
Abstract
The forearm is composed of the radial and ulnar shafts, which are linked by the interosseous membrane and intercalated between the elbow and wrist. The radius and ulna are connected by three joints, the proximal, middle, and distal radioulnar joints. The forearm ensures pronation/supination and longitudinal load transfer. The biomechanical and clinical relevance of the proximal and distal radioulnar joints is well established. In contrast, the middle radioulnar joint was considered relatively unimportant until studies published in the last decade showed that it fulfils crucial biomechanical functions and is of considerable clinical significance. We believe the conventional concept in which the forearm is viewed as part of either the elbow or the wrist is outdated and that a more relevant concept describes the forearm as a triarticular complex that functions as a full-fledged entity. In this concept, the three forearm radioulnar joints (proximal, middle, distal) work together to provide stability, mobility and load transfer. Here, we will argue for the relevance of the triarticular complex concept based on published data about forearm biomechanics and pathological conditions.
Introduction
The forearm has three main functions: to allow pronosupination and therefore appropriate hand positioning, to transfer longitudinal loads between the wrist and the elbow, and to serve as an attachment site for the muscles that move the wrist and fingers (Kapandji, 2005). The forearm is made of two bones, the radius and the ulna, which are joined at the proximal and distal radioulnar joints (PRUJ and DRUJ, respectively). Both joints are located at the ends of the forearm and are therefore often considered part of the elbow (PRUJ) and wrist (DRUJ). The largest part of the forearm, between the DRUJ and PRUJ, is composed of the radial and ulnar shafts linked by the interosseous membrane (IOM) and is classically viewed as a transition segment between the elbow and wrist.
The anatomical definition of a joint is the junction between two or more bones, usually with the interposition of connective tissue or cartilage (Garnier and Delamare, 2004). However, structures such as the scapulo-thoracic junction and subacromial space are also classified as joints. By definition, joints serve to allow motion and to provide mechanical support. Joints are classified structurally and functionally according to the shape of the articular surfaces, type of tissue interposed between the bones, and characteristics of joint motion (Drake et al., 2006). Between the PRUJ and DRUJ, the radial shaft moves around the ulnar shaft (Hollister et al., 1994; McGinley and Kozin, 2001; McGinley et al., 2001; Moritomo et al., 2009). Therefore, the radial and ulnar shafts linked by the IOM can be viewed as an authentic joint. Because this joint is intercalated between the PRUJ and DRUJ, an appropriate designation is ‘middle radioulnar joint’ (MRUJ), as suggested by LaStayo and Lee (2006). According to another interesting concept put forward by Hagert, the proximal and distal radioulnar joints together form a bicondylar joint (Hagert, 1987; 1992). Over the last decade, an increasing number of studies focused on the IOM (and therefore the MRUJ). Their results establish that the IOM is not merely a fibrous band filling the interosseous space, but instead a multicomponent ligamentous structure that has a complex behaviour and plays an essential role in forearm stability and physiology (Birkbeck et al., 1997). The insights provided by several studies of the IOM suggest that the conventional description of the forearm as a simple segment intercalated between the wrist and the elbow may be outdated and that a more relevant concept may be that of a triarticular complex in which the MRUJ plays a crucial role (Gabl et al., 1998; Hagert, 1987; 1992).
The goals of this article are to demonstrate that the forearm should be viewed as a triarticular complex and that, although the MRUJ is intimately related to the DRUJ and PRUJ, it represents a specific entity. To achieve these goals, we will draw from anatomic, biomechanical, phylogenetic, pathologic, and therapeutic data in the literature.
