
Abstract
Reconstruction of grip in tetraplegia aims to improve upper extremity performance and control in daily life. We evaluated the effects of surgery and rehabilitation on performance and satisfaction of patient identified activity goals in 20 patients (22 arms) who had grip reconstructions for both finger and thumb flexion. Patients assessed an improvement in both performance and satisfaction after surgery in all groups of activities assessed using the Canadian Occupational Performance Measure (COPM). The mean improvement at 6 and 12 months was 3.5 points better than the 2.5 points before surgery. Before surgery 36% of the goals identified were impossible to perform. After surgery, 78% of these goals were possible. The largest improvement was observed in the basic activity of ‘eating’ but significant improvement was also noted in activities generally regarded as complex and not measured in standard ADL such as ‘doing housework’ and taking part in ‘leisure’.
INTRODUCTION
Cervical spinal cord lesions cause dramatic changes in a person’s life. The majority of activities previously performed independently become impossible or require great effort or assistance. Extended rehabilitation is necessary to recapture as many activity skills as possible. After the rehabilitation phase, disability can persist.
Regaining hand and arm function was the highest priority for patients with tetraplegia (Anderson, 2004). In a study of 565 persons, 77% expected significant improvement in their quality of life if their hand function improved (Snoek et al., 2004).
Previous studies focusing on grip strength, range of motion and general ADL demonstrated improvement in hand function after surgery (Forner-Cordero et al., 2003; Gansel et al., 1990; Vastamäki, 2006). However, only a few have focused on the disability rather than impairment. Patients who had any kind of upper extremity surgery are generally satisfied with the outcome (Wuolle et al., 2003). Sixty-eight percent reported improvement in ADL. The individuals included in this study performed more activities, felt more able to function independently and needed less adaptive equipment (Meiners et al., 2002; Wuolle et al., 2003).
In the present study, we have extended the previously documented functional improvements and assessed perceived performance and satisfaction after reconstructive hand surgery. Emphasis has been given to those tasks that were most highly desired by patients.
PATIENTS AND METHODS
Demographics
Post posterior deltoid-to-triceps reconstruction.
Abbreviations: d, dominant hand; nd, nondominant hand; tf, thumb flexion reconstruction; ff, finger flexion reconstruction; ta, thumb abduction reconstruction; Zl, zancolli lasso plasty; CMC, arthrodesis of CMC I. ASIA, Neurological classification according to American Spinal Injury Association; Int Classification, International Classification; McDowell et al., 1986
Surgical reconstruction included muscle-tendon transfer of brachioradialis to flexor pollicis longus (FPL) and extensor carpi radialis longus to flexor digitorum profundi. These tendon transfers were combined with split tenodesis of FPL to extensor pollicis longus. Three cases had fusion of the carpo-metacarpal joint of the thumb and seven cases had tendon transfer of extensor digiti minimi to abductor pollicis brevis. Functional training started the day after surgery and between training sessions the hand was immobilized in splints. Three days after surgery the patients were discharged from hospital. They were carefully told about the training required and given written guidelines on how to do this functional training themselves. One month later they returned to the clinic for 5 days of training focused on activity as well as for follow up of the functional training. Additional follow-ups were undertaken at 2, 3, 6 and 12 months after surgery.
Canadian Occupational Performance Measure (COPM) is an individualized, patient-centred outcome measure that captures a patient’s perception of their performance in daily activities (Law et al., 1998). COPM includes semi-structured interviews during which the individual identifies activities in which difficulties are experienced. COPM has demonstrated sufficient test–retest reliability and validity (Carswell et al., 2004; Wressle et al., 1999). At the 8th International Upper Limb Surgery and Tetraplegia Meeting (2004), the use of COPM was recommended as a measurement tool for research in this patient group (Bryden et al., 2005).
The semi-structured interview was performed on three occasions; before surgery and then at 6 and 12 months after surgery by the treating occupational therapist with extensive experience in this instrument. At follow-up the patient was not dependent on the therapist since treatment was completed before 6 months. As the COPM interviews were about grip reconstruction, the individual described problems experienced in her/his daily life which were caused by their hand. They then chose up to five limitations, which described their activity goals after grip reconstruction surgery. Finally the patient rated their chosen goals for the current level of performance and satisfaction with the performance on scales from 1 to 10 where 1 represented ‘not able to do it’ or ‘not satisfied at all’ and 10 represented ‘able to do (that task) extremely well’ or that the patient was ‘extremely satisfied’ with how that task was performed.
In order to classify the data in the different groups, each goal was classified according to the International Classification of Functioning, disability and health (ICF) in which activities and participation represented one dimension and included nine chapters (World Health Organization, 2002). These are given in a single list covering the range of life areas. The COPM goals were chosen from this list.
Data on performance and satisfaction were compared using Wilcoxon Signed Rank Test to detect differences between pre- and post-surgery assessments. Statistical significance was set at P-value of less than 0.05.
RESULTS
Twenty-two operations were performed on the 20 patients and analysis was done on the 106 goals identified by these individuals.
General and significant improvements were observed for both performance and satisfaction with the performance from the preoperative levels compared with those at 6 and 12 months. The mean improvement was 3.5, from around 2.5 preoperatively to 6 at both 6 and 12 months after surgery (Fig 1). Before surgery, 94% of the performance goals were rated as five or less and 50% as one or two, for both performance and satisfaction. After 12 months, more than 50% of the tasks were rated seven or higher in both performance and satisfaction.
Change of performance and satisfaction of patient prioritized goals. All follow-ups demonstrated significant differences (P < 0.05) compared to the preoperative rating.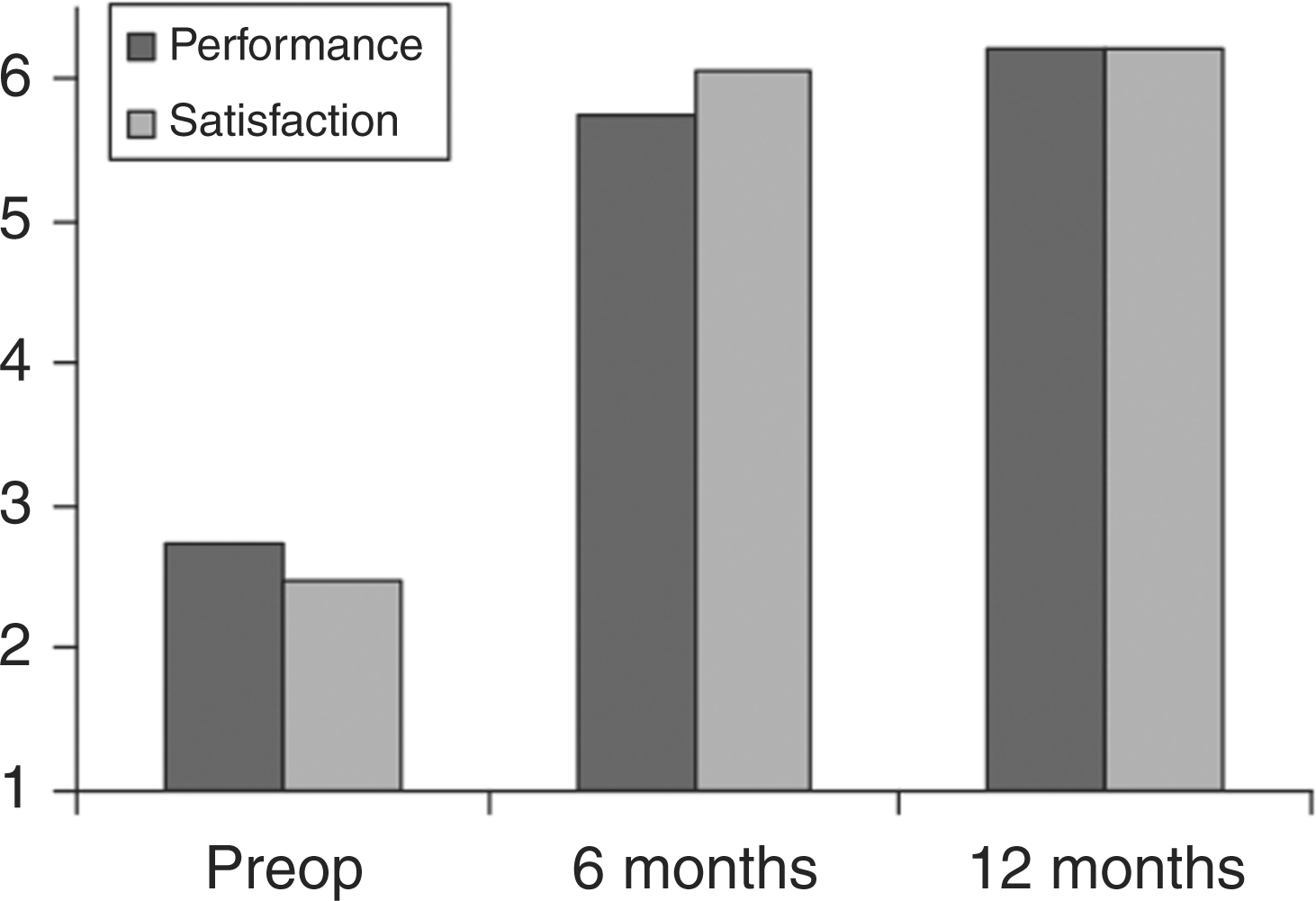
Categories of goals classified according to ICF

After surgery, improvements were reported in both performance and satisfaction for all groups of activities (Fig 2). The improvements for satisfaction were slightly higher than those for performance. The most dramatic improvement occurred after 6 months. Activities for ‘domestic life’, ‘eating’ and ‘leisure’ demonstrated the greatest improvement in both performance and satisfaction, with a more than 4 point improvement after 6 and 12 months. Activities of ‘writing’ and ‘preparing meals’ also improved by more than 4 points for satisfaction. The greatest improvement occurred in satisfaction with ‘leisure’ demonstrating an increase of 5.5 and 6 points after 6 and 12 months. The activities for ‘dressing’ and ‘personal care’ showed the smallest improvement with only a 2 point improvement for performance.
