
Abstract
Chronic exertional compartment syndrome of the forearm is rare in the published literature. We report the outcome of a series of 12 patients treated with fasciotomy over a 14 year period. All patients underwent dynamic intra-compartmental pressure testing using a slit catheter technique before surgery. Raised intra-compartmental pressures on exercise, typical symptoms and the absence of other diagnoses were criteria for offering surgical intervention. The superficial flexor, deep flexor and extensor compartments were released. Median follow-up was 9.5 years (range 7 months to 12 years). Median patient-reported percentage improvement after surgery was 88% (range 0%–100%). Median time to return to full activity was 9 weeks. Eleven out of 12 patients were satisfied, very satisfied or extremely satisfied with the outcome of surgery. Fasciotomy can be an effective treatment for chronic exertional compartment syndrome of the forearm.
Introduction
Chronic exertional compartment syndrome (CECS) of the lower limb is well reported (Bourne and Rorabeck, 1989; Detmer et al., 1985; Pedowitz et al., 1990). However, CECS of the forearm is rare in the published literature. CECS of the forearm has been described in association with weight training (Jawed et al., 2001), kayaking (Piasecki et al., 2008), tennis (Berlemann et al., 1998), carpentry (Soderberg, 1996), gymnastics and field hockey (Wasilewski and Asdourian, 1991), wheelchair athletics, climbing, water skiing (Zandi and Bell, 2005), and factory assembly work (Kutz et al., 1985; Pedowitz and Toutounghi, 1988) but seems particularly prevalent in motorcycling (Allen and Barnes, 1989; Garcia Mata et al., 1999; Goubier and Saillant, 2003; Jeschke et al., 2006; Zandi and Bell, 2005).
The forearm is made up of three fascial compartments (extensor, deep flexor and superficial flexor), all of which can be at risk of developing a compartment syndrome. Typical symptoms of CECS described in the literature include pain, a feeling of tightness, hardness or a ‘pumped up’ sensation in the forearm, cramping, swelling, paraesthesiae of the fingers, weakness and a feeling of loss of control of the hand. The symptoms are brought on by exertion and relieved by rest, but recur when the precipitating activity is resumed. Symptoms are often bilateral. This pattern of symptoms was reflected in our series.
Differential diagnoses for CECS include tendinopathies, as well as vascular and nerve entrapments. Patients require a thorough physical examination, with nerve conduction studies as indicated. Clinical examination at rest is typically normal in CECS and assessments are made to exclude other potential causes. The diagnosis of CECS is generally confirmed by measuring raised intra-compartmental pressures during and/or after exercise.
We performed a retrospective study to determine the long-term outcome of decompressive fasciotomy for CECS of the forearm undertaken by a single surgeon in a single centre over a 14 year period.
Methods
Patients who had undergone fasciotomy of the forearm for CECS were identified using surgical databases, theatre logs and pressure testing records in our centre. All had met the established criteria for surgery. Where available, the medical records were obtained and reviewed. Patients described pain, tightness, cramping, solidity or ‘pumped up’ sensations on activity. Tingling, weakness and numbness of the hands were also often reported. Symptoms resolved following periods of rest from 5 minutes to 2 hours. Intra-compartmental pressure (ICP) measurements were available for each patient.
Patients identified were contacted by telephone or mail by independent investigators. Having provided consent to be included in the study, their history and complications were confirmed and their outcome recorded. As no standardized outcome measure exists for this condition, outcome was ascertained by asking each patient to self-rate the percentage improvement they felt the surgery had achieved (0% being no improvement and 100% improvement representing cure). The level of satisfaction with the outcome was recorded on a seven-point scale (extremely dissatisfied, very dissatisfied, dissatisfied, neutral, satisfied, very satisfied or extremely satisfied). The time taken to return to activity after surgery was also recorded.
One further patient was identified with a typical presentation of CECS who had raised compartment pressures on testing but elected not to undergo surgery. This patient was also contacted for follow-up.