The MRUJ and forearm triarticular complex: descriptive anatomy and biomechanics
Descriptive and functional anatomy of the MRUJ
The MRUJ is composed of the radial and ulnar shafts linked by the IOM and oblique cord (Figure 1). While the ulnar shaft axis is almost linear, the radial shaft exhibits a supinator curvature and a pronator curvature that are essential to pronosupination (Matthews et al., 1982; Schweizer et al., 2009). The IOM is formed by two groups of fibres (Moritomo et al., 2009; Poitevin, 2001; Soubeyrand et al., 2007). Fibres of the first group course proximally toward the ulna, while those of the second group run proximally toward the radius. The second group is the most important in terms of thickness and function. It can be separated into at least three parts according to morphology and function. The most important part is the middle part, known as the central band, which is a strong coherent structure. It is inserted on the ulna at an angle of 21° on average to the longitudinal axis of the ulna (Skahen et al., 1997). The central band fibres are the thickest fibres in the IOM, whereas the distal fibres are the thinnest. The orientation of the IOM fibres governs the vector of their biomechanical action. This vector can be divided into a transverse and a vertical vector. The transverse vector reflects the role of the IOM in limiting interosseous space expansion, i.e., in ensuring the transverse stability of the forearm. The vertical vector limits the proximal migration of the radius and contributes to maintain the distal radioulnar variance. Fibre tension is greatest in neutral rotation in the central band and in full supination in the distal fibres (Moritomo et al., 2009; Nakamura et al., 1999a; 1999b; Noda et al., 2009). As supination or pronation increases, progressive recruitment of the distal or central-band fibres, respectively, occurs. Thus, the stabilizing role of the various IOM components depends on forearm position. This fibre recruitment process is crucial to allow forearm rotation, as illustrated by the contribution of IOM fibre retraction to the loss of pronosupination in children with brachial plexus birth palsy, in whom IOM release is required to restore passive rotation of the radius (Ozkan et al., 2004). At the wrist, longitudinal loads pass chiefly through the radiocarpal joint and to a lesser extent from the carpus to the ulna (Markolf et al., 1998; 2000; Pfaeffle et al., 1999; 2000). At the elbow, this ratio is inverted, with most of the longitudinal loads transmitted between the forearm and humerus passing through the humeroulnar joint. This ratio difference implies that a load transfer occurs between the radius and the ulna (Birkbeck et al., 1997). Thus, longitudinal forearm stabilization and load transfer are closely associated. Load transfer between the radius and the ulna is ensured by the MRUJ via the IOM.
