
Abstract
A variety of flaps have been described to treat longitudinal soft tissue defects located on the dorsal aspect of the fingers. We report 13 dorsal soft tissue defects in four patients in which unipedicle laterodigital transposition flaps were used for reconstruction. This flap is especially useful for the reconstruction of long and narrow defects located on the dorsal region of the fingers in multi-digit injuries.
Introduction
It is generally agreed that longitudinal soft tissue defects of the dorsum of the digits are difficult to reconstruct when the defect is long and narrow in shape, spanning more than one phalanx (Fujiwara et al., 2007; Yii and Elliot, 1999). These injuries usually involve multiple fingers. They often cause complex defects in which extensor tendons and bones are exposed and cannot be covered by simple grafting procedures. Also, the shape of individual defect is not the same as most of the flaps described for the hand, unless the defect is enlarged to fit to the contours of the flap, which is an undesirable practice. The limitation of treatment options in multiple finger injuries forces the surgeon to solve the problem within the same digit, since heterodigital flaps are not logical options when the adjacent fingers are already injured. Recent concerns about preserving the proper digital arteries when planning flap coverage has led surgeons to design flaps nourished from the dorsal arterial system of the hand and fingers (Chen and Chiou, 2007; Omokawa et al., 2005; Yang and Morris, 2001). This system is capable of supporting flaps designed on the dorsal aspect of the fingers.
