reported in U.S. administrative claims and other settings.16,74 Factors such as older age, indigenous status, higher comorbidity burden, and greater organ dysfunction appear to increase the risk of post-hospital mortality. 64 This finding is aligned with evidence from Denmark 75 and an observational cohort study in the U.K. 73 In addition, evidence regarding sex differences in post-hospital mortality remains inconsistent. Notably, two studies reported higher mortality among male survivors.63,64 This is supported by findings from the U.K., 73 France, 76 and the U.S. 77 Proposed biological explanations include X-chromosome–linked gene expression and oestrogen-mediated modulation of immune response and endothelial function protection to reduce severity and mortality risk in females.78 –80 In contrast, another study in the review reported no sex-based difference in long-term mortality, 67 possibly due to its methodological approach, which deployed a risk-adjusted analysis by stratifying patients by age groups (premenopausal, <50 years vs. older). A prior systematic review supports this finding, indicating that sex had no clear effect on short-term mortality, while female sex may be linked to lower 1-year mortality (OR = 0.83, 95%CI 0.68–0.98). 81 Moreover, the review identified conflicting results in long-term mortality outcomes in Indigenous versus non-Indigenous population groups. Davis et al. 64 found higher long-term mortality, while Hargovan et al. reported similar overall mortality. 65 The higher mortality rates in Aboriginal and Torres Strait Islander people may be attributed to health care access and utilisation disparities, higher alcohol and smoking usage, higher chronic illness burden, and residual confounding.82,83
Australian sepsis survivors experience high rates of hospital readmission, commonly due to recurrent sepsis. In this review, around 40% are readmitted within 30 days and up to 75% within 12 months of discharge. 53 These rates are consistent with international reports: 20%–32% at 30 days, about 40% at 90 days, and more than 40% at 1 year.12,21 –26,29,73 This elevated risk could be due to the increased vulnerability to infections and worsening of chronic conditions following sepsis-related immune dysregulation. 12 Although generated from a single piece of evidence, the review also found a higher readmission risk among males; a cohort across three U.S. states reported a similar pattern, 25 possibly due to sex-based immune differences. 79 Readmissions contribute to higher mortality, longer hospital stays, and greater healthcare use and costs, underscoring the need to identify high-risk groups and strengthen post-sepsis follow-up services. 84
Poor HRQoL is another important concern among sepsis survivors in Australia. This review concluded that HRQoL is substantially impaired after sepsis,58,60,61,63,69,70 consistent with findings from global studies.41–44 Reductions in HRQoL are plausibly driven by persistent inflammation and immune dysregulation, physical limitations, psychological morbidity, and disruptions to social roles. 85 Conversely, some studies in the review reported that the HRQoL of sepsis survivors is comparable to that of other ICU patients,57,62,68 supported by international studies.17,42,86,87 However, prospective studies from Tokyo and the Netherlands reported worse HRQoL among sepsis survivors compared to other ICU cohorts88,89; a discrepancy might be explained by lower baseline HRQoL in those studies, whereas studies included in this review did not account for pre-sepsis HRQoL, limiting direct comparison. Evidence on determinants of HRQoL remains limited, and findings on sex differences remain debatable. Notably, one study found that males had better HRQoL than females, 69 consistent with findings from a Chinese case–control study. 90 This difference may be attributed to lower physical and psychological well-being and less frequent exercise habits among women, which could contribute to reduced HRQoL. 91 Conversely, another cohort study observed no sex-based difference at 12 months. 67
Although under-explored, this review also divulged that sepsis survivors in Australia also experience significant impairments in physical functioning. Approximately half of survivors reported ongoing pain (44.5%–53.5%),54,57 consistent with prior investigations in ICU survivor cohorts.31,92 Persistent pain likely reflects interacting mechanisms, including ongoing inflammation with peripheral and central sensitisation, neuropathic changes related to inflammatory nerve injury, cytokine-mediated alterations in nociception, and sequelae of organ dysfunction and ischaemic injury.30,93 More than half also experienced some degree of fatigue and exercise intolerance,54,57 supported by findings from a prospective cohort at Jena University Hospital, Germany. 94 These outcomes are associated with prolonged ICU stays and immobility, leading to neuromuscular dysfunction and loss of muscle mass and strength. 95 Additional sequelae include self-care deficits, mobility problems, amputations, and other disabilities.54,56,57,60 Collectively, these impairments are associated with loss of independence and concentration, increased health care utilisation, and diminished quality of life. 96
Cognitive dysfunctions are another long-term sequela reported by existing studies in Australia. Consequently, memory loss affected over half of survivors (53.5%), 54 while nearly one-third (29.5%) showed broader cognitive impairment, 60 consistent with expert estimates that 25%–50% of severe sepsis survivors experience significant cognitive deficits.97,98 The proposed mechanisms include cerebral hypoperfusion and ischaemia, blood–brain barrier disruption, neuroinflammation, and neurotransmitter dysregulation.98,99 In contrast, this finding exceeds those reported in some U.S. cohorts (10.6%–18%),100,101 likely reflecting differences in socio-demographic attributes of study populations, assessment timing, and measurement tools. For example, one U.S. study enrolled older, non–critically ill septic participants, 100 whereas Australian studies included mechanically ventilated ICU patients with outcomes assessed within 6 months of discharge, a window that may precede full cognitive recovery.