The MRUJ and forearm triarticular complex.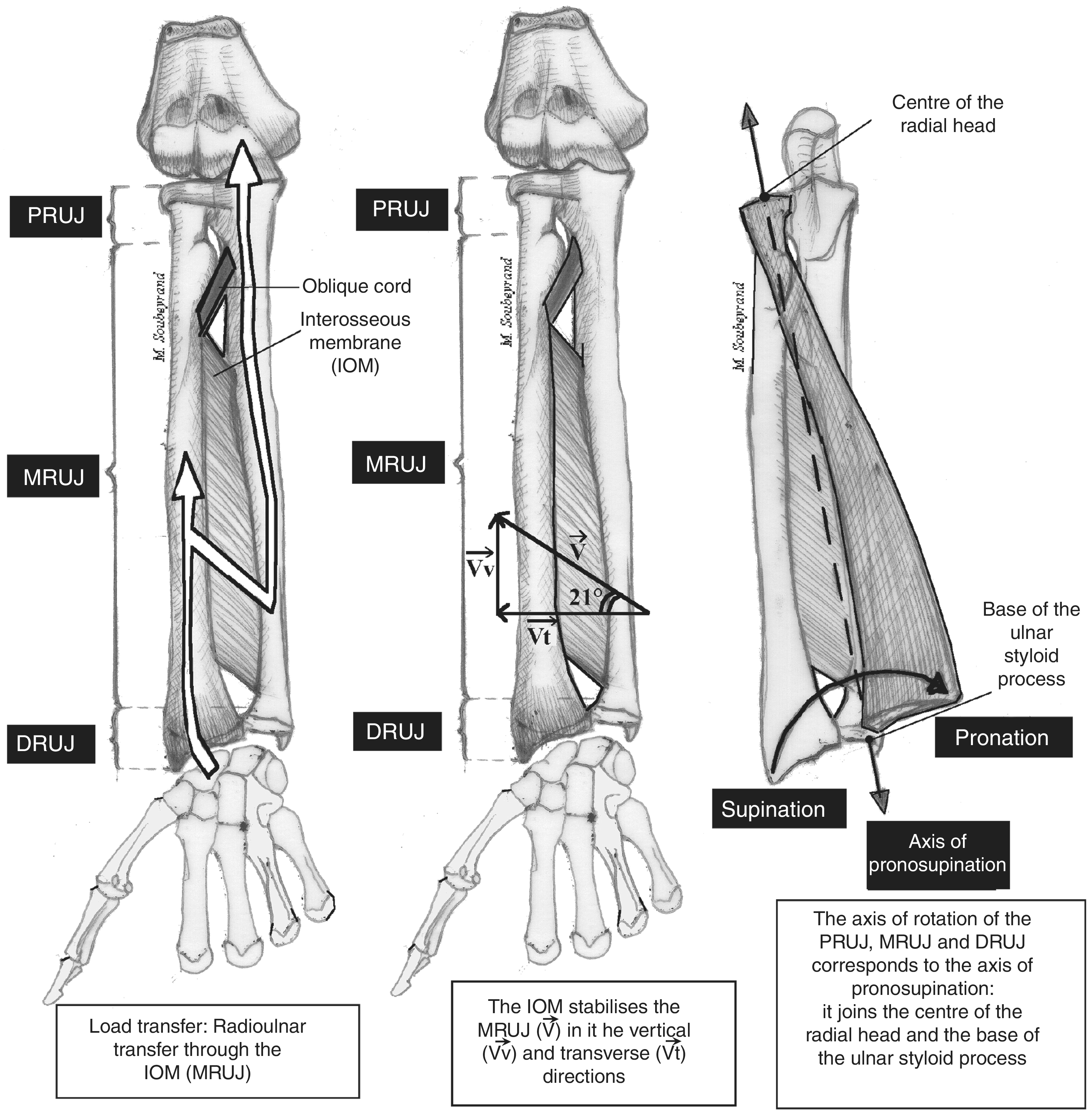
The specific movement of the forearm triarticular complex is pronosupination, in which the radius rotates around the ulna. Hollister et al. (1994) demonstrated that this rotation occurs around a constant axis that is independent of elbow flexion and extension. This axis joins the centre of the radial head and the base of the styloid ulnar process at the insertion of the triangular fibrocartilage complex (TFCC). It keeps a constant relationship to the IOM throughout the entire range of rotation and therefore represents the axis of motion of the MRUJ. Changes in the positional relationship between this axis and the IOM modify MRUJ kinematics, thereby inducing loss of pronosupination (Yasutomi et al., 2002).
Specific features of the MRUJ compared to the PRUJ and DRUJ
Most of the muscles involved in pronosupination (i.e., pronator teres, brachial biceps, and supinator) insert at the MRUJ. Moreover, the PRUJ and the DRUJ are classified as uniaxial synovial pivot joints, whereas the MRUJ is a fibrous joint. However, these three joints share the above-described axis of rotation.
Functional relationships between the three radioulnar joints
The IOM, which is part of the MRUJ, plays an important role in the longitudinal and transverse stability of the forearm (Green and Zelouf, 2009), to which the PRUJ and DRUJ also contribute. The joint between the radial head and the capitellum prevents proximal migration of the radius, as does the TFCC at the DRUJ (Rabinowitz et al., 1994; Shaaban et al., 2004). The annular ligament maintains the radial head in the lesser sigmoid notch of the ulna, while the TFCC prevents expansion of the space between the distal ulnar and radial epiphyses. Moreover, stabilizers considered specific to one joint can contribute indirectly to the stability of the adjacent joint. For example, Watanabe et al. (2005) have demonstrated that IOM disruption is required for DRUJ dislocation to occur. For all these reasons, the forearm can be viewed as a triarticular complex in which the PRUJ, DRUJ, and MRUJ work in close cooperation to allow pronosupination and to ensure forearm stability. Forearm stability is directly related to longitudinal load transfer from the wrist to the elbow. This fact highlights the crucial role played by the MRUJ in forearm physiology and, more broadly, in upper limb function. The IOM not only transfers loads between the radius and the ulna, but also absorbs part of the loads. Thus, the forearm can be likened to a shock absorber that protects the proximal upper limb from the effects of longitudinal impacts on the wrist such as occur, for instance, during a fall on the outstretched hand. Another example is the Essex-Lopresti syndrome (Essex-Lopresti, 1951), in which the longitudinal stabilizers (i.e., radial head, IOM, and TFCC) are injured but the proximal upper limb is usually intact.
