
Abstract
We studied self-concept and psychological well-being in children with hand deformities and upper limb deficiencies. Ninety-two children, 53 boys, 39 girls, aged 9–11 years were included. The children were divided into two subgroups – one with milder (less visible) deformities and one with severe (more complex and visible) finger–hand–arm deformities. Of the 92 children, 79 had received reconstructive surgery, and 13 had been treated with prostheses. The Piers–Harris Children’s Self-Concept Scale (PHCSCS) was used to measure self-esteem and well-being. Overall PHCSCS scores showed that the whole hand deformity group had ‘good’ self-concept with mean scores in excess of 60 points, equal to a comparison group of healthy children. Within the hand deformity group, those with mild deformities had lower scores than those with severe deformities. This result was also found in the group of boys but not in the girls. The children with severe deformities had even higher scores than the comparison group regarding the subscale ‘Intellectual and School Status’. The children with milder deformities had lower scores than the comparison group regarding the subscale ‘Popularity’.
Keywords
Introduction
Children born with hand deformities and upper-limb deficiencies often undergo reconstructive surgery or are fitted with hand prostheses early in life. The deformities are clearly visible and the children usually receive quite a lot of medical attention and treatment for these conditions. It is important for the child to have good hand function and decreased ability to use the hands can be frustrating. The literature has given few insights into the role of hand deformities for the psychological well-being of these children and there is a dearth of information on their psychological development and self-concept.
Children with chronic physical disorders have been found to have an increased risk of psychological and social adjustment problems. However, there is considerable variability in individual children’s adaptation to their physical handicap, with some children functioning quite well psychologically and other children exhibiting psychological and social adjustment problems (Wallander et al., 1988).
According to Didierjean-Pillet (2002) “the relationship of the body of the person afflicted with a congenital malformation is a question of aesthetic suffering and not of functional use”. Lukash (2002) writes that children cannot adequately express their feelings about physical issues that may be affecting them emotionally. The hand has a particular psychological and social meaning in addition to its functional importance. It is also an instrument of sensory exploration and intimate contact. The appearance of the hand conveys to others information about a person’s status and life experience. Bradbury et al. (1994) and Argyle (1988) have written extensively on nonverbal communication, and have found that there “is a great deal of bodily movement during social interaction though movements of the hand are most informative”. The hand is difficult to hide from others and from oneself. The functional competence, appearance and sensibility of the hand confront the observer and the observed.
Self-esteem is considered a key aspect of psychological functioning (King et al., 1993). Rosenberg (1985) writes that self-esteem is only one of many dimensions of self-concept and is important at all life stages, but is probably most problematic during adolescence. The importance of having a good self-concept is universally accepted. Appearance or attractiveness is regarded as a major component of self-concept. The importance of appearance is evidenced by its prominence in children’s self-descriptions in the early development of self-concept (Leahy and Shirk, 1985).
A Swedish study of psychosocial adjustment in children with upper-limb reduction deficiency and a myoelectric prosthetic hand showed that this group had social competence and behaviour/emotional problems similar to Swedish standardized norms. However, the girls with upper limb reduction were found to demonstrate lower scores in social competence (Hermansson et al., 2005). In another Swedish study (Strömbeck and Fernell, 2003) activities and participation in daily life were studied in adolescents with another type of unilateral limb impairment – obstetric brachial plexus palsy (OBPP) – and in a comparison group. The main result was that subjects with OBPP had interests and a social life very similar to the age-matched teenagers. Differences were found with respect to sports and motor activities, self-esteem being lower in subjects with OBPP, especially in those with a total palsy.
The purpose of this study was to examine self-concept and psychological well-being in children with congenital hand anomalies who had undergone surgery for hand deformities or had been fitted with myoelectrical prostheses because of upper limb deficiencies.
Method
Study group
We assessed all mainstream classroom children, born to Swedish parents, who were referred for surgical treatment because of hand deformities or for fitting with myoelectric prostheses before age 10 years at the Sahlgrenska University Hospital in Gothenburg. Data collection started in 1994 and was continued over 10 years. There were 92 children of whom 79 had received reconstructive surgery (28 of whom had also been treated with orthoses), and 13 had been treated with prostheses.
