
Abstract
Background:
Appropriate antibiotic use can save life in sepsis while reducing the risk of bacterial resistance. Biomarkers, such as procalcitonin (PCT), can inform the timing of the clinical decision to stop a course of antibiotics. The recently reported multicentre ADAPT-Sepsis trial showed that a daily PCT-guided protocol can safely reduce the duration of antibiotic use in people with suspected sepsis. This linked study aimed to identify potential barriers and facilitators to implementation of PCT testing.
Methods:
This process evaluation collected qualitative and quantitative data from clinical teams involved in the delivery of adapt-sepsis. Trial site staff were invited to complete a questionnaire and to participate in a semistructured interview. Responses were thematically analysed and compared with constructs from the Consolidated Framework for Implementation Research (CFIR v2.0).
Results:
A total of 69 staff from 26 critical care units responded to the online questionnaire (n = 55); the interview invitation (n = 3); or both (n = 11). Interviewees included critical care consultants, junior doctors, and research nurses. At least 60% of ADAPT-Sepsis trial staff respondents supported the continuation of PCT testing, even before trial results were publicised. Several of the implementation facilitators related to factors evident at the level of the site/organisation, such as microbiology involvement and increasing access to knowledge and information about evidence supporting the tests. Cost was raised as a potential barrier.
Conclusion:
Adoption of biomarker tests such as PCT may be facilitated by communicating high-quality evidence, supported by staff focussed on antimicrobial stewardship. Cost implications have been considered in a related economic analysis.
Study registration:
This study was prospectively registered online. The unique identifying number at researchregistry.com is researchregistry4244.
Introduction
Patients presenting to hospital with suspected sepsis are started on a course of antibiotics as early as possible, due to the severity of the illness and potential for rapid deterioration. However, overuse of antibiotics contributes to bacterial resistance, therefore it is important to stop antibiotics as early as it is safe to do so. Procalcitonin (PCT) is an inflammatory biomarker related to bacterial infection and can be readily measured in routine hospital service laboratories from blood samples. PCT measurements are one of many factors which clinicians may consider when deciding when to stop prescribing antibiotics in people with sepsis.
At present, PCT-guided antibiotic prescribing has not been universally adopted. Ten years ago, NICE guidance on PCT testing for diagnosing and monitoring sepsis concluded that there was insufficient evidence to recommend routine adoption. 1 Their Diagnostics Advisory Committee recommended that “robust evidence is generated to show the impact of adding procalcitonin testing to standard clinical practice in the NHS, to guide the use of antibiotic treatment in people with confirmed or highly-suspected sepsis in intensive care units.” 1
The ADAPT-Sepsis trial (Biomarker-Guided Duration of Antibiotic Treatment in Hospitalised Patients with Suspected Sepsis) investigated adults with suspected sepsis admitted to 41 critical care units throughout the UK NHS between January 2018 and June 2024, with an aim to establish whether biomarkers could safely inform early discontinuation of antibiotics without increasing mortality. The three-arm trial compared daily PCT-guided and daily C-reactive protein-guided (CRP) protocols against a pragmatic definition of “standard care” which varied between hospitals. 2
A unique feature of the trial design was that intervention allocation was concealed from clinical teams making prescribing decisions, with laboratory staff communicating carefully worded automated advice instead of the specific biomarker values that they might normally have access to in real-world practice (Table 1). Dark et al. 3 concluded that care guided by daily measurement of PCT levels leads to a safe reduction in antibiotic prescribing duration compared with standard care. There was a significant reduction in antibiotic duration from randomisation to 28 days for those in the daily PCT-guided protocol compared with standard care (mean duration, 10.7 [SD, 7.6] days for standard care and 9.8 [SD, 7.2] days for PCT; mean difference, 0.88 days; 95% CI, 0.19–1.58, p = 0.01).
ADAPT-Sepsis trial biomarker-guided antibiotic discontinuation protocol. 3 The standard care group underwent no additional testing, and a daily message was communicated to the clinical team that the protocol supports standard care. For the PCT and CRP group, PCT or CRP were measured daily and tailored advice communicated to the clinical team according to biomarker levels as shown in the table.