In Australia, sepsis survivors and their families experience substantial mental health burdens, with anxiety and depression affecting roughly 20% to over 50% of individuals.54,57,60 Estimates are concordant, with reported anxiety prevalences of 32% at 3 months, 40% at 6 months, and 34% at 12–24 months post-sepsis 102 and depression prevalences of 29% at 2–3 months, 34% at 6 months, and 29% at 12–24 months. 103 Contributing mechanisms include neuroinflammation, cerebrovascular injury, neurotransmitter disturbances, and trauma from the ICU experience.12,99,104,105 Difficulty recalling events during the illness and uncertainty about the future may also explain these phenomena.106,107 Although factors such as advanced age, female sex, prolonged ICU stay, baseline mental health status, and post-discharge supportive service status are associated with adverse psychiatric outcomes, 105 herein, this review could not quantify their association in the Australian context.
Evidence gaps of existing studies
Beyond mapping the findings of existing literature, this scoping review identified several important gaps in the Australian evidence base on post-sepsis outcomes. Key domains of post-sepsis syndrome—particularly cognitive, physical, and psychological outcomes—have not been comprehensively explored. Australian evidence on post-sepsis outcomes has prioritised long-term survival over survivors’ well-being. Studies assessing these outcomes frequently relied on proxy or self-reported measures, made limited use of validated assessment tools (e.g., the Montreal Cognitive Assessment [MoCA], Mini-Mental State Examination [MMSE], 6-minute Walk Test [6MWT], Timed Up and Go [TUG], and Short Physical Performance Battery [SPPB]), employed heterogeneous instruments (such as the Hospital Anxiety and Depression Scale [HADS] and European HRQoL measures for mental health assessment), and often involved short follow-up periods, limiting understanding of long-term outcomes.
Secondly, existing studies also insufficiently examine key determinants of long-term sequelae, particularly for the physical, cognitive, and mental health outcomes, and often lack a rigorous analytical approach to control confounders.
Thirdly, use of inconsistent sepsis definitions reduces comparability, interpretability, and generalisability of the findings. Lastly, infrequent assessment of outcomes beyond 1 year potentially underestimates the true burden of post-sepsis sequelae. Reliance on retrospective or cross-sectional designs might introduce misclassification or recall bias, restricting e the robustness of the evidence (Tables 1–6).
Strengths and limitations
The key strength of this scoping review lies in its rigorous and comprehensive search strategy across multiple databases and grey literature, ensuring broad coverage of existing evidence. Nevertheless, some limitations should be acknowledged. First, data extraction by a single reviewer may introduce interpretation bias. Secondly, the broad scope of the review required prioritising the mapping of diverse themes over in-depth exploration of individual domains. Finally, the absence of stakeholder or consumer consultation—an optional but valuable component of JBI scoping review methodology—may limit the translation of findings into practice, particularly in relation to post-sepsis care needs.
Implications and future directions
Understanding the long-term trajectories and lived experiences of adult sepsis survivors is essential for strengthening post-sepsis care pathways. This scoping review demonstrates that sepsis survivors in Australia experience substantial long-term challenges, including increased mortality and persistent multidimensional sequelae, underlining that sepsis is a life-altering condition rather than a time-limited acute illness. Findings from the included grey literature simultaneously indicate that post-sepsis care remains poorly planned and insufficiently implemented, largely because the health system remains focused on the acute hospital management of illness.52 –54 For example, an online survey conducted in Queensland reported that 68.7% of respondents felt family circumstances were overlooked at discharge, 57.2% received insufficient guidance on managing post-sepsis syndrome, and 62.2% were not informed about warning signs of deterioration. 54 Collectively, these findings underscore the need for clinical practice, research, and health system responses to extend beyond hospital discharge. This suggestion is also supported by a national recommendation by Sepsis survivors in Australia, ACSQHC, and the George Institute of Global Health, underscoring that rehabilitation service should commence during hospitalisation, be incorporated into discharge planning and strengthen individualised and structured follow-up service settings46,55,108
Conclusions and recommendations
The scoping review concluded that sepsis survivors in Australia experience substantial long-term complications and elevated mortality risk. These findings highlight the need for greater stakeholder emphasis on the design of a coordinated, culturally safe, and person-centred rehabilitation service supported by scalable care models, improved awareness, and sustained engagement of survivors, families, and primary care providers. Moreover, inconsistencies in sepsis case definitions, the absence of validated outcome measurement instruments, short follow-up periods, and inadequate exploration and adjustment for key determinants highlight the need for robust, standardised, and well-designed longitudinal studies to better characterise the breadth and depth of PSS outcomes and to inform targeted intervention strategies.
Supplemental Material
sj-docx-1-inc-10.1177_17511437261456097 – Supplemental material for Trajectories of sepsis survivors in Australia: A scoping review
Supplemental material, sj-docx-1-inc-10.1177_17511437261456097 for Trajectories of sepsis survivors in Australia: A scoping review by Berihun Bantie, Anteneh Mengist, Jacqueline H. Stephens and Diane Chamberlain in Journal of the Intensive Care Society
Footnotes
Abbreviations and acronyms
ACSQHC- Australian Commission on Safety and Quality in Health Care; AIHW- Australian Institute of Health and Welfare; AKI- Acute Kidney Injury; CKD- Chronic Kidney Injury; CLD- Chronic Liver Disease; CVD- Cardiovascular Disease; ICU- Intensive Care Unit; OSF- Open Science Framework; PCC- Population, Concept, Context; PSS—Post-Sepsis Syndrome; PTSD - Post-Traumatic Stress Disorder; HRQoL- Health-Related Quality of Life; PRISMA-ScR - Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews; RCT: Randomised Control Trials; U.K.- United Kingdom; U.S.- United States; WHO- World Health Organisation.
Ethical considerations
As the study involves the synthesis of publicly available data and does not involve human participants, ethics approval was not required. Indeed, the review protocol was registered to ensure transparency and methodological rigor.
Consent to participate
There are no human participants in this article, and informed consent is not required.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Open science framework (OSF) registration
Data availability statement
The manuscript and its supplementary materials contain all the information used to draw the conclusions. No new datasets were generated for this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.