The reason for including only mainstream classroom children born to Swedish parents was the need to recruit a group of children – without major intellectual problems or Swedish language problems – who would be able to complete the self-report of a questionnaire.
Informed consent
All parents provided written informed consent for their child to participate in this study.
The children in the study group were subdivided into two subgroups – a) ‘Mild’ (simple) deformities (n = 35) e.g. pollicis duplex, triphalangeal thumbs and syndactyly, often treated early with one surgical procedure and with a cosmetic result close to normal; and b) ‘Severe’ (complex) deformities (n = 57) e.g. reduction anomalies at finger–hand level, longitudinal reduction anomalies, often treated with several surgical procedures, and transverse reduction anomalies treated with myoelectrical prosthesis. In this group the deformity was still obvious even after treatment.
Comparison group
The comparison group was of similar Swedish children aged 9–13 years old taken from Gothenburg mainstream classrooms. They represented all 9–13-year-olds from a comparison group of 9–18-year-olds included in a controlled study of the self-concept of children with infantile hydrocephalus, the detailed results of which have been published elsewhere (Fernell et al., 1992). This group had been examined a few years before the study of the children with hand deformities took place.
Measurements
Subscales on the PHCSCS
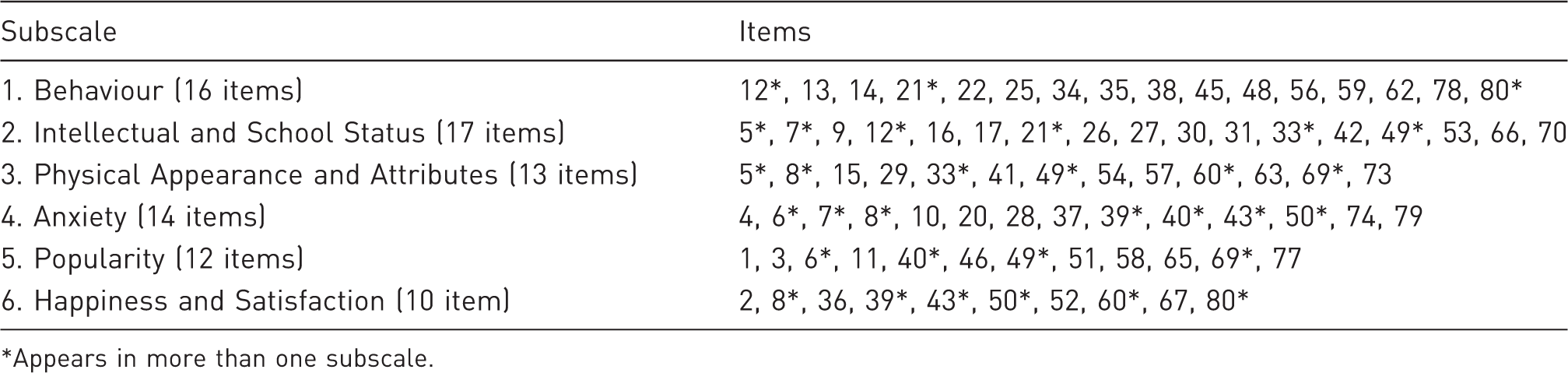
Appears in more than one subscale.
Total score cut-offs for levels of self-concept as recommended by the Piers–Harris manual are: ‘poor’ self-concept <40; average 40–60; and ‘good’ >60 (Piers and Harris, 1984). The PHCSCS takes about 20 minutes to complete. It has been developed for use with children and adolescents aged 8–18 years. It is unsuitable for younger children or children with verbal or comprehension problems. The PHCSCS is considered a highly reliable and valid instrument with test–retest reliability ranging from .42 to .96, internal consistency from.88 to.93, and correlations of.32 to.85 with other measures of self-concept (Piers and Harris, 1984). It was developed as a research instrument and is used to investigate the relationship between self-concept and other psychological traits. The PHCSCS used in the present study was translated into Swedish by Professor Lennart von Wendt (Fernell et al., 1992).