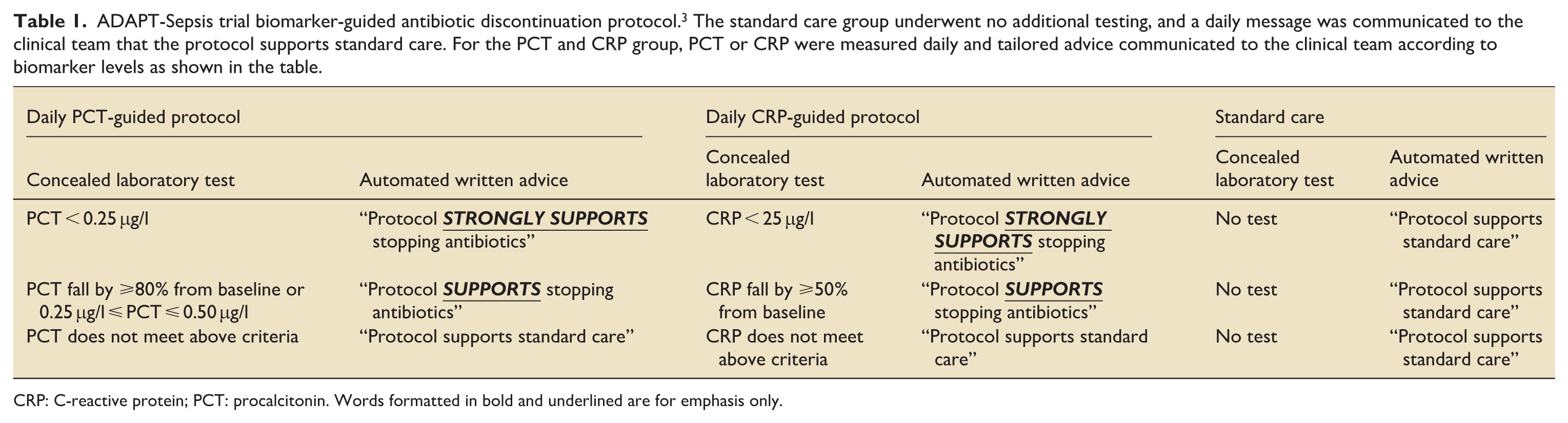
CRP: C-reactive protein; PCT: procalcitonin. Words formatted in bold and underlined are for emphasis only.
In light of this new evidence, it is important to explore the context and potential mechanisms involved in the implementation of daily PCT-guided antibiotic prescribing. In an earlier review, we used Qualitative Content Analysis to retrospectively explore factors influencing decision-making in published trials of PCT-guided antibiotic prescribing protocols for treatment of patients with suspected sepsis. 4
To complement the ADAPT-Sepsis effectiveness trial, we carried out a prospective mixed-methods process evaluation study (PREADAPT-Sepsis). The Medical Research Council defines a process evaluation as a “study which aims to understand the functioning of an intervention, by examining implementation, mechanisms of impact, and contextual factors.” 5 We aimed to capture the experiences of trial teams during delivery of ADAPT-Sepsis, and to gain a deeper understanding of complex decision-making processes associated with antibiotic discontinuation in critical care. In this paper, we explore how our findings could inform real-world implementation of PCT-guided antibiotic prescribing.
Methods
The Consolidated Criteria for Reporting Qualitative research (COREQ) checklist was used to guide the development of this manuscript. 6 Research Ethics Committee (REC) review is not normally required for research involving NHS staff recruited as research participants by virtue of their professional role. The PREADAPT-Sepsis process evaluation was considered to satisfy the criteria of a “non-REC” research project 7 and was formally approved by the Health Research Authority (HRA) and Health and Care Research Wales (HCRW) in February 2019. The study was prospectively registered online with the Research Registry. The unique identifying number is ResearchRegistry4244. 8
Study design
This process evaluation was conducted alongside the ADAPT-Sepsis randomised controlled trial.2,3 It was designed to identify barriers and facilitators affecting implementation of PCT-guided antibiotic prescribing protocols, including the influence of culture and context. The Consolidated Framework for Implementation Research (CFIR) was used to structure our approach. CFIR is a well-established framework which brings together multiple constructs and domains to explain what works, where, and why, in different contexts. 9 Data were collected through an online questionnaire and semi-structured interviews. These were both designed with reference to relevant constructs from CFIR v1.0 9 and revised in accordance with CFIR v2.0. 10
Online questionnaire
We developed a bespoke 32-item online questionnaire using Microsoft Forms. The format included Yes/No and multiple-option tick boxes, free text and Likert scales. It included questions about participants and standard care where they worked, their experience of being involved in the ADAPT-Sepsis clinical trial, and about PCT testing to inform decision-making. The content was piloted using a paper questionnaire at an in-person ADAPT-Sepsis Investigator Meeting in July 2022. Once finalised, a link to access the online questionnaire was distributed by the trial team by email, and sent multiple times to all sites currently participating in the ADAPT-Sepsis trial. Data on the number of individuals given the opportunity to take part were not collected, and all questionnaire respondents were self-selected. Informed consent was implied.