Anatomy: the vascular system of the dorsal aspect of the finger
There is a constant, well defined longitudinal arterial network on the dorsum of the fingers, which has been demonstrated by several authors (Braga-Silva et al., 2002; De Resende et al., 2004; Strauch and De Moura, 1990). This system can be considered as an extension of the dorsal metacarpal arterial system. At the level of the metacarpal head, the metacarpal arteries terminate and form the two dorsal digital arteries coursing distally along the facing sides of the two adjacent fingers. These arteries subdivide further into smaller branches and re-anastomose to form the longitudinal dorsal arterial network stretching to the distal end of the fingers. The dorsal arterial system also receives branches from the palmar arterial arch by commissural arteries located at both sides of the digit. The largest branches are found approximately at the level of the middle and distal thirds of the proximal phalanx (Figure 1). Preservation of these anastomoses during flap dissection further increases the blood supply of the mobilized dorsal soft tissues, minimizing the risk of necrosis.
Vascular anatomy of the unipedicled laterodigital flap.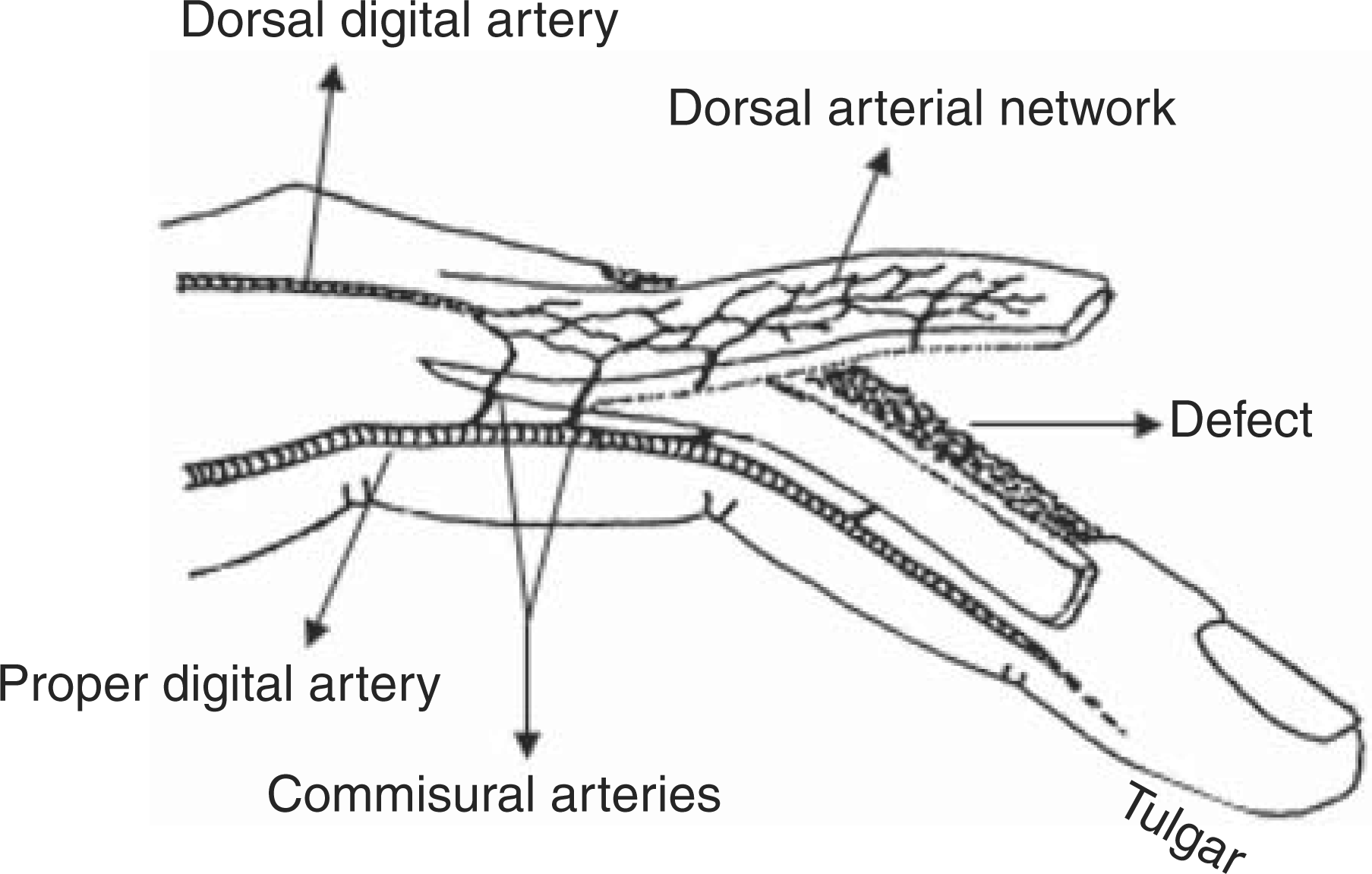