All study group children were given the PHCSCS by the same occupational therapist in connection with follow-up of surgical outcome around the age of 10 years (9–11 years). The child completed the questionnaire himself/herself but could ask either the occupational therapist or parents if he/she did not understand a particular question.
Statistical analysis
For comparison of continuous variables, both total scores and subscale scores, between two groups, a Mann–Whitney U-test was used. For comparison of categorical variables, that is frequencies of ‘yes’ or ‘no’ scores on individual items, between two groups, a chi-square test was used. Yates’ continuity correction was applied when the expected value in a two-way table was less than five. All tests were two-tailed and conducted at 5% significance level. P-values <0.05 were considered statistically significant. Due to multiplicity comparisons the upper limit for expected number of false significances is given for each table.
Results
In the study group there were 92 children (53 boys, 39 girls) aged 9–11 years, mean 10.6 (SD 0.8) years. In the comparison group there were 49 children without hand deformities (21 boys, 28 girls), aged 9–13 (mean 11).
Overall PHCSCS score
Overall and subscale scores in children with mild/severe hand deformities and comparison group
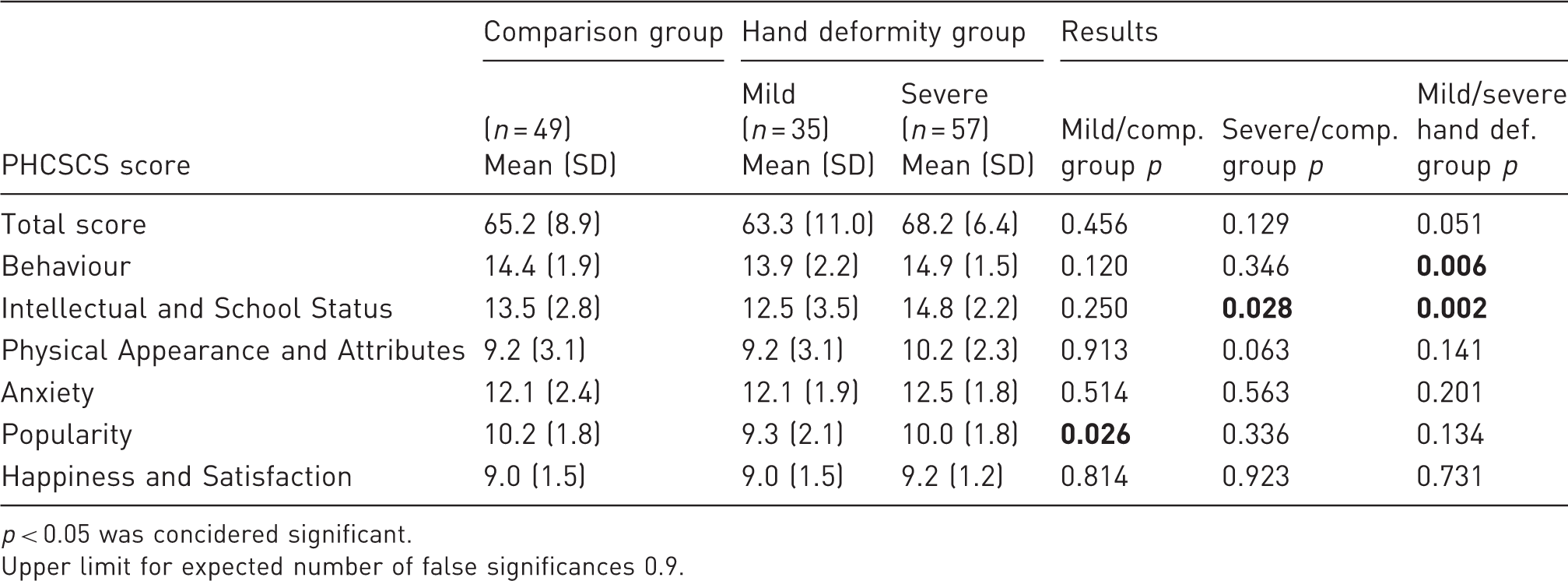
p < 0.05 was concidered significant.