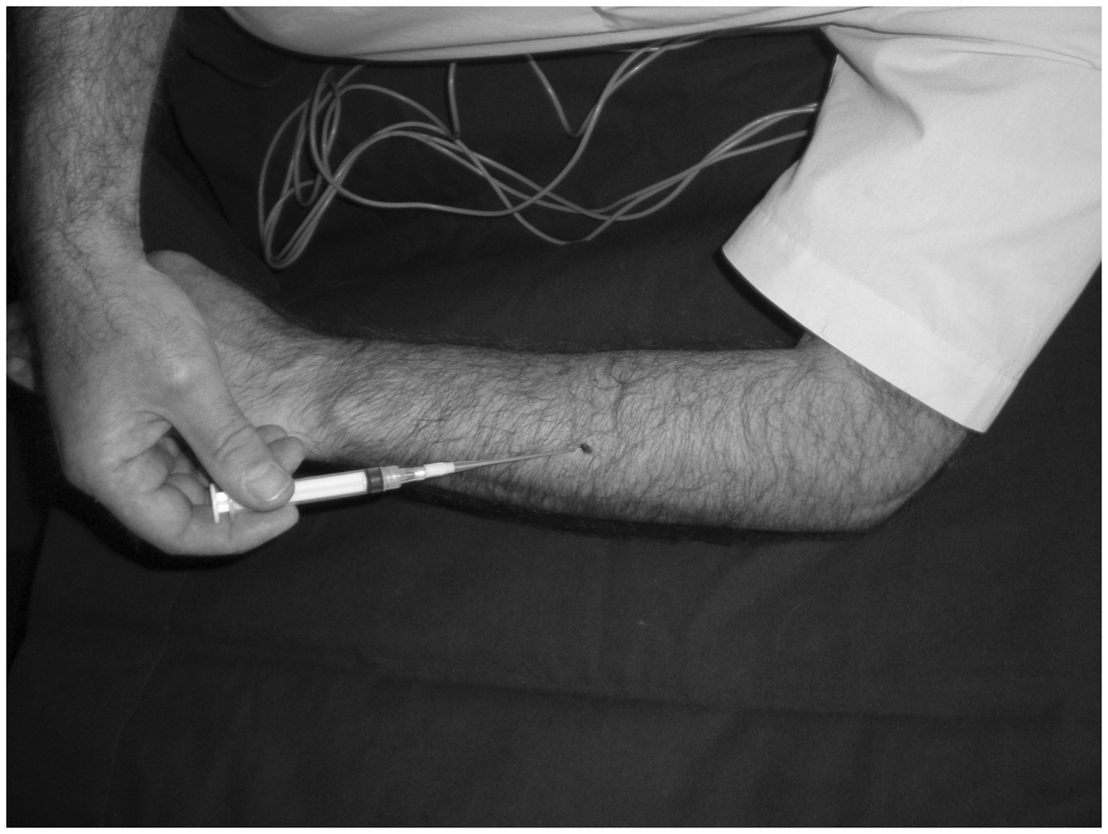
Dynamic intra-compartmental pressure measurements were obtained using slit catheters as described in Barnes et al. (1985). Following local anaesthetic infiltration of the skin with 1 ml of 2% lidocaine, Medicut intravenous 16 g cannulae (Tyco Healthcare UK Ltd, Northern Ireland, UK) were inserted into the clinically relevant compartments to permit passage of a 16 g slit catheter pre-filled with heparinized saline. The superficial flexor compartment was entered in the midline of the middle third of the flexor aspect of the forearm (the compartment lying directly under the deep fascia) (Figure 1). The deep flexor compartment was accessed in the middle third of the forearm by sliding the catheter just anterior to the ulna (Figure 2). The extensor compartment was entered in the midline of the middle third of the extensor aspect of the forearm (the compartment lying directly under the deep fascia) (Figure 3). The catheters were connected directly to pressure transducers (Spectramed P10 EZ pressure transducer, Gould Inc., Cleveland, USA) which in turn were connected to an amplifier and analogue chart recorder (Gould Inc., Cleveland, USA). If the patient’s symptoms were similar in both forearms then the compartments of only a single forearm were measured. It is our experience that the pressures in one symptomatic forearm are likely to be mirrored in the other.