In this study, we describe a proximally based, unipedicled homodigital flap based on the dorsal longitudinal arterial network of the fingers for covering longitudinal defects in multiple finger injuries.
Patients and methods
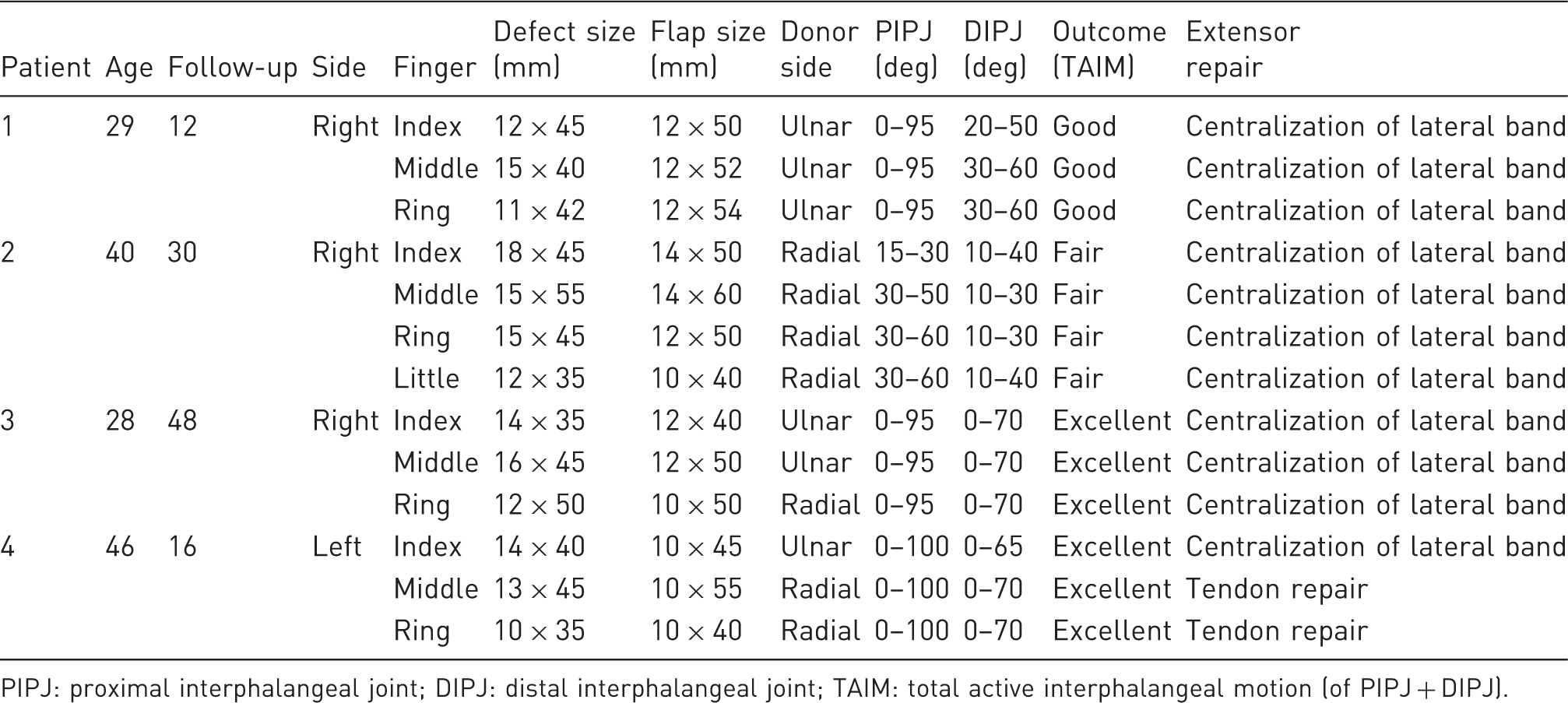
Thirteen fingers in four patients who had dorsal longitudinal soft tissue defects due to injuries from rotating machinery underwent reconstruction of the missing soft tissue cover between December 2004 and July 2007. All the patients were men, with an average age of 35.5 years (range 28–46). The mean follow up of these patients was 26 months (range 12–48). All the patients suffered a central or near central soft tissue loss on the dorsum of the fingers, spanning multiple zones (Figure 2A). In all fingers, the defect included the dorsal side of the proximal phalanx, proximal interphalangeal joint and middle phalanx. In four fingers, the defect extended distal to the distal interphalangeal joint, reaching to the base of the nail. The average length of the defect was 49 mm (range 35–55 mm), with an average width of 14 mm (range 10–18 mm) (Table 1). In all cases, a moderate to severe defect of the central slip of the extensor mechanism was present. In nine fingers, the defect also included superficial bone loss on the dorsum of the proximal interphalangeal joints. After debridement and irrigation, extensor tendon injuries were repaired and the defects were reconstructed using proximally based unipedicled laterodigital transposition flaps.