Semi-structured interviews
The semi-structured interview topic guide was developed and adapted in response to suggestions from key stakeholders; the guide was not shared with interviewees. Questionnaire respondents could provide their contact details if they were willing to be invited to an interview, or could opt to remain anonymous and complete only the questionnaire. There was also an option to provide contact details for interview without completing the questionnaire. Although a purposive sampling strategy had been planned for the interviews, low numbers of respondents led to a convenience sampling method being adopted. All those who volunteered to be interviewed were able to take part. All interviews were conducted by the lead author (RLP) whilst the trial was in progress (see Supplemental Materials for more details about the background and training of study researchers).
Formal consent was sought from participants before each interview commenced, and was documented by the researcher. Interviews were conducted and recorded using Microsoft Teams. Audio-transcription of interviews was carried out by the research team; field notes were not taken. None of the interviews were repeated and transcripts were not shared with participants.
Analysis
Quantitative data from the questionnaire was analysed using simple descriptive statistics. Free text responses were imported into NVivo (v14) for qualitative analysis. Together with the questionnaire free text, all interview transcripts were analysed by a single researcher (CL) using reflexive thematic analysis, following the six-phase analytical process: (1) data familiarisation was achieved through multiple readings of transcripts and listening to interview recordings, on the second read of each full transcript, these were highlighted and annotated and brief notes were made for each individual transcript. (2) data was coded systematically using NVivo (v14), initial coding was conducted between July and August 2024, code names were reviewed and discussed with RLP. (3–6) Initial themes were generated by CL and discussed in terms of their wording and explanation with RLP in in-person meetings between September and October 2024. Initial themes were then presented to PD, RL, and AH. Themes were reviewed and refined during further discussions between CL and RLP and throughout the writing of the report.
We incorporated elements of both inductive (themes were generated iteratively during coding) and deductive reasoning (viewing findings through the lens of CFIR). Although it had not been possible to purposively sample interview participants, we were satisfied that data had been collected from a range of trial staff from different organisations. As highlighted by Braun and Clarke11,12 reflexive thematic analysis does not require quantifiable data saturation nor coding reliability testing.
This study applied a critical realist approach to understanding the experiences of clinicians’ decision-making processes associated with antibiotic discontinuation in critical care. 13 Data from the questionnaire and from interviews were integrated using triangulation, as compatible with a critical realist lens, to deepen understanding and explore different facets of the research questions. 14 After viewing descriptive statistics and conducting thematic analysis, the identified themes and sub-themes were systematically mapped against the domains and constructs of CFIR.