Phylogenesis and comparative anatomy of the MRUJ
That the MRUJ is an authentic joint responsible for important functions, alongside the PRUJ and DRUJ, is apparent from a comparison of the human forearm with forearms of other species, most notably mammalians. According to the taxonomic classification of species (Retrieved February 4, 2010, from the Integrated Taxonomic Information System (ITIS), http://www.itis.gov) derived from the works of Carl Linnaeus (1707–1778) (Linnaeus, 1735), Homo sapiens belongs to the phylum Chordata, class Mammalia, order Primates, family Hominidae, and genus Homo. The human upper limb has a similar structure to that of the other pentadactylous tetrapods (Mariani and Martin, 2003; Tickle, 2003). It is composed of four differentiated segments: the stylopodium or proximal segment, containing a single bone (the humerus); the zeugopodium, with two bones (the radius and ulna); the mesopodium, composed of the carpal bones; and the autopodium or hand skeleton. Among species having two forearm bones, some use their radius and ulna to achieve pronosupination (e.g., humans, monkeys, cats, and dogs), whereas others do not. In the order Primates (which includes humans), the IOM does not extend to the PRUJ and DRUJ; whereas in the order Carnivora (which includes cats and dogs), it occupies the entire interosseous space. In humans, the oblique cord is inconsistently present, of moderate size, and well separated from the IOM (Tubbs et al., 2007). In dogs and cats, in contrast, the oblique cord is a large strong ligament that adheres closely to the IOM. In the obsolete order Ungulata, which encompassed mammalians belonging to the orders Artiodactyla (e.g., bovines, goats, pigs, and hippopotami), Perissodactyla (e.g., horses and rhinoceros), Cetacea (e.g., dolphins and whales), and Proboscidea (elephants), the two forearm bones are joined, not by an IOM, but by a strong, short, wide interosseous ligament that forms a syndesmosis. This ligament allows very little range of motion and, moreover, undergoes ossification with advancing age. Interosseous vessels then perforate the ossified ligament through an authentic foramen that marks the boundary between the proximal and distal interosseous ligaments. Thus, the considerable range of motion at the MRUJ appears specific of the order Primates. The forelimb is composed of a humerus, a radius, and an ulna in several classes of the phylum Chordata including Mammalia, Reptilia, and Amphibia and the oldest example of this forelimb pattern known to date is Eusthenopteron, a lobe-finned fish that lived 380 million years ago (Marzke, 2009). Thus, this pattern probably derives from a common ancestor. Several authors have stated a belief that evolutionary changes in the forelimb (the upper limb in humans) occurred in relation with changes in the behaviours of our ancestors (Ladd, 2009; Marzke, 2009; Oberlin, 2006). The common ancestor of the order Primates that lived 56 million years ago was an arboreal animal that ate fruits and insects and that grasped branches to move from tree to tree. Whereas the hind limb provided support and propulsion, the forelimb evolved in a way that increased the precision with which the animal could position the autopodium (the hand) in order to manipulate objects and to hang from branches. Thus, the forearm became smaller, and pronosupination was allowed by an increase in mobility between the two forearm bones with the development of the radial curvatures. The leg skeleton, in contrast, evolved to improve weight bearing, which requires considerable stability. Thus, there is very little motion between the tibia and fibula, which have relatively straight shafts. The forearm IOM exhibits a complex biomechanical behaviour, with sequential fibre recruitment, whereas the leg IOM is constantly taut from its proximal to its distal end (Minns and Hunter, 1976). Thus, the MRUJ is an exceptional joint in terms of shape and biomechanics.
From another point of view, the articular forearm complex can be compared to the femorotibial joint, as done previously by Hagert et al. (1987; 1992): the PRUJ and DRUJ can be likened to the medial and lateral femorotibial compartments and the IOM to the cruciate ligaments. However, pronosupination consists in pure rotation around a linear and fixed axis (Hollister et al., 1994), whereas flexion–extension of the knee associates rolling and sliding motions around a mobile axis.