(A) Change in performance, grouped into type of goals. (B) Change in satisfaction, grouped into type of goals. All follow-ups demonstrated significant differences (P < 0.05) compared to the preoperative rating.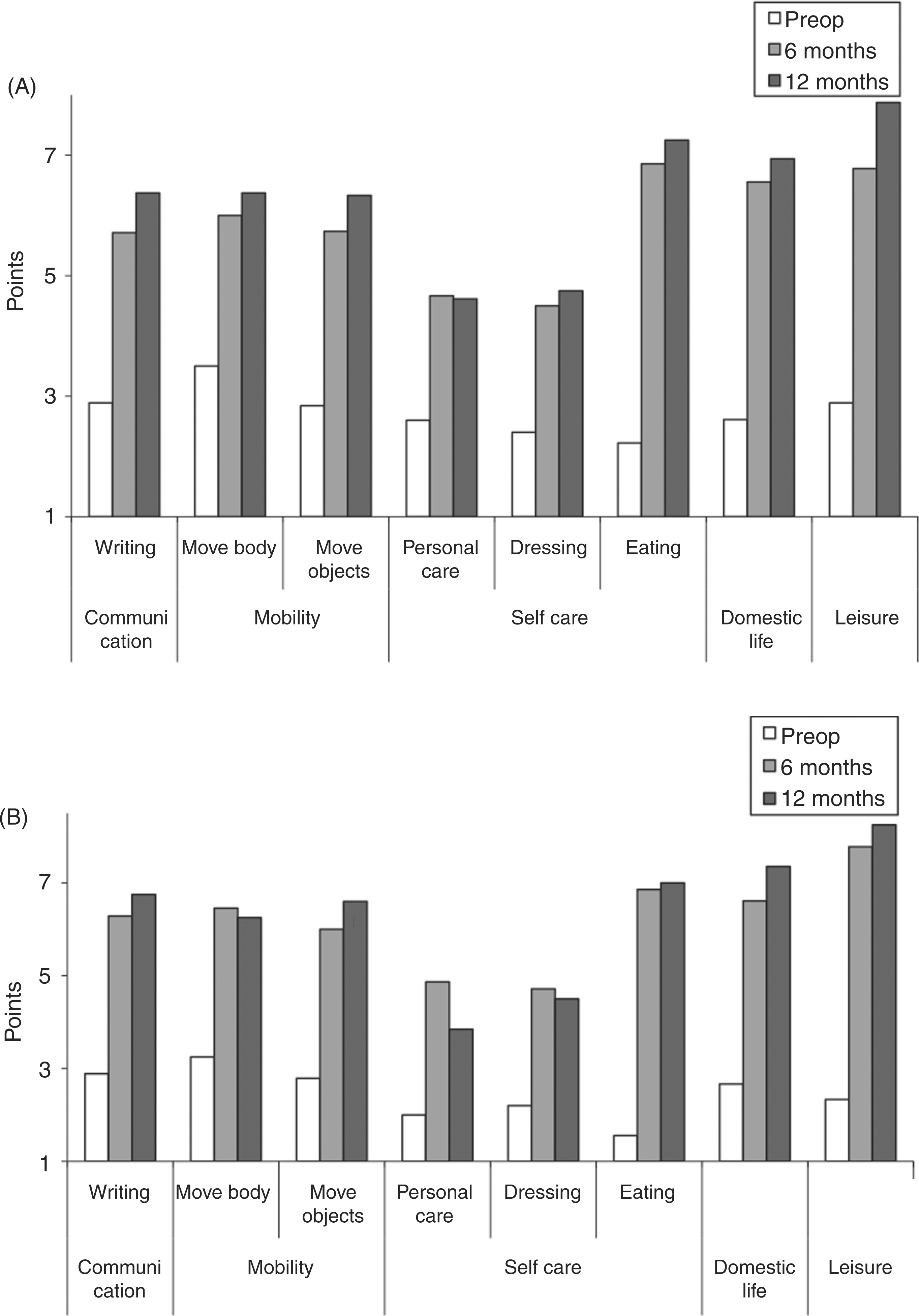
In total, 15% of the performance goals were rated ‘able to do extremely well’ (10) after surgery. For satisfaction, 18% of the goals were rated as ‘extremely satisfied’ (10) after surgery.
