
Abstract

Dear Sir,
A 21-year-old man presented with a closed rupture of the FDP tendon of the dominant right ring finger 6 weeks after injury. Because of the delayed presentation, he was treated by staged tendon reconstruction. As the first stage procedure a silicone rod was placed and it was planned to use the FDS tendon of the same finger as a graft to reconstruct the FDP tendon, thus converting the finger into a single flexor tendon finger. During the second stage of reconstruction, the FDS tendon of the ring finger was divided near its insertion and Camper’s chiasma was split around the silicone rod. Proximal retrieval of the tendon through a forearm incision proved impossible. It was evident that the little finger flexed at the PIP joint when pulling on the ring finger FDS tendon. This finding raised the likelihood of a common FDS tendon to both ring and little fingers. Further exploration in the forearm confirmed that the little finger did not have an independent muscle belly and tendon. The incision was then extended distally to the wrist and palm, opening the carpal tunnel. A narrow but strong slip of the FDS tendon to the little finger was found to arise from the ring finger FDS just under the superficial palmar arch (Fig 1). Only when that connection was divided could the FDS of the ring finger easily be retrieved. The FDS to the little finger was left in the palm, thus leaving the little finger to be a single flexor tendon digit as well.
FDS tendon to the little finger arising from the FDS of the ring finger, causing the little finger to flex at PIP joint.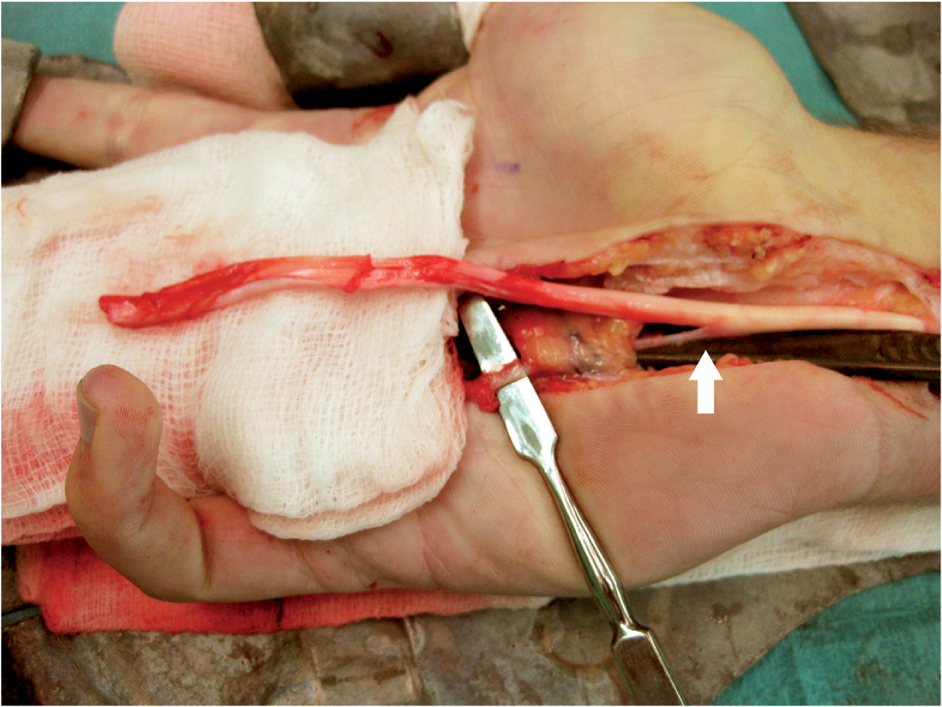
Flexor tendon anomalies, particularly of the little and ring fingers, are well described. One study described anomalous muscle and accessory tendons arising from superficial flexor tendons, inserting into deep flexor tendons (Furnas, 1965). Another study has shown absence of the FDS to the little finger in 15–21% of the population (Austin et al., 1989). An almost similar proportion of the population has a common FDS to the ring and little fingers, leaving 56–58% of the population with an independent FDS in the little finger. A recent study described the standard method of testing the FDS by holding all fingers in full extension except for the little finger (Tan et al., 2009). The little finger was then tested for the presence or absence of isolated FDS function. A hand demonstrating no independent FDS function in the little finger was subjected to a modified FDS test in which all fingers were held in extension except for the little and ring fingers. If the little finger showed flexion at PIP along with the ring finger, it was regarded as having a shared FDS. If the little finger still showed no flexion at the PIP, or PIP flexion only in conjunction with DIP joint flexion, it was labelled as FDS-absent.
A case similar to ours has been described in which a narrow slip of tendon was found arising from the FDS of the ring finger and inserting distally on the FDP of the same finger, thus making tendon retrieval difficult (Evans, 1982). What makes our case notable is the origin of the FDS to the little finger from the ring finger tendon just under the superficial palmar arch. A blind attempt to retrieve the tendon would have risked injury to the palmar arch.
This case underlines the importance of careful preoperative clinical examination of both hands, keeping in mind the numerous variations in flexor tendon anatomy. In situations in which tendon retrieval proves difficult complete exploration is advisable, rather than blind dissection or continued use of forced traction.
Conflict of interests
None declared.