Pathological conditions of the triarticular forearm complex
Two types of pathological conditions may affect the triarticular forearm complex, namely, instability and range-of-motion limitation due to radioulnar joint stiffness or synostosis. The cause is usually traumatic and occasionally congenital.
Radioulnar joint stiffness and synostosis
Either a synostosis at any level between the radius and ulna or stiffness involving the PRUJ or DRUJ can lead to loss of pronation/supination of the entire forearm (Kamineni et al., 2002) (Figure 2). An example of forearm stiffness due to MRUJ disease is angular or rotational malunion of the radial or ulnar shaft (Matthews et al., 1982; Tarr et al., 1984). MRUJ stiffness can also be caused by IOM contracture in patients with brachial plexus birth palsy (Ozkan et al., 2004). Thus, the range of motion of each joint in the triarticular complex depends directly on the range of motion of the other two joints.
Synostosis.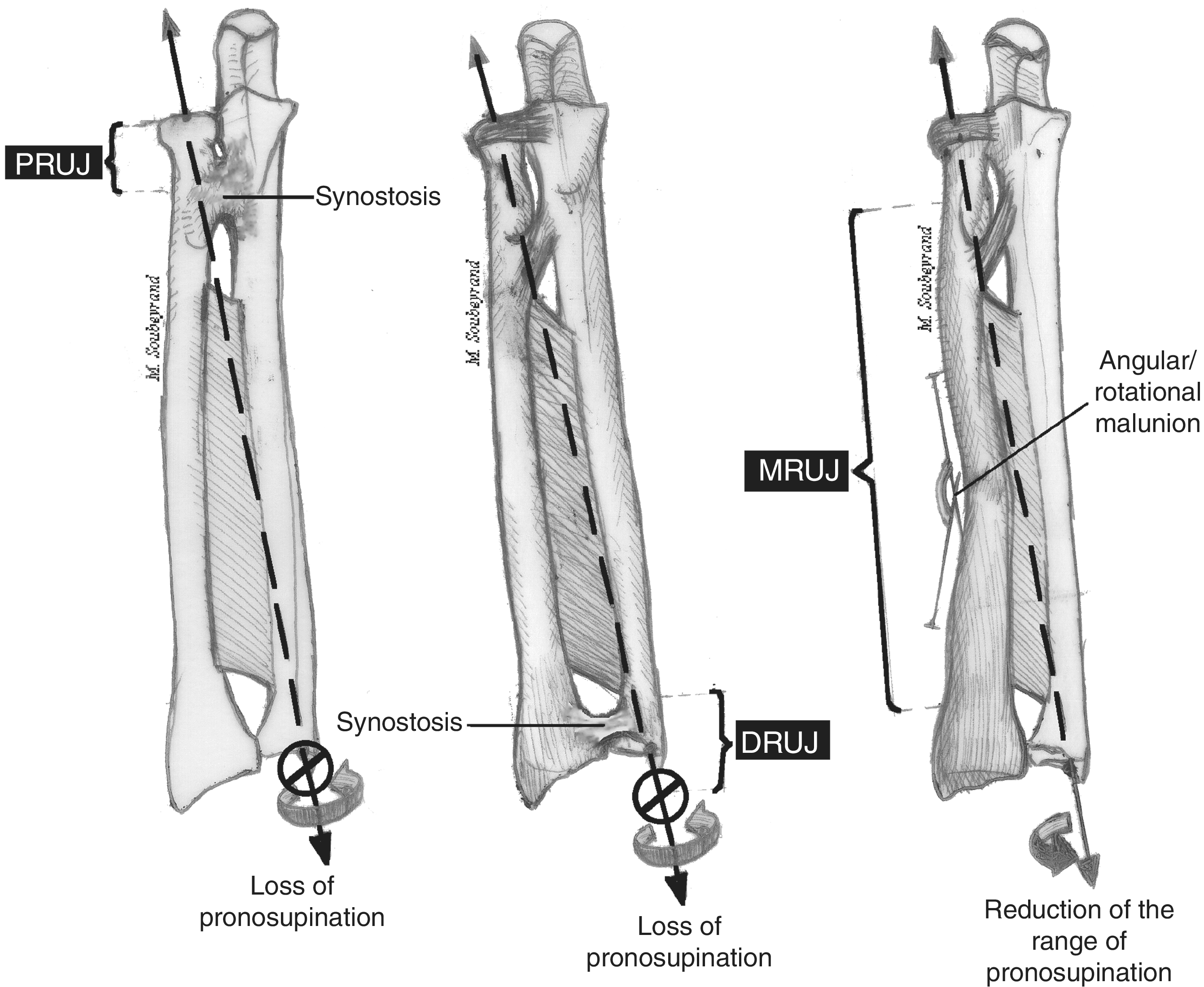
Instability
As explained above, the forearm is stabilized in both the transverse and the longitudinal direction (Green and Zelouf, 2009; Pfaeffle et al., 1999; 2000). Examples of transverse instability (Figure 3) include radial head dislocation at the PRUJ, for instance in Monteggia’s fracture (Eathiraju et al., 2007), ulnar head dislocation at the DRUJ, as in Galeazzi’s fracture (Giannoulis and Sotereanos, 2007), and isolated ulnar head dislocation. In these situations, inadequate stabilization of either the PRUJ or the DRUJ is sufficient to induce loss of pronosupination, even if the other forearm joints are intact. Leung et al. (2005) have described a pattern of lesion called ‘criss-cross injury’ in which both the PRUJ and the DRUJ are dislocated, whereas the MRUJ is intact (intact IOM, radial shaft, and ulnar shaft). The dislocations prevent forearm rotation.
Instability.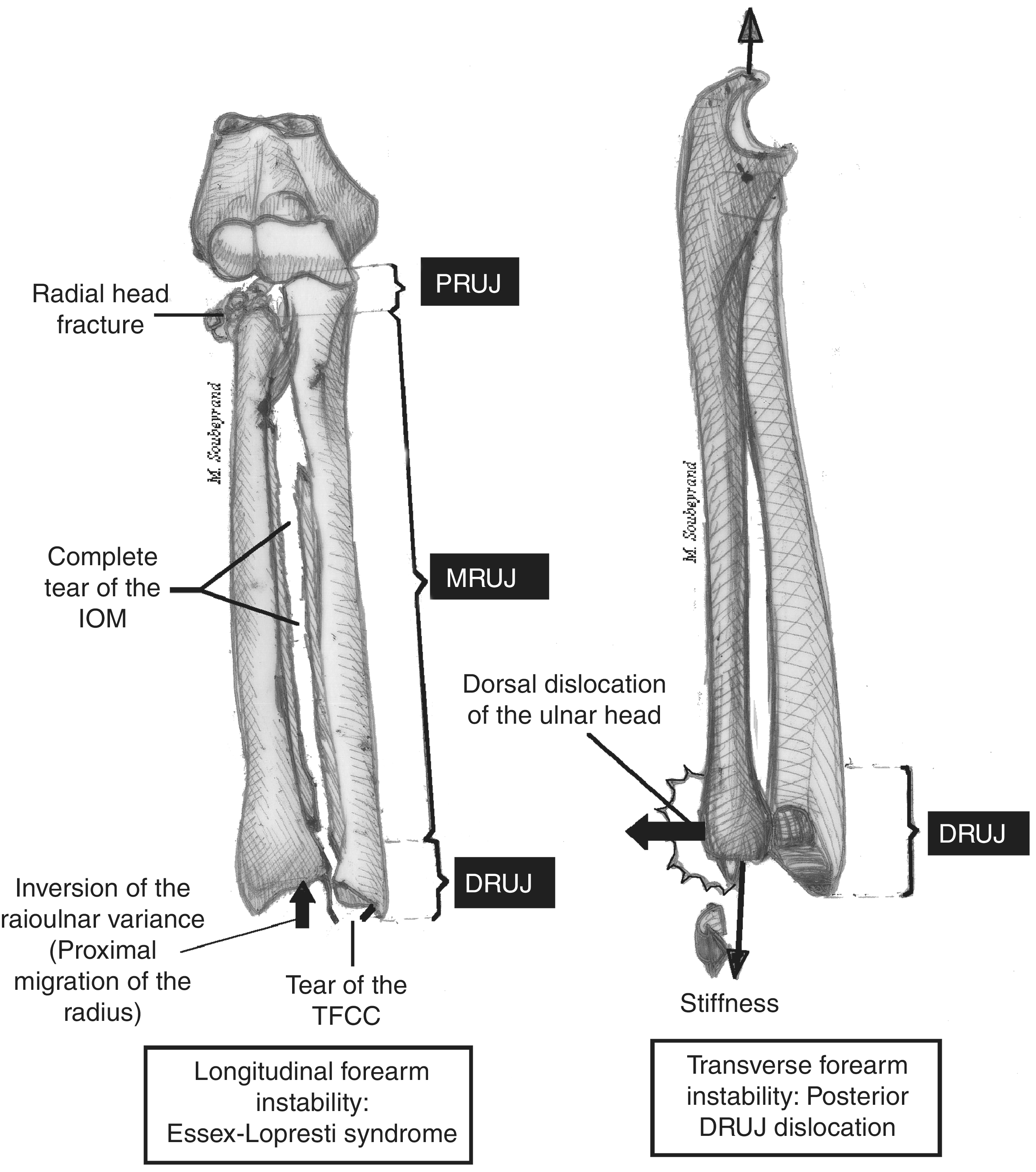
Longitudinal instability occurs in the Essex-Lopresti syndrome (Essex-Lopresti, 1951), in which all three forearm joints are damaged: the PRUJ (radial head fracture), the MRUJ (tear of the IOM), and the DRUJ (TFCC tear and inversion of the radioulnar variance with ulnocarpal abutment). The result is complete forearm destabilization, which contraindicates isolated radial head resection, because of the risk of proximal migration of the radius (Tejwani and Mehta, 2007). Prosthetic replacement of the radial head is therefore recommended but may lead to elbow pain and prosthesis subluxation, because of the IOM tear. The radius is pulled proximally by muscles such as the biceps. When the IOM fails to ensure longitudinal stability, the radiocapitellar joint is exposed to excessive loads that damage the capitellar cartilage (Jungbluth et al., 2008). This mechanism may explain the development of elbow pain after prosthetic replacement of a fractured radial head that was actually one manifestation of missed Essex-Lopresti syndrome (Jungbluth et al., 2006; 2008). The combined damage to the PRUJ, MRUJ, and DRUJ explains why most authors recommend treatment of all three joints and why several IOM ligamentoplasty techniques have been developed (Chloros et al., 2008; Green and Zelouf, 2009; Soubeyrand et al., 2007). In a cadaver study, Pfaeffle et al. (2006) demonstrated that IOM ligamentoplasty decreased the loads applied by the prosthesis to the capitellum.
Whereas instability involving the PRUJ or DRUJ is easy to diagnose on standard radiographs, instability of the MRUJ and therefore the status of the IOM are much more difficult to assess. MRI was used by some authors (Nakamura et al., 1999c; 2000; Starch and Dabezies, 2001) and stress radiographs by others, including Smith et al. (2002), who described the ‘radius pull test’. However, the most efficient tool for diagnosing IOM disruption may be static ultrasonography (Failla et al., 1999; Jaakkola et al., 2001) or overall dynamic ultrasonography (Soubeyrand et al., 2006).
Conclusion
The MRUJ is an authentic joint composed of the radial and ulnar shafts connected by the IOM. It is one of the three forearm joints, whose anatomy, biomechanics, phylogenesis, and pathological conditions are intimately linked. Thus, the forearm is best viewed as a triarticular complex. Although it articulates with the arm proximally and the wrist distally, the forearm is a full-fledged entity. The clinical and radiological evaluation of the forearm must be conducted with the triarticular concept in mind to ensure that no lesions are missed.
Footnotes
Conflict of interests
None declared.