Upper limit for expected number of false significances 0.9.
Within the hand deformity group, the mild deformity group showed lower total scores (mean 63.3, SD 11.0) than the severe group (mean 68.2, SD 6.4) (Table 2). However, the p-value was just above significance level (p = 0.051).
Subscale scores
Considering all six subscales in PHCSCS, there were no significant differences between the total hand deformity group and comparison group.
However, between the mild and the severe hand deformity groups, there were significant differences according to two subscales. The ‘Behaviour’ subscale mean score was significantly lower in the group with mild hand deformities (p = 0.006) (Table 2).
Rates of positive answers on subscale items in groups with mild and severe hand deformities
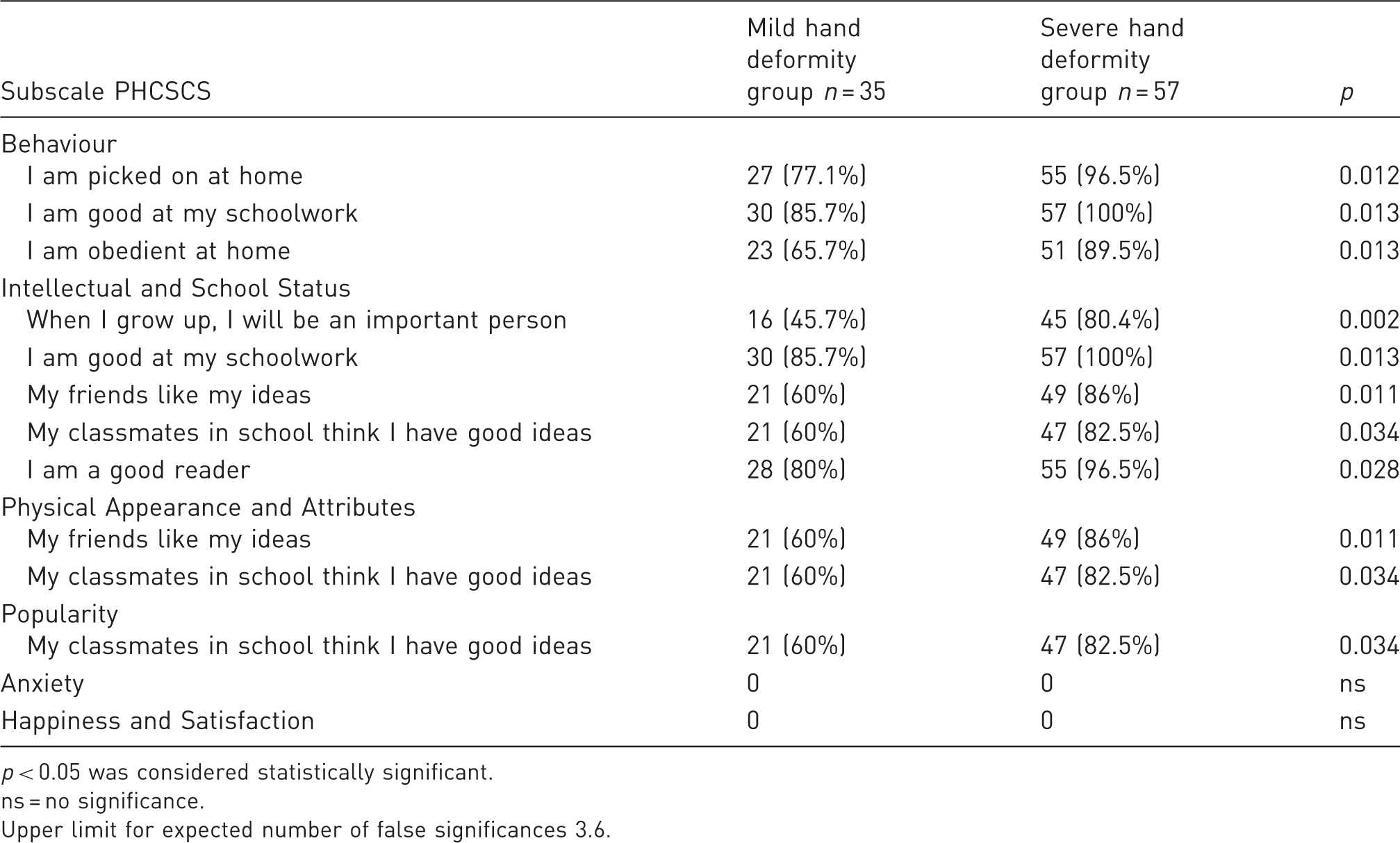
p < 0.05 was considered statistically significant.
s = no significance.