Site of catheter into superficial flexor compartment. Site of catheter into deep flexor compartment. Site of catheter into extensor compartment.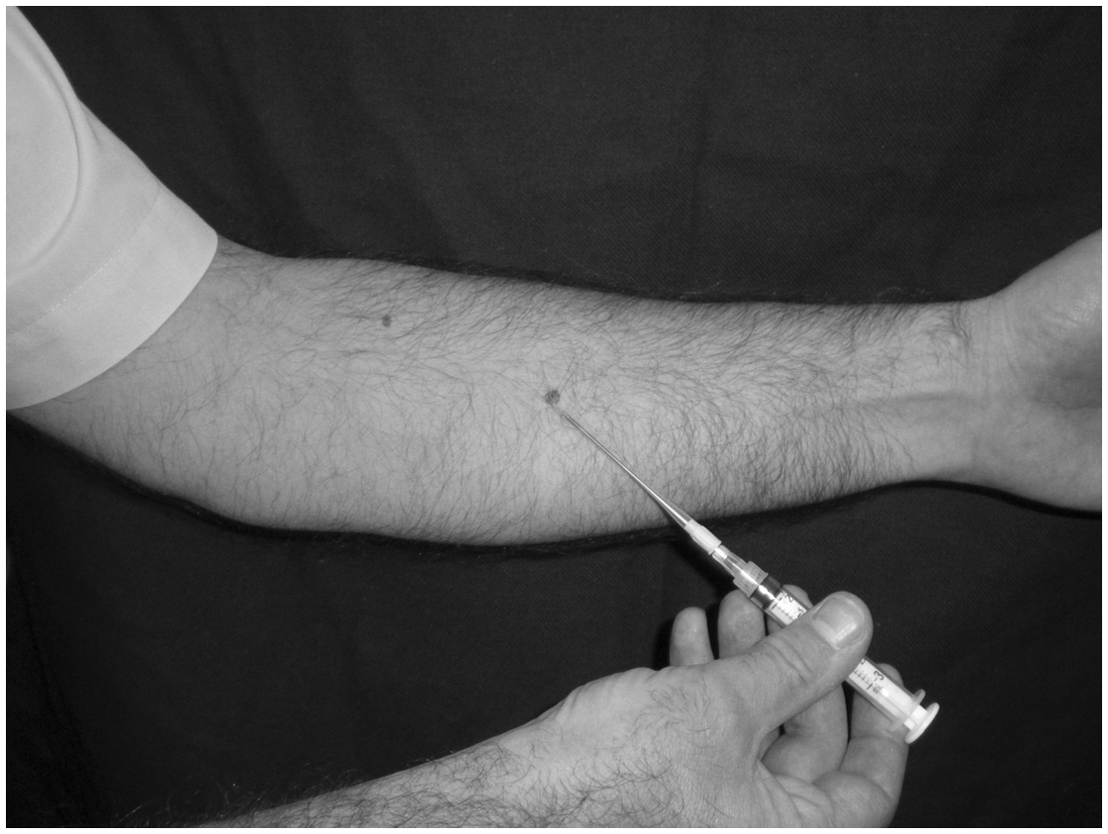

During testing, the patient sits upright on a couch with the forearm horizontal and hand resting on the thigh. A resting pressure is recorded in this position. Three series of exercises are then undertaken, each for one minute or until exhaustion:
Repeated squeezing of a sphygmomanometer bulb Repeated flexion and extension of the wrist holding a 3 kg dumbbell Repeated gripping of a fixed bar and performing an isometric pull with palms facing up and then with palms facing down
The peak pressures achieved during each activity were recorded. We use a threshold for abnormality of 30 mmHg. We do not routinely monitor compartment pressures after cessation of activity. All analyses were performed by the same investigators.
All operations were performed by the same surgeon. A long longitudinal incision down the flexor aspect of the forearm, slightly towards the ulnar side, is used. This ensures visualization of the neurovascular structures and facilitates access to the deep flexor compartment. After incision of the superficial fascia the superficial flexor muscles are retracted radially and the flexor carpi ulnaris ulnarwards with care being taken to protect the ulnar nerve and vessels. The deep fascia overlying flexor digitorum profundus can then be incised.
The extensor compartment is decompressed via a longitudinal incision along the extensor aspect of the forearm starting approximately 7 cm distal to the lateral epicondyle.