Results
Participants
A total of 69 people who had been involved in delivering the ADAPT-Sepsis trial either responded
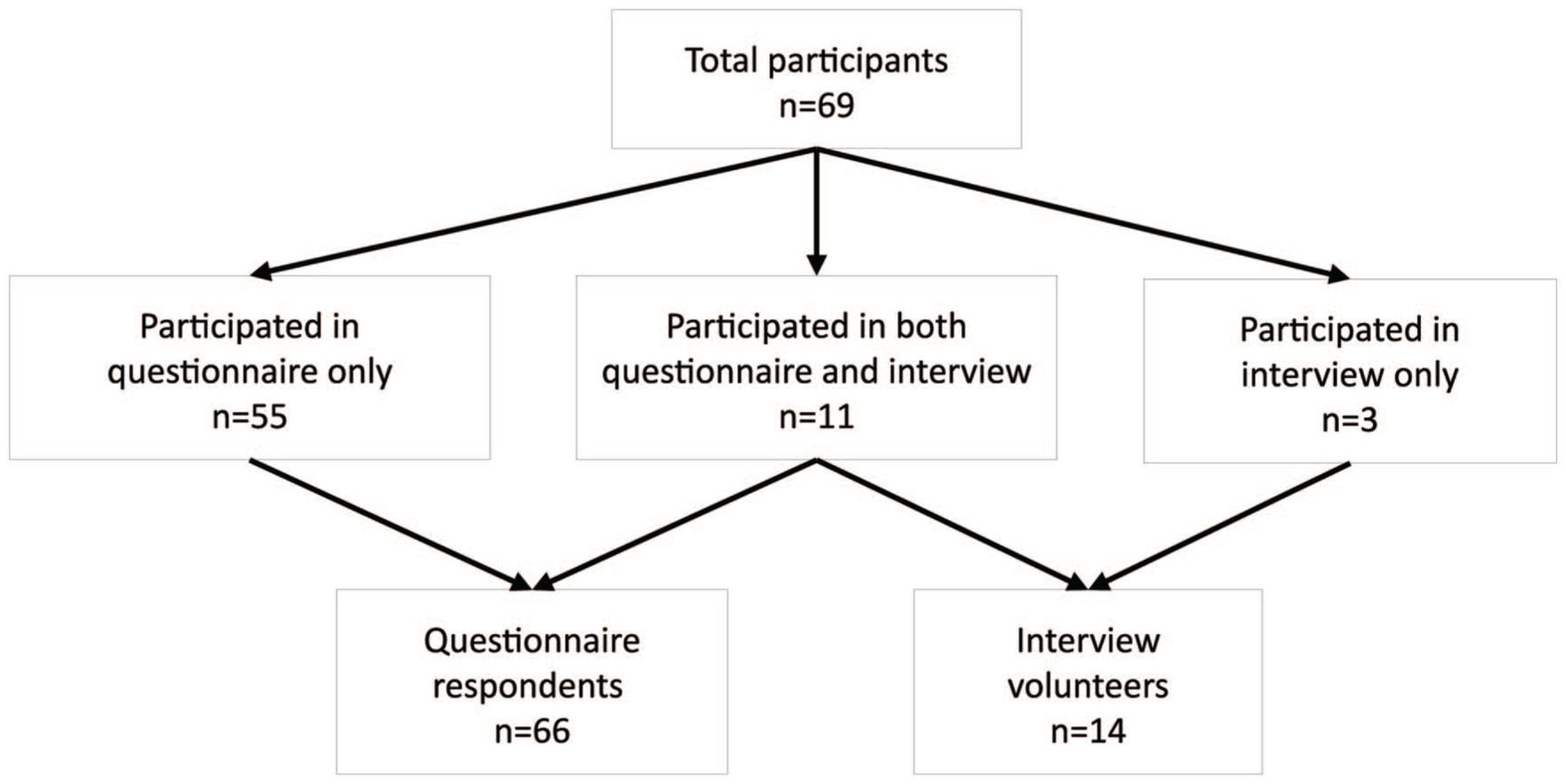
Number of trial staff who completed a questionnaire and/or participated in an interview.
Semi-structured interviews were carried out between September 2022 and July 2023 with 14 participants. Interviews ranged in length between 27 and 56 min, with a total of 613 min of recordings. Interview participants were from 11 hospitals in England. Eight of the interviewees were Consultants (critical care or medical), some of whom were Principal Investigators of the ADAPT-Sepsis trial; the remainder were research nurses or junior doctors.
Integrated findings
Three key themes were developed from an integration of questionnaire and interview data: (1) Pathfinding in antibiotic prescribing: biomarkers as a potential handrail; (2) Local antibiotic prescribing culture; and (3) The future of PCT in antibiotic prescribing. Exemplar quotes corresponding with each theme are available as a Supplemental File.
Theme 1: Pathfinding in antibiotic prescribing for sepsis: Biomarkers as a potential handrail
Participants discussed the many pieces of information they consider when making decisions around antibiotic prescribing. In addition to biomarkers, they mentioned: the patient’s breathing rate, heart rate, temperature, blood pressure, and sputum colour; results from blood tests, urine tests and imaging; other medications being taken; change in condition; the potential origin of the infection, and measures being taken to control the infection at source. There were differences in how clinicians weighed the evidence from PCT tests within the overall clinical picture, with many considering it “another tool” “to be used in conjunction” with other information (questionnaire participant #38) and others “almost completely guided by a PCT drop as a marker of stopping antibiotics” (I3S60).
