
Abstract

Dear Sir,
We present a modified technique (Fig 1) of dental wire fixation for spiral/oblique metacarpal and phalangeal fractures, and compare it to other techniques of dental wire fixation. The periosteum is reflected and the fracture is reduced. A 1 mm K-wire on a power drill is used to drill a hole through the cortex on each side of the fracture (Fig 1A). A single interosseous 0.35 mm dental loop wire is passed through the drill holes and twisted once to make the ‘first’ knot. The long wire end is then passed around the bone in a cerclage fashion and twisted again to make the ‘second’ knot. Hence, we named this technique the ‘double’ knot technique (Fig 1B). Alternatively, the same technique may be used without making the ‘first’ knot and hence the term ‘single’ knot technique (Fig 1C). The fixation is always supplemented with one or two simple cerclage dental wires (size 0.4 mm or 0.45 mm). The twisted wire ends are turned laterally to avoid impinging on the extensor tendon. A light dressing is applied. No splint is used and mobilisation of all joints is started immediately after surgery. The technique was used in nine patients (six fractures of the proximal phalanx and three metacarpal shaft fractures) with satisfactory results. There were no complications such as infection, loss of reduction, nonunion or need for wire removal. The mean total active motion (TAM, normal = 260°) was 257° (range = 245–260°).
The new technique.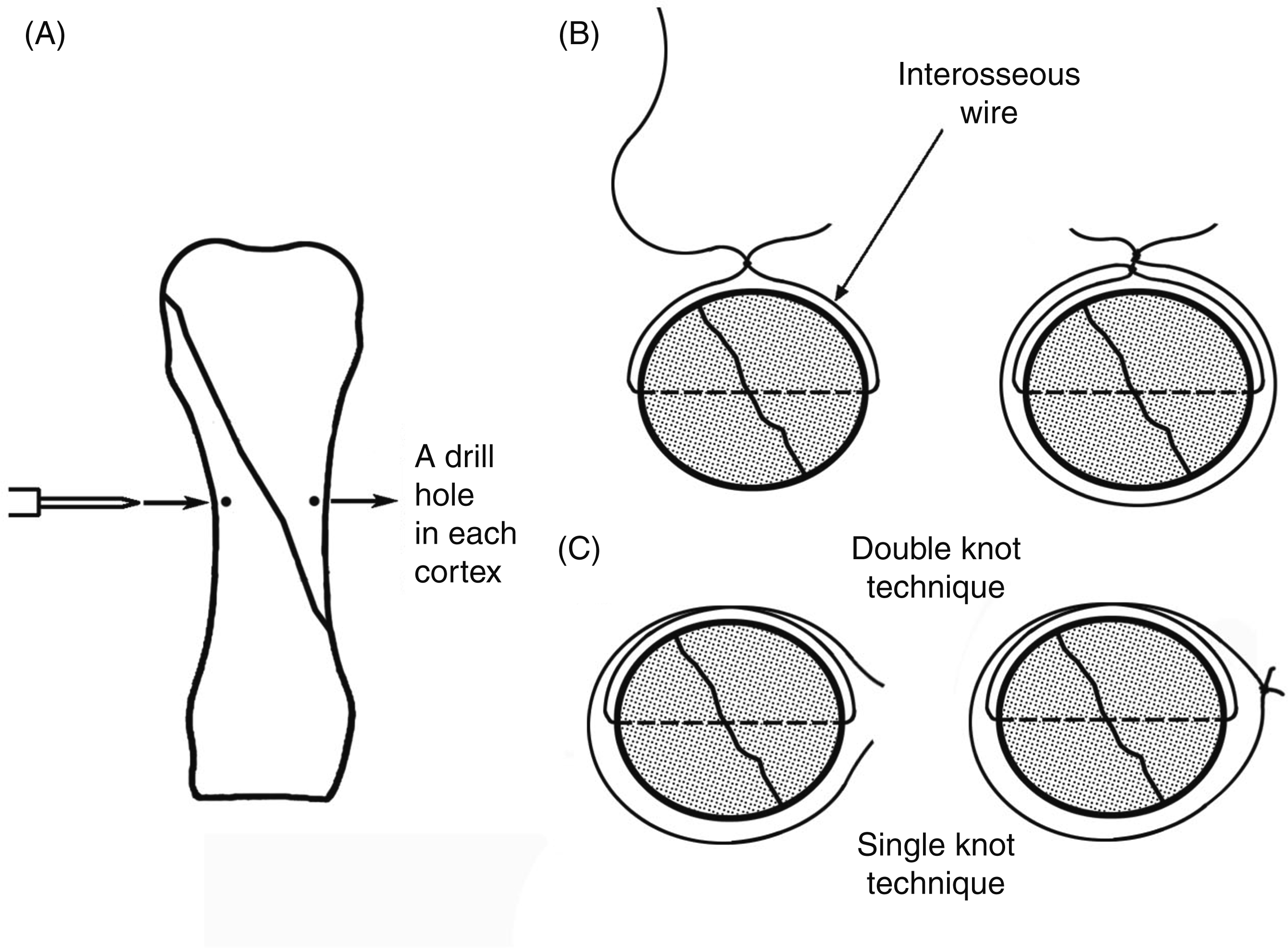
Dental wire fixation for spiral/long oblique fractures is generally used in cerclage rather than a loop configuration (Fig 2). A major problem with cerclage fixation is the risk of wire migration with early postoperative mobilisation. The shape of the metacarpal and phalanx should be taken into consideration in respect of possible migration. The shaft is fairly thick proximally and distally, but remains thin, with a relatively constant diameter, in the mid-shaft. Therefore, simple cerclage wire (Fig 2A) migration does not tend to occur if the fracture is located and the wires are placed along the mid-shaft (Al-Qattan and Al-Lazzam, 2006; Al-Qattan and Al-Zahrani, 2008). However, cerclage wire migration towards the mid-shaft may occur after tightening in fractures located in the proximal or distal parts of the shaft. In these cases, three different techniques have been suggested to minimize the risk of migration. In the first technique (Gropper and Bowen, 1984), the wire sits in a groove scored in the cortex with a side-cutting burr (Fig 2B). This complicates the technique as slippage may still occur with immediate postoperative mobilisation. Hence, Gropper and Bowen (1984) recommended an initial period (10–14 days) of immobilisation. In the second technique (Al-Qattan, 2008), a unicortical loop wire is inserted first followed by simple cerclage wire application (Fig 2C). Migration is not prevented completely but it is minimised because the unicortical loop wire will block significant migration towards the mid-shaft. Finally, for fractures with multiple cortical splits, simple cerclage wires may be used first to maintain the reduction, thus providing sufficient initial stability for placement of a plate and screws as shown in Fig 2D (Teoh et al., 2006). The plate and screws complicate the technique but will prevent cerclage wire migration.
The use of dental wires for spiral/long oblique fractures.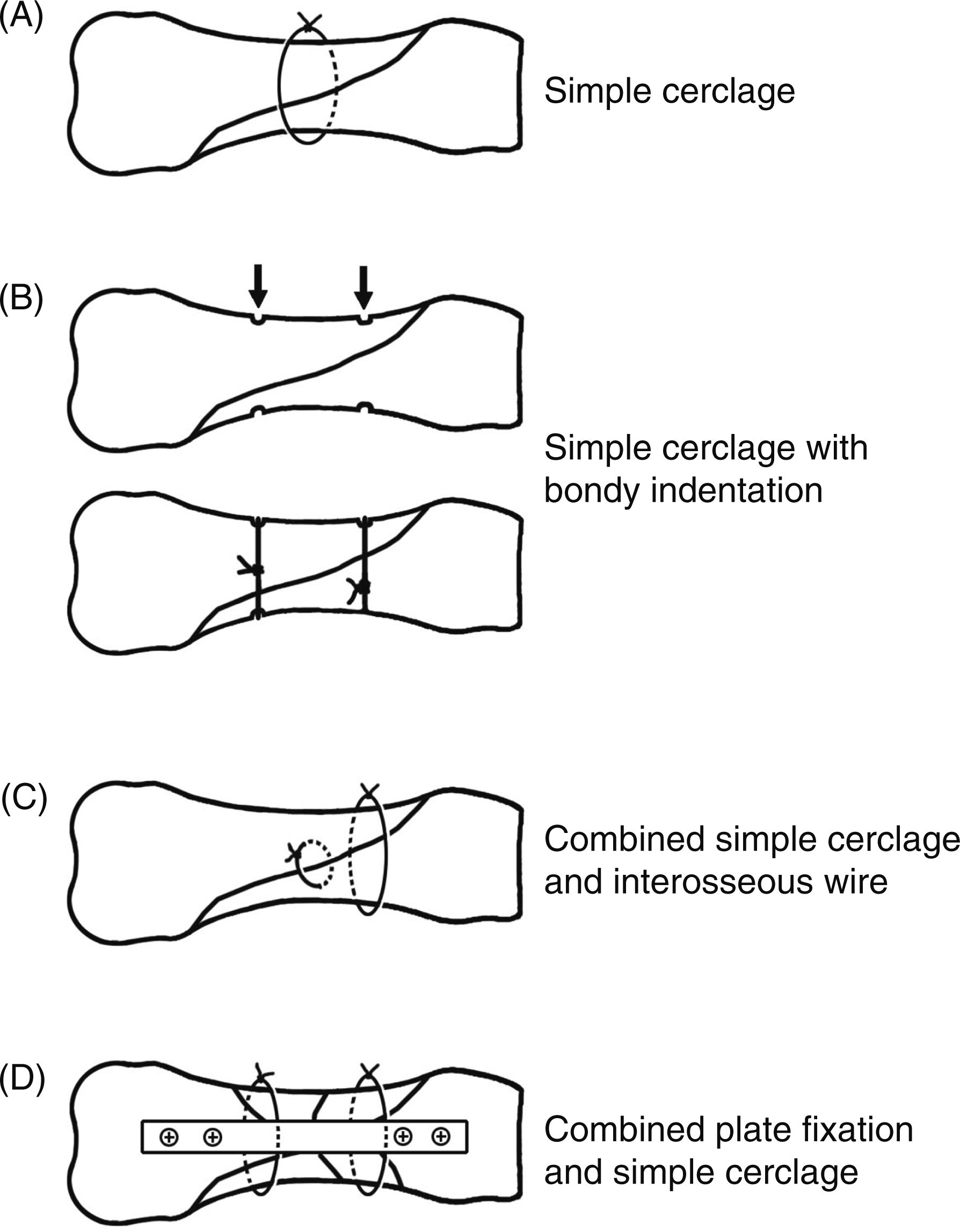
The single or double knot technique of cerclage wire fixation has the major advantage of complete prevention of wire migration and hence there is enough stability to allow immediate postoperative mobilisation. Furthermore, it is relatively simple compared to supplementary scoring or plate fixation. Finally, the ‘knot’ cerclage wire will minimise axial migration (shortening) at the fracture site and will block migration of supplementary simple cerclage wires applied at the thicker part of the shaft.