Case 1. (A) Longitudinal dorsal defects of the index, middle and ring finger. (B) Mobilization of the lateral bands which were centered dorsally to reconstruct the extensor tendon defect at zone 3. (C) Flaps transferred to the defect. (D) Appearance at 12 months after surgery. Patient data PIPJ: proximal interphalangeal joint; DIPJ: distal interphalangeal joint; TAIM: total active interphalangeal motion (of PIPJ + DIPJ).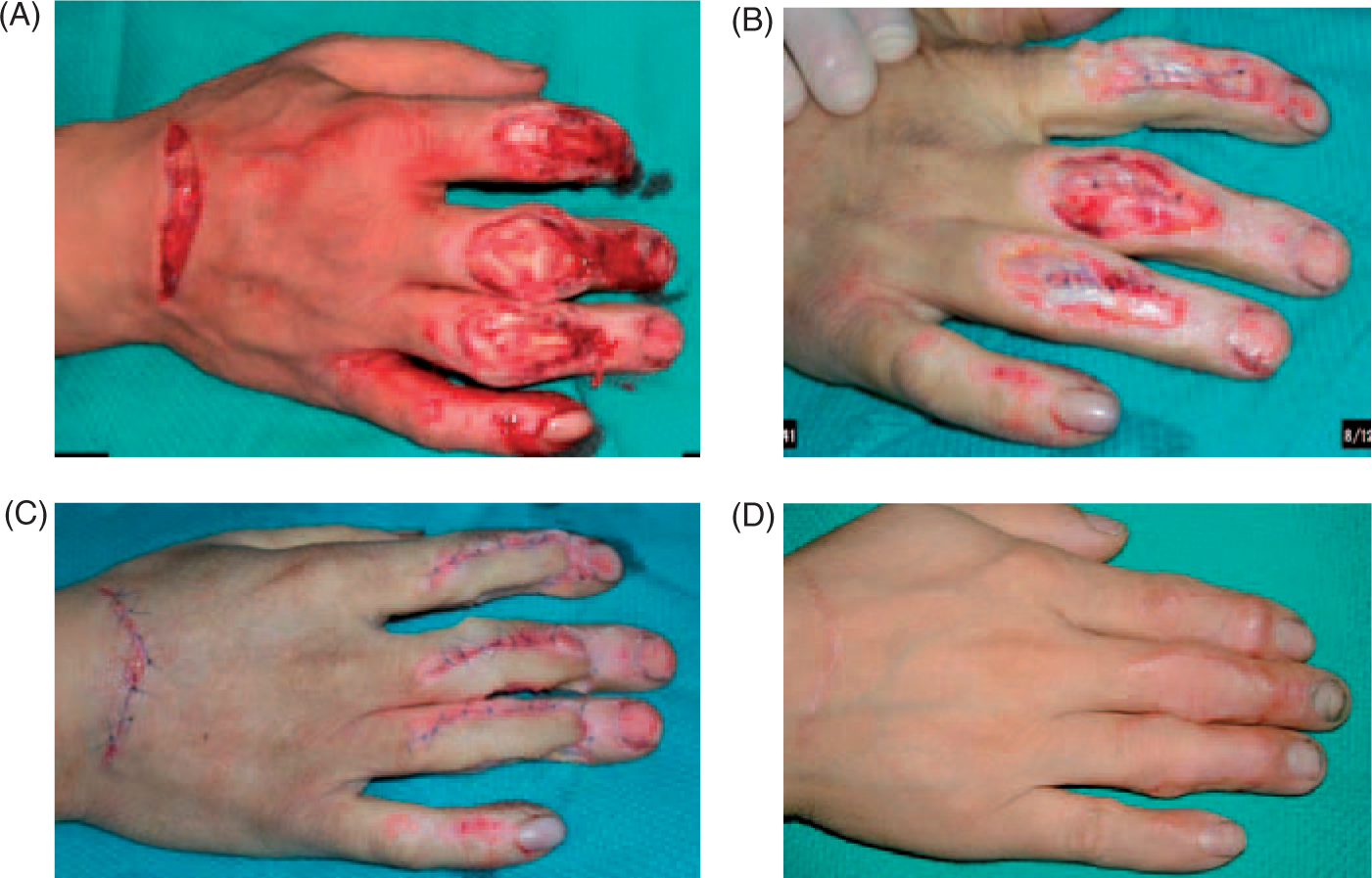
Surgical technique
The operation was carried out using axillary block anaesthesia, tourniquet control and loupe magnification. The central defects of the extensor apparatus were repaired using the local tendon flaps using the method described by Aiache et al. (1970) in which the remaining lateral bands were longitudinally split, the middle portion of both tendons was centralized and the defect was closed (Figure 2B). The soft tissue defect is covered by a laterodigital transposition flap. This is a proximally based longitudinal band of soft tissue mobilized from the adjacent dorsoulnar or dorsoradial side of the defect (Figure 3C). The lateral margin is usually located at the radial or ulnar midlateral line. If needed, this margin can be shifted palmarwards, but the proper digital artery should never be included in the flap. The flap is harvested preferably on the contralateral side of the soft tissue loss in order to include the least damaged tissue and include the greatest number of undamaged vascular connections to the dorsal arterial system within the flap. The flap is elevated based on one of the dorsal digital arteries. Although the proper digital artery is not incorporated, it is advisable to preserve the proximal commissural arteries which anastomose with the dorsal arterial system and include them in the flap in order to increase the vascular supply. To achieve the necessary transposition, Cleland’s ligament can also be divided. If more mobility is desired, the proximal part of the proper digital artery may be freed and shifted dorsally. The length can be extended as much as needed. The distal end of the flap should stretch a few millimetres distal to the injury site in order to eliminate tension on the flap when transferred over the defect. The dorsal venous and arterial network of this flap is located in the subcutaneous plane between the dermis and the paratenon of the extensor tendons. Dissection is carried out in this plane, from distal to proximal, with great care to preserve subcutaneous tissue from injury. There is no need for the pedicle to be visible. When dissection is complete, the elevated soft tissue is transferred onto the recipient area and fixed there with loose sutures. The defect created by raising the flap is covered by a skin graft (Figure 3D). The fingers are splinted for 2 weeks, after which active mobilization is begun.
Case 3. (A) Longitudinal dorsal defects of the index, middle and ring finger due to rotating machinery injury. (B) Partial extensor tendon and dorsal capsular loss as viewed when the fingers are in flexion. (C,D) Flap designs as seen from the radial and ulnar side of the fingers. (E,F) Flaps transferred to the defect and donor sites skin grafted. (G,H) Functional result of the hand at the postoperative fourth year, with perfect ROM of the interphalangeal joints.