Staff had varying levels of experience in utilising PCT testing outside of the ADAPT-Sepsis trial. In the questionnaire, 45% of respondents reported that PCT is routinely used to inform antibiotic duration as part of standard care for patients with sepsis or suspected sepsis where they work. Those who reported using PCT testing routinely outside of the ADAPT-Sepsis trial had more positive perceptions about the benefits of the biomarker being sensitive, specific, accurate or having an appropriate response profile to facilitate timely decisions. The evidence for using PCT testing to inform antibiotic prescribing was often filtered through the lens of interviewees’ own experiences, beliefs and attitudes, with some “wedded” to PCT testing (I3I01 and I3S17), while others retained caution in its use.
Clinicians were generally positive about the opportunity for improved objectivity in antibiotic prescribing presented by PCT.
. . .if biomarkers are able to be a kind of handrail to help ensure that antibiotic prescribing is appropriate and is the, is the right thing and you're doing the right things at the right time then that would be excellent. (I3S17)
In this quote (I3S17), biomarkers are suggested as a potential “handrail” for antibiotic prescribing. Handrails provide support and guidance but are not the only influence on the direction of travel. In a similar way, biomarker values might be used to support and guide decision making with evidence-based guidance, other contextual information, and previous experiences also influencing their path.
Healthcare professionals in the ADAPT-Sepsis trial reported that having numerical biomarker results may been more influential in clinical decision making than the advice statements. Numbers are a “hard, fast piece of evidence” (I3S54), potentially inspiring more confidence (I3S33) or faith (I3S55) than the advice. They enable tracking of trends in results over time, supporting clinicians’ autonomy in decision making.
I think that [doctors] like to see the results and it provides them with reassurance and autonomy. . . (I3S07)
Tempering this optimism about the potential for biomarkers to influence antibiotic prescribing, there were suggestions that there could be improvements made on the clarity of thresholds in PCT protocols and more information available on the ideal frequency for testing. There were some concerns raised about potential “noise” (I3S03) from over-testing, over reliance on a single measure, or PCT being used inappropriately during the diagnosis of sepsis.
Sub-theme 1a: Uncertainty in the utility and limitations of PCT in specific clinical scenarios
Clinicians expressed uncertainty regarding the utility of PCT for certain patients, specifically those with pancreatitis, burns, major abdominal surgery, or intra-abdominal infection. PCT was considered preferable to CRP for patients treated with Interleukin-6 Antagonist as treatment for Covid-19. The trial exclusion criteria were adapted accordingly.
Sub-theme 1b: Logistical and economic influences on PCT testing
Several logistical factors were considered to influence the potential for real-world implementation of PCT-guided antibiotic prescribing in critical care. Sites varied in their access to PCT testing prior to the trial, with some reports of the test being available “very early, predating this study” (I3I04), some began to have access “at the time of Covid” (I3S03) while in other sites PCT testing was only made available because of the ADAPT-Sepsis trial.
The geographical location of laboratories was thought to impact processing time and therefore the potential for using this information to make timely prescribing decisions. Off-site laboratories may have contributed to a delay in receiving results. Outside of the trial context, estimated time intervals between sending blood samples and receiving PCT results ranged from around 45 min (if the laboratory had been prompted) to within 24 h. The interval would be affected by how closely the sample collection corresponded with the scheduled PCT run in the laboratories, which in one example was reported to occur once a day. The potential impact of the result on decision making would be influenced by timeliness of receipt ahead of ward rounds, and the availability of microbiologists at the appropriate time.
The cost of PCT was discussed as a potential barrier to real-world implementation, although some participants reported that its cost had reduced over time. It was suggested that the cost could be considered in comparison to other interventions used to improve the treatment of sepsis in intensive care.
Theme 2: Local antibiotic prescribing culture
Participants discussed the culture where they worked and how this might influence antibiotic stewardship. Factors such as prescribing norms, policies, team composition, and interactions between staff and between disciplines were key influences. This is summarised in a quote below (I3I01).