Results
Patients with CECS: Demographics, precipitants, compartment pressure measurements and outcome
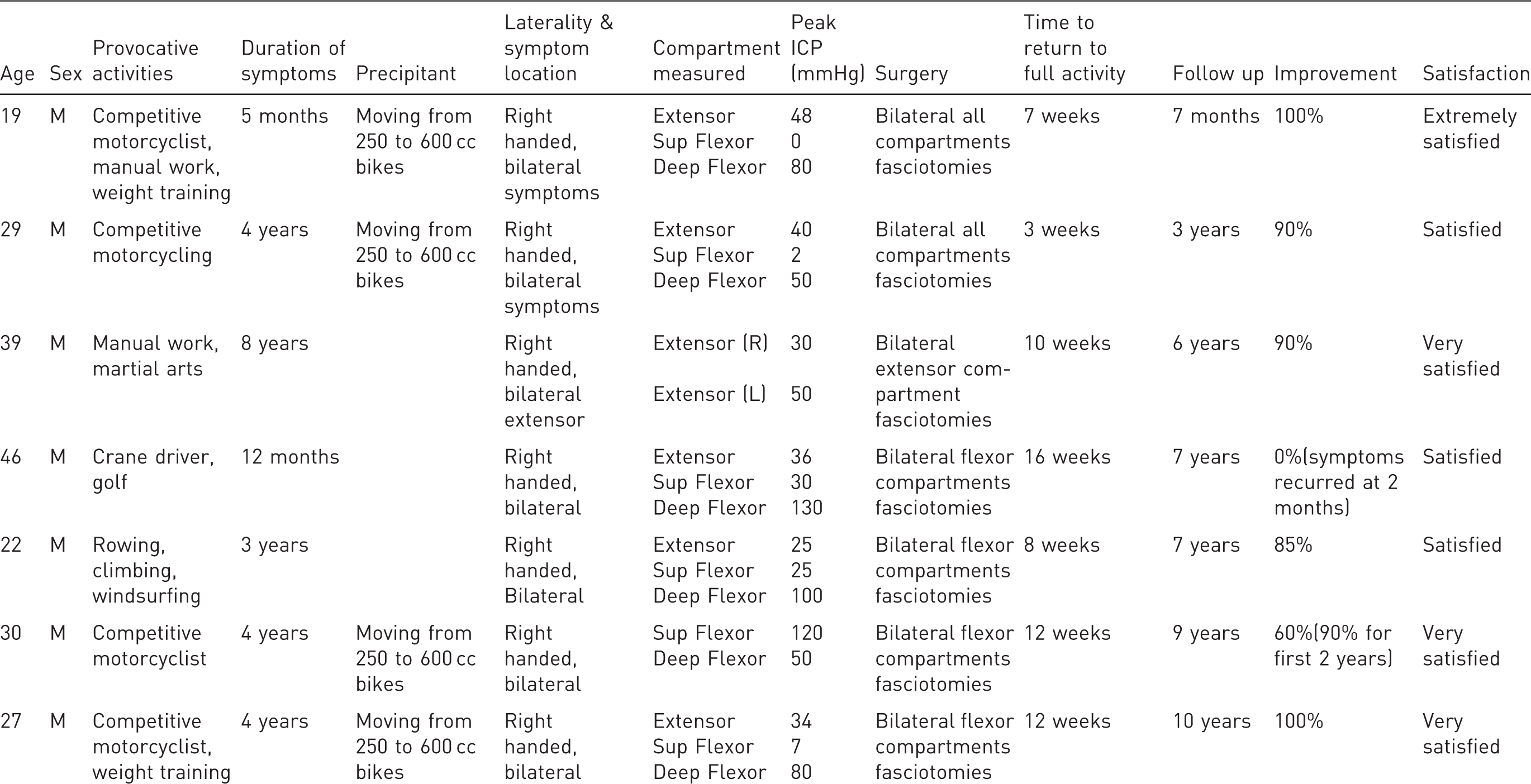
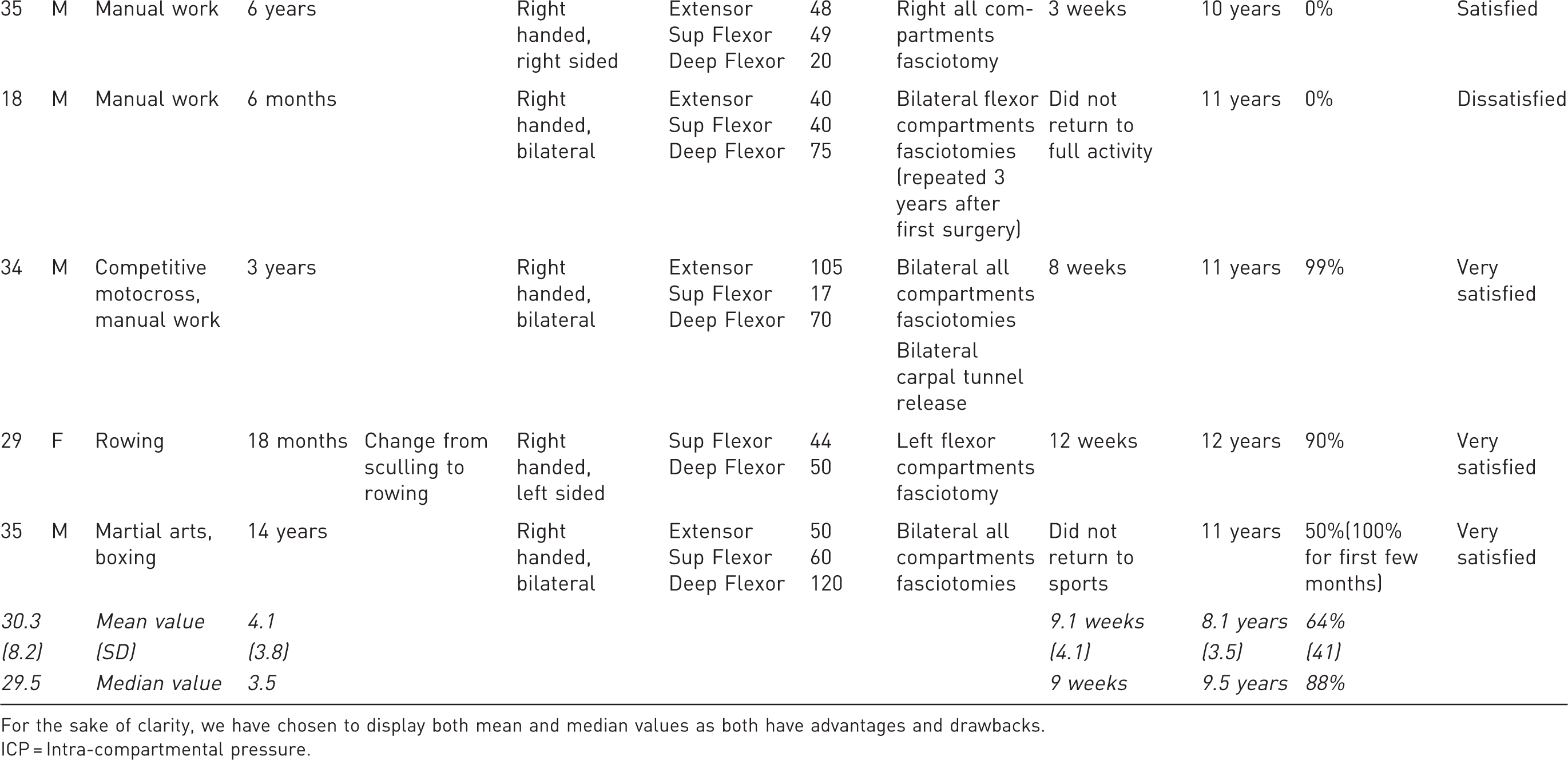
For the sake of clarity, we have chosen to display both mean and median values as both have advantages and drawbacks.
ICP = Intra-compartmental pressure.
The median follow-up was 9.5 years (range 7 months – 12 years). Median patient self-reported percentage improvement after surgery was 88% (range 0%–100%). Ten out of 12 patients returned to their previous level of activity. Median time to return to full activity for these 10 patients was 9 weeks (range 4–12 weeks). Of those that did not return to full activity, one was because surgery did not alleviate the symptoms and the second chose not to return to sports despite experiencing a 50% improvement in his symptoms. This and one further patient reported excellent relief in symptoms for a number of months before noticing a deterioration in improvement to about half of what had been experienced in the initial postoperative period.
Eleven out of 12 patients were satisfied, very satisfied or extremely satisfied with the outcome of their surgery. They included two of the three patients who reported no improvement in their symptoms after surgery. They were happy as they had tried all treatment options even though it had not been successful in curing their symptoms. One of the patients who experienced poor improvement in symptoms went on to have a repeat decompression 3 years after the original surgery and again he felt no improvement in symptoms. This was the only dissatisfied patient in our series.
The patient who was identified with symptoms of CECS of the forearm and raised compartment pressures that chose not to undergo surgery was found to have had no spontaneous improvement in symptoms at 2 year follow-up. He had stopped motocross racing as a result.
Discussion
Although the aetiology of CECS is unclear the condition does appear more commonly in activities requiring repetitive gripping (most notably motorcycling). It is not clear why some individuals develop CECS, while others subjected to similar stresses do not. It is possible that some inherent susceptibility is involved. Garcia Mata et al. (1999) reported bilateral forearm CECS in two brothers and proposed a congenital anatomical predisposition of the compartments might be responsible. This is supported by Wasilewski and Asdourian (1991), who reported the case of a 14-year-old girl who underwent bilateral fasciotomies for forearm CECS but who later developed bilateral lower limb CECS requiring fasciotomy.