Grading
The percentage of normal total active interphalangeal motion (TAIM) was calculated using Strickland’s formula [(TAIM - extension lag) / 175°] × 100. Results were then classified as excellent (85% to 100%), good (70% to 84%), fair (50% to 69%), or poor (<50%) (Strickland, 1985) (Table 1).
Results
We achieved successful coverage of the defects in 13 fingers in four patients with supple skin. Flap circulation was adequate and did not cause any problem in any of the fingers. Partial or total necrosis of the flaps did not occur in any of the fingers and skin grafts healed uneventfully. Hyperpigmentation of full-thickness skin grafts to the flap donor sites was observed in four fingers in one patient. The flap size ranged from 10 × 40 mm to 14 × 60 mm. In fingers in which the extensor mechanism was partially lost, sufficient PIP and DIP joint movement was achieved (Table 1). Mean total active interphalangeal motion was 121° (range 40°–170°). All patients returned to their work or everyday routine at a maximum of 4 months after injury.
Discussion
Dorsal longitudinal defects of the fingers are unique injuries spanning multiple zones, exposing osteo-tendinous components, involving multiple adjacent fingers and usually extending to the distal interphalangeal joints. Simple skin grafting techniques are inadequate since the paratenon is damaged in almost all injuries, necessitating flap coverage.
Of the numerous flaps that have been described, most have matching difficulties and are insufficient for the reconstruction of multiple finger injuries, due to the long and narrow shape and the distal location of the defect. Yii and Elliot (1999) drew attention to these defects and advised the use of bipedicled transposition flaps to achieve coverage. They did not include the proper digital artery in their flap and based their flap solely on the dorsal digital arteries, which forms the ‘pedicle’ at both ends. The mobility of this flap is largest at the centre, gradually becoming less mobile near the pedicles. Defects located around the PIP joint seem most appropriate for reconstruction with this flap. Dorsal defects extending more distally may be difficult to cover with bipedicled flaps because the amount of transposition is restricted at the edge of the flap. To overcome this problem, a proximally based unipedicled flap was designed. This modification has been quite successful in covering distal dorsal defects without causing tensioning of the flap; the unattached distal end greatly increases the arc of transposition. We have observed no complications of flap survival by converting a bipedicled flap into a unipedicled one. The rich dorsal arterial network is capable of maintaining the viability of the flap (Beldame et al., 2008). The dorsal arterial system is capable of nourishing extensive soft tissue elevated from the dorsum of the fingers (Bene et al., 1994; Braga-Silva et al., 2002; De Resende et al., 2004; Endo et al., 1992; Fujiwara et al., 2007; Strauch and De Moura, 1990).