So, I think what you're planning to do – what you've always done; what your unit’s policy is; what your unit’s culture is; what your microbiology culture/input is (microbiology culture in terms of practice rather than results) – it remains the single biggest driver of antibiotic prescribing and is probably the hardest thing to influence. (I3I01)
There were a range of approaches in local antibiotic prescribing, with some reporting that they consistently aimed to stop (considering themselves a unit that prescribes short courses), while others reported an inclination to finish the course of antibiotics. Clinicians who had been practising in the same unit for a long time were sometimes uncertain how use of PCT testing in their unit might compare to other units. If we consider PCT testing in terms of the diffusion of innovations, 15 communication channels discussed in interviews included the rotation of senior trainees, the merging of hospital trusts and the potential for comparing publicly available hospital guidelines or learning at conferences.
Sub-theme 2a: Hands and weeks: Prescribing units
. . .probably somewhere between 5 and 10 days, based on the number of digits in one hand and the number digits in both hands rather than any science I would suggest (but I think that's what everyone does). (I3I03)
The survey asked how long patients with sepsis or suspected sepsis would normally be prescribed antibiotics for, the most frequently cited figures were 5, 7, 10, and 14 days. These figures were also referred to in interviews, as the “default length” (I3S54) or standard care. When providing a rationale for these durations, clinicians considered that this was largely determined by historical practice, habit and the prevailing western numerical culture of working in factors of 10 and considering time in units of weeks. There was variation in how frequently the antibiotic treatment would be reviewed, with estimates including daily, every 48 h or at the end of a 5-day treatment period.
Sub-theme 2b: Multi-disciplinary teams influence prescribing culture
There was wide variation of the integration of roles within multi-disciplinary teams (MDT) and how decisions were influenced by MDT members. Roles discussed in terms of their input to antibiotic prescribing decisions included microbiologists, pharmacists, intensive care consultants, nurses, “parent” teams, infectious diseases teams, Advanced Critical Care Practitioners (ACCPs), and physiotherapists. The expert support provided by microbiology was highly regarded. Where roles were well integrated into the MDT, such as having a physical presence on ward rounds on a regular basis, this appeared to contribute to a learning culture where decision making could be explored as a joint enterprise which takes into account the expertise of all team members.
Theme 3: The future of PCT testing in antibiotic prescribing