Thickened fascia or tight fascial bands have occasionally been noted intraoperatively (Garcia Mata et al., 1999; Hider et al., 2002; Pedowitz and Toutounghi, 1988; Piasecki et al., 2008; Zandi and Bell, 2005) and could, the authors hypothesized, have been be due to previous forearm injury or muscle hypertrophy. Fascial thickening was noted in one forearm in our series. It may have been present in others but not been recorded as being unusual at the time of surgery.
Considerable variation in the measurement and interpretation of intra-compartmental pressures is evident in the literature. Delay in return of intra-compartmental pressures to normal is thought by some authors to be important in the diagnosis of CECS (Garcia Mata et al., 1999; Goubier and Saillant, 2003; Kutz et al., 1985). Although persistently high pressures after exercise have been demonstrated (Garcia Mata et al., 1999; Goubier and Saillant, 2003; Kumar et al., 2003; Kutz et al., 1985; Zandi and Bell, 2005) it is unclear if such protracted testing protocols are superior to those limited to the period of exertion.
Diagnosis is also complicated by the fact that normal pressure ranges for the forearm during and after exercise have not been reliably established. Schoeffl et al. (2004) recorded pressures of 36 mmHg in the flexor compartments of asymptomatic subjects on exercise. Likewise, Rydholm et al. (1983) recorded exercise-induced pressures of 39 mmHg in the extensor compartments. In our department, a peak level of 30 mmHg or more accompanied by typical history and with exclusion of other causes, is taken as diagnostic of CECS. Compartment pressures were often far in excess of this threshold.
This series provides further evidence that fasciotomy can be a very effective treatment for CECS of the forearm. The largest study we have found reported a series of fifteen subjects (Pritchard et al., 2005). However, this dealt only with the extensor compartment. Our series of 12 patients – a total of 22 forearms – significantly increases the number of published cases in which surgical outcome is known. The results of fasciotomy for CECS in the literature are generally good with most patients reporting resolution of their symptoms (Allen and Barnes, 1989; Berlemann et al., 1998; Garcia Mata et al., 1999; Goubier and Saillant, 2003; Kumar et al., 2003; Kutz et al., 1985; Pedowitz and Toutounghi, 1988; Piasecki et al., 2008; Rydholm et al., 1983; Soderberg, 1996; Steinmann and Bishop, 2000; Wasilewski and Asdourian, 1991; Zandi and Bell, 2005). As was found in two previous studies (Pritchard et al., 2005; Rydholm et al., 1983), and also in ours, not all patients recover fully after surgery. Zandi and Bell (2005) also reported the incidence of scar widening over time, in one case up to 10 mm. This was noted by one patient in our series.
As this study is a retrospective analysis involving subjects who had surgery some time ago, estimation of percentage improvement is vulnerable to recall bias concerning the preoperative symptom level. We attempted to check these data against information from medical notes, where available. As many of the patients were professional or semi-professional athletes or unable to work preoperatively, their recollections of the events tended to be detailed. In the absence of a recognized outcome measure we had to rely on patient perception of improvement and their recollections about duration of symptoms and return to activity.
Our experience, and that of Garcia Mata et al. (1999), is that patients with typical symptoms and raised compartment pressures, who choose not to undergo surgery, do not improve and struggle to perform at their pre-morbid level.
A history of forearm overuse due to sports or work involving heavy gripping seem to be important in the development of CECS. It is interesting to note the disproportionate number of motorcyclists (particularly those riding the heavier bikes) presenting with CECS of the forearm. Of note, four of the five motorcyclists in our series reported experiencing problems soon after they started riding heavier bikes. Although there are very few cases of CECS of the forearm in the literature, several of our patients have reported a condition resembling CECS which is referred to as ‘arm-pump’, being well known in the motorcycling community. In addition, Sabeti-Aschraf et al. (2008) in their study of injuries in Enduro motorcyclists found that over 50% had pain in their forearms after riding.
Compartment syndromes are associated with intra-compartmental pressures over the capillary filtration pressure. In motorcycle racing, there is little opportunity for relaxation of the forearm muscles and consequently little chance of pressures dropping to a level to allow capillary filtration (Allen and Barnes, 1989). It is possible that these factors combined with the extra demands of riding a heavier bike might precipitate the onset of CECS. More positively, a trend that has run through this series and the literature is that the outcomes of surgery for this group of patients are usually excellent.
Further work is needed to establish the cause of CECS, to determine an optimal testing protocol and to define normal compartment pressures during exertion.
Footnotes
Conflict of interests
None declared.