Bene et al. (1994) described a dorsal digital island flap which may include all the dorsal surface of the finger below the proximal third of the proximal phalanx on a bridge of 3–5 mm of intact tissue located at the proximal edge of the flap. No attempt was made to visualize the random venous or arterial branches located in the narrow soft tissue bridge. Although the flap is large, they concluded that the abundant vascular supply enables such a narrow soft tissue pedicle with random vascularity to nourish their flap.
The boomerang flap as also a good example of a dorsal digital flap supplied by the retrograde flow of the dorsal arterial system (Chen et al., 2000). In this flap, the pedicle is formed by incorporating the two adjacent dorsal digital arteries, proving that a dorsal digital artery is sufficient to feed soft tissue harvested from the dorsal side of the finger. In this study we also observed that a proximally based 10 mm to 14 mm wide laterodigital flap with an average length of 50 mm based on dorsal digital arteries survived and healed without any problems.
The main indication for the unipedicled dorsolateral transposition flap is a dorsal longitudinal soft tissue defect of the fingers, spanning the PIP joint and the dorsum of the middle phalanx. This flap can be applied to treat defects up to half the width of the dorsum of the affected digit. Dorsal soft tissue loss extending distal to the DIP joint can also be reconstructed successfully with this flap. The very distal location of such defects limits the choice of possible flaps. Pedicled flaps harvested on a digital vascular bundle may be an option but they sacrifice a major artery (Momeni et al., 2008). Flaps harvested from the dorsal surface of the hand may not reach to the distal edge of the defect. Free flaps for covering multi-digit dorsal defects necessitate advanced microsurgical skills, prolonged hospitalization and secondary operations to separate the syndactylized fingers (Trovato et al., 2008; Yu et al., 2005).
The unipedicled laterodigital transposition flap does not have a random vascularity; instead it has a constant dorsal arterial supply based on the dorsal digital artery which is the extension of the dorsal metacarpal artery. The dorsal digital artery has proven to be a reliable pedicle, since the boomerang flap relies totally on this artery for nourishment. To increase the blood flow to the flap, it is advisable to preserve proximally located commissural arteries and include them in the flap. The suggested length/width ratio in randomized flaps is 2 to 1; in this flap, longer flaps with a ratio of 4–5 to 1 can be elevated without risking the nourishment of the most distal part of the flap. Although the flap has a pedicle at the proximal attached end, it is not advisable to dissect and separate it from the overlying soft tissues, since this may jeopardize blood flow in the artery and adjacent venules. The commissural arteries also should not be dissected extensively; instead soft tissues located between the skin and extensor mechanism should be mobilized and shifted dorsally, as much as the elasticity of these tissues allow.
The advantages of this flap are that: it has similar texture to the lost tissue and excellent pliability; harvesting is simple and quick; it achieves perfect coverage without tension, even on the very distal edges of the defect; early mobilization of the finger is possible; it is a homodigital flap which can be used in multiple digit injuries; the flap is well vascularized, so extensive mobilization is possible without endangering flap survival; it leaves limited scarring confined to the injured finger; and the procedure is a single stage operation that preserves the proper digital arteries.
The disadvantages of this flap include the following: an additional surgical injury to the already traumatized finger; a donor site defect that requires grafting; flap survival is endangered in circumferential crush injuries with contusion of the dorsal side of the finger.
Homodigital flaps are preferred to heterodigital ones, since they avoid injury to the adjacent fingers or dorsum of the hand. Also, these flaps are very useful in multiple digit injuries where an adjacent injured finger cannot be used as a donor finger.
Conflict of interests
None declared.