Participants discussed the future of PCT testing to support antibiotic prescribing and were interested in the outcomes of the ADAPT-Sepsis trial. In some cases where the use of PCT was already embedded in routine practice outside of the context of the clinical trial, staff considered that the biomarker would continue to be used regardless of the results of the trial. More than 60% (40/66) of questionnaire respondents agreed that they would probably support continuation of routine procalcitonin testing after the trial. In general, clinicians reported that they were willing to align their practice with the clinical evidence, despite the trial results not yet being available at the time of data collection. Potential enablers to support changing practice were reported as: timely published evidence; updating standards of care either locally or nationally through NICE or General Medical Council (GMC) guidance; further education for clinicians; a clear economic case to support the use of PCT testing; and additional involvement of the microbiology team.
Relationship with established implementation theory
Mapping study findings against CFIR constructs revealed that many areas of the theoretical implementation framework were relevant (Table 2). The Framework’s Inner Setting domain seemed particularly pertinent with respect to potential facilitators to changing practice. This is defined as “The setting in which the innovation is implemented,” and can be applied at the level of the organisation/hospital or critical care unit. 10
Identified themes mapped against domains and constructs of the Consolidated Framework for Implementation Research (CFIR). 10
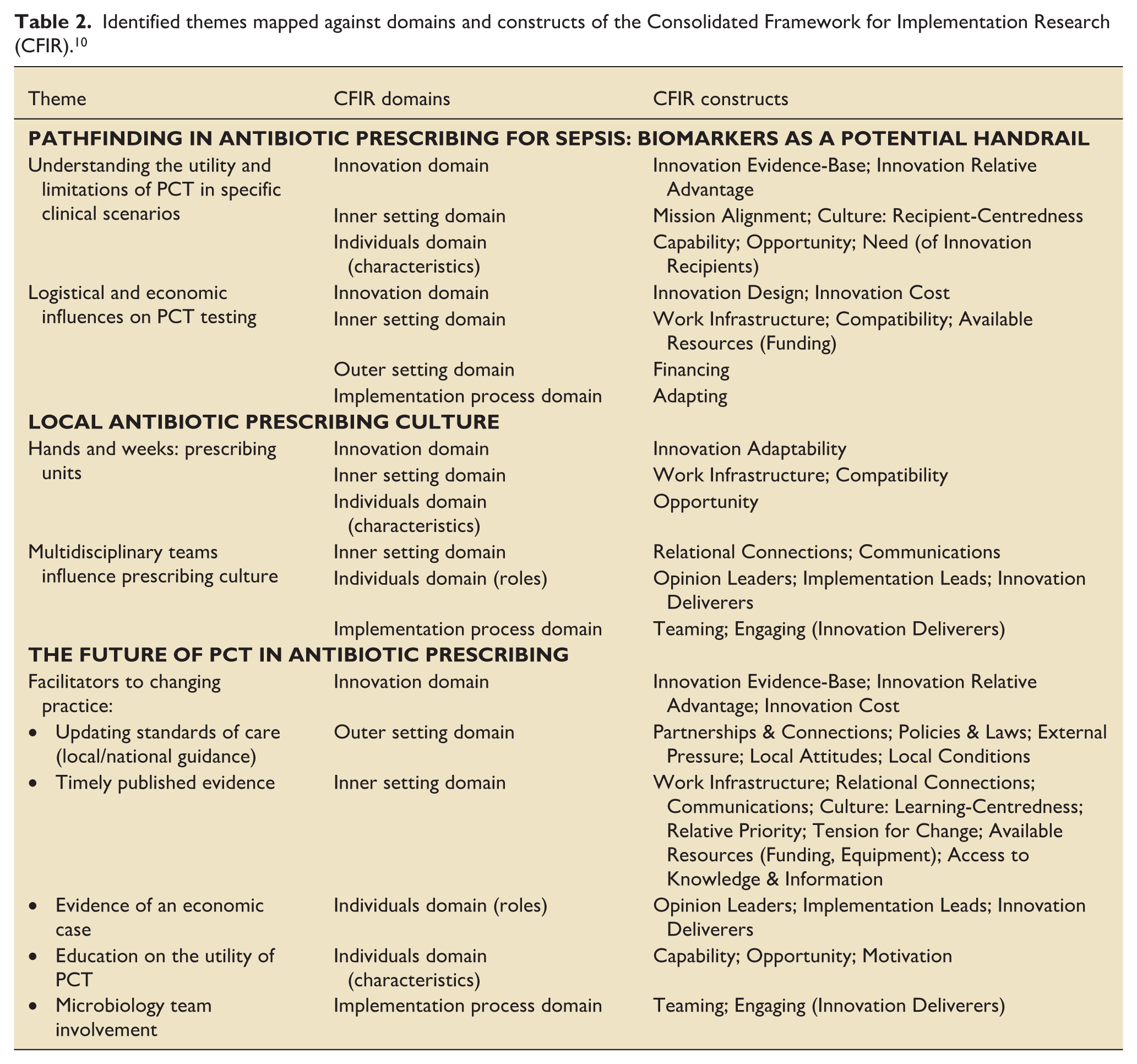
This exercise indicated that more widespread implementation of PCT testing could be facilitated by:
Increasing access to information about the innovation evidence-base and the relative advantages of PCT testing
Promoting the role of microbiologists as opinion leaders and advocates for the value of PCT testing as a tool to improve antibiotic stewardship
Engaging and educating MDT staff through relational connections and clear communications
Encouraging a learning-centred approach and openness to change
Making an economic case for the provision of associated resources (equipment, staff, educational materials).
Discussion
Many complex factors influence antibiotic prescribing decision-making processes in critical care.16,17 With recent empirical and anecdotal evidence being favourable towards the use of PCT-guided protocols to safely reduce the duration of antibiotic prescribing; the research emphasis is shifting from “Should PCT testing be implemented?” to “How should PCT testing be implemented?”. The uptake of PCT testing has previously been hindered by insufficient published implementation studies.18,19 In our study, staff at the front line of trial delivery provided rich insights into their perspectives on the value of protocols for PCT-guided prescribing in the care of patients with suspected sepsis. Our exploration of barriers and facilitators enhances the limited literature available by providing additional insights into approaches to implementation, which could inform knowledge translation strategies on a wider scale.