Before surgery, 35% of the goals had been rated as impossible to perform. After surgery, 78% of those goals were estimated as possible to do, 11% were rated ‘able to do extremely well’. These activities included ‘writing’, ‘sewing’, ‘holding a fishing pole’ and ‘to button’.
No improvement was reported in 10 of the 106 goals documented and increased impairment reported in a further two goals. Eight of these goals were related to self-care. Eight of the twelve goals with no improvements were activities impossible to perform prior to surgery. Due to reasons not only related to surgery, these activities remained impossible to perform at 6 and 12 months.
At the 6 month follow-up six goals were removed from the collected data due to one person dropping out of the follow up and because one other activity remained impossible to perform. At 12 months, three patients dropped out and a further 15 goals were excluded. A further two goals related to activities impossible to perform at that time were also removed. The four patients who did not attend follow up had a similar distribution of goals.
DISCUSSION
This study demonstrated that after grip reconstruction self rated performance with individually prioritized goals improved. The patients were satisfied with their performance. Law reported that changes over 2 points represent “a clinically important change” (Carswell et al., 2004). Performance of all activities identified in the present study improved by at least 2 points. The primary rehabilitation of spinal cord injury increased the level of performance by 4.6 points (Donnelly et al., 2004). The current study demonstrated general improvements by 3.5 points and in some domains up to 5 points. Patients also rated activities that were impossible to perform before surgery as possible to perform after surgery. The results are similar to those of a previous study which showed that six of eight patients achieved improvements in all five goals they wished to improve with surgery (Lo et al., 1998).
An overall goal for the group was to obtain greater independence and participation at home and in the community. The greatest improvements were found in the basic ADL of ‘eating’, which is in line with results reported by others (Meiners et al., 2002). Interestingly, the most spectacular improvements were observed not only in the basic activity of ‘eating’ but in activities that are generally regarded as complex and not measured in standard ADL measurements, e.g. leisure and domestic life, including gardening and using a hammer. The surgery and the following rehabilitation made a difference in the activities most important in their situation and in activities important in community living with responsibilities including so much more than just the individuals’ self care.
In this study around 40% of the goals related to self care in contrast to a group of individuals newly injured with spinal cord injury, where 79% of prioritized goals were related to self care (Donnelly et al., 2004). It is natural to focus on self care in the first phase of rehabilitation while it is important and natural to focus on other activities and activities in the community after the completion of the acute rehabilitation. The individuals in this study prioritized activity goals related to their previous experiences and their role in the community. This is therefore also reflected in the performance and satisfaction after surgery. These findings highlight that time lapsed after injury appears to have an effect on patients’ individual activity goals. If they would have had additional time to try other activities, they would have gained more knowledge of the likely benefits of surgery. A patient with clear activity goals is an important prerequisite for a successful outcome of surgery.
Several of the activities described as impossible to perform before surgery, but still ranked as highly desired, were often performed well or extremely well and with high levels of satisfaction after surgery. This together with the rated performance and satisfaction indicate that the patients had realistic expectations of surgery. It indicated a high expectation from surgery and also demonstrated a well informed patient. These patients were well informed about what to expect following surgery, and confirmed this by checking the outcomes in discussions with and observations of other patients. Realistic expectations and goals are crucial for the individual to make an informed decision about whether or not to consider surgery. COPM is a useful patient-centred approach which allows the patient to focus on the tasks important to his/her life situation (Donnelly and Carswell, 2002). It is a structured instrument to encourage the patient to take an active role in the process and an important clinical tool to ensure realistic expectations.
In all groups of activities improvement of performance and satisfaction was found at 6 months and in some cases continued to improve 12 months postoperatively. This was probably due to relearning. The patient had to stop using passive ‘tenodesis grips’ and to start using the new active function in all hand tasks. We do not know the endpoint of recovery after surgery and rehabilitation but expect that performance levels will continue to improve for a long period of time as neuromuscular control and new habits in using the hand continues to develop. In this study the patient was responsible for relearning an activity; however, in primary rehabilitation after spinal cord injury professional guidance and support is needed throughout the rehabilitation process of relearning. Further research is therefore required to determine whether intensive rehabilitation after surgery can improve these results even further.
Footnotes
Conflict of interests
None declared.
Acknowledgements
This study was supported by grants from the Swedish Research Council (project number 11200) and University of Gothenburg. The authors are indebted to occupational therapists Annika Dahlgren and Åsa Sand for participation in the data collection and Dr Richard L. Lieber for valuable help with the statistical analyses.
This investigation conforms to the Göteborg University Human Research Protection Program guidelines.