Engagement of microbiologists and other members of a MDT was identified as a key facilitator in our study. Implementation of a PCT-guided prescribing protocol is reportedly more successful when supported by an antibiotic stewardship team approach than when a protocol is implemented without this additional support. 20 From another perspective, the self-efficacy (professional autonomy) of clinicians at a single site in Ireland was proposed as potential barrier to implementation. 19 Around 76% of UK critical care units have a dedicated microbiologist or infectious disease specialist, with almost half providing daily input. 21 However, this requires adequate staff resourcing, which may not always be available in smaller hospitals. 22
Even when persuasive evidence is available, results need to be disseminated and understood by those able to enact change in real-world settings. In their exploration of attitudes associated with rapid diagnostic tests for respiratory illnesses, Burrowes et al. 23 found that “the mere provision of testing materials and guideline information is not enough to see appreciable differences in care. Providers need clear evidence that supports using the test will result in improved clinical outcomes.” Our study participants described how evidence was filtered through the lens of their own personal experiences, and those who had previously encountered PCT testing outside of the trial context had more positive views about its benefits. Stewart et al. 24 advocated for “behaviourally intelligent” approaches to the implementation of guideline-based solutions to antimicrobial resistance. In common with our findings, they concluded that lessons learned from prior experience and interactions with other people are important influencing factors to be considered in addition to conventional biomedical evidence.
Strengths and limitations
This process evaluation had the advantage that it was conducted by researchers that were independent of the main ADAPT-Sepsis trial. This may have encouraged openness and honesty from participants (whose identities were concealed from the main trial team), and reduced bias in interpretation of findings. We were able to recruit a range of healthcare professionals from multiple sites, facilitating assessment within differing antibiotic prescribing cultures. However, recruiting participants on a voluntary basis carries the risk of selection bias; we were unable to individually identify those who did not respond to our invitation and are therefore unable to confirm whether the sample was representative of the whole critical care community.
Whilst our aim had been to identify potential barriers and facilitators to implementation of PCT testing, data collection for our process evaluation took place within the context of a blinded randomised clinical trial. The trial took a pragmatic approach to defining standard care, although use of PCT testing in the standard care arm of the trial was considered a protocol violation (reported as a very infrequent event). 3 Automated trial blinding mechanisms were also used to conceal allocation to the three trial arms and clinicians were not able to view absolute levels of biomarkers, nor to observe changes in these levels as each patient progressed through their clinical course. As such, our findings may not be directly realisable in a real-world scenario. A further specific implementation study may be worthwhile.
Unlike the three-arm ADAPT-Sepsis trial, this process evaluation focussed in particular on PCT testing. This was because we intended to provide evidence to inform a potential revision of NICE guidance. 1 There is scope for additional qualitative research which encompasses a broader range of biomarkers.
Conclusion
Critical care professionals are generally in favour of PCT testing to guide antibiotic prescribing discontinuation in adult patients with sepsis when viewed as an adjunct to other indicators of infection and sepsis resolution. Widespread implementation may be facilitated by communicating high-quality evidence of safety and effectiveness, and the support of dedicated antimicrobial stewardship staff. A recently published economic analysis 25 may help to address some of the barriers to implementation.
Supplemental Material
sj-docx-1-inc-10.1177_17511437261458968 – Supplemental material for Implementation of procalcitonin-guided antibiotic stopping advice in sepsis: A mixed-methods process evaluation in a clinical trial context
Supplemental material, sj-docx-1-inc-10.1177_17511437261458968 for Implementation of procalcitonin-guided antibiotic stopping advice in sepsis: A mixed-methods process evaluation in a clinical trial context by Ruth Louise Poole, Christina Lloydwin, Harley Anderson, Paul Dark, Ranjit Lall, Anower Hossain and Judith White in Journal of the Intensive Care Society
Footnotes
Acknowledgements
The authors would like to thank Professor Bronagh Blackwood for her support during initial development of the process evaluation protocol, as well as CEDAR staff Dr Susan O’Connell, Dr Helen Morgan and Michael Beddard for searching and reviewing the literature. We are also grateful to Warwick Clinical Trials Unit for facilitating participant recruitment. Particular thanks go to the ADAPT-Sepsis site staff who volunteered their time as study participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CEDAR researchers were supported through a contractual agreement with the National Institute for Health and Care Excellence (NICE). RLP received additional research funding from the Intensive Care Society through a New Investigator Award. PD was funded by NIHR Manchester Biomedical Research Centre and a NIHR Senior Investigator award.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Study registration
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.