Upper limit for expected number of false significances 3.6.
The ‘Intellectual and School Status’ subscale mean score was also considerably lower in the group with mild deformities versus the group with severe hand deformities (p = 0.002) (Table 2). Several endorsed problems contributed towards this overall result: ‘When I grow up, I will be an important person’, ‘I am good in my school work’. ‘My friends like my ideas’, ‘My classmates in school think I have good ideas’ and ‘I am a good reader’ (Table 3).
As regards the subscale ‘Popularity’ one item ‘My classmates in school think I have good ideas’ gave lower scores in the mild deformity group compared to the severe deformity group (p = 0.034), but this single item did not influence the total subscale scores enough to produce a significant difference between the groups with mild and severe deformities. Also in subscale ‘Physical Appearance and Attributes’ two items were found to give lower scores in the mild deformity group, ‘My friends like my ideas’ and ‘My classmates in school think I have good ideas’ (Table 3).
We did not find significant differences between the mild and the severe hand deformity groups in the ‘Anxiety’ and ‘Happiness and Satisfaction’ subscale mean scores (Table 2).
When comparing the severe hand deformity group with the comparison group, we found significant differences regarding subscale ‘Intellectual and School Status’ (p = 0.028) with surprisingly higher scores for the severe deformity group than for the comparison group. However, comparing the mild deformity group with the comparison group a significantly lower mean score (p = 0.026) was found in the mild deformity group for the subscale ‘Popularity’ (Table 2).
Effects of gender
Differences between boys and girls with hand deformities: There was no difference between boys and girls in the total hand deformity group. When comparing boys and girls with only severe hand deformities the girls had significantly lower scores than the boys regarding two subscales, ‘Anxiety’ (p = 0.032) and ‘Happiness and Satisfaction’ (p = 0.047). However, the girls within the comparison group also had significantly lower scores for ‘Anxiety’ than the boys (p = 0.020).
Differences between boys with mild and severe hand deformities: Boys in the mild hand deformity group scored significantly lower total PHCSCS scores (p = 0.018) than the boys in the severe hand deformity group. There were differences across the mild and severe hand deformity groups on three of the subscales: ‘Behaviour’ (p = 0.037), ‘Intellectual and School Status’ (p = 0.001) and ‘Physical Appearance and Attributes’ (p = 0.040), with the mildly affected group invariably showing lower scores. In comparison with boys in the comparison group, boys in both hand deformity subgroups had lower scores on the ‘Popularity’ subscale: mild deformity group (p = 0.009); and severe deformity group (p = 0.048).
Differences between girls with mild and severe hand deformities: Amongst girls there were no significant differences between the mild and severe hand deformity groups on any PHCSCS subscale mean score. Neither were there any differences between total or any subscale scores when girls in the mild and severe hand deformity groups were contrasted with girls in the comparison group.
Individual items on PHCSCS subscales by severe and mild hand deformities status: Out of the 80 items in the PHCSCS, seven revealed differences between the severe and mild hand deformity subgroups (Table 3). The severe hand deformity group invariably had a more positive response on these seven items. For example on item ‘When I grow up I will be an important person’, 80% of the children with severe hand deformities had a positive response compared to 46% of the children with mild deformities.
Discussion
The Piers–Harris Children’s Self-Concept Scale (PHCSCS) is a well established instrument for measuring self-concept and well-being in children (Piers and Harris, 1984). Most studies using the PHCSCS in children with disability have been carried out on children with diagnoses involving abnormalities of the head and face, or of the whole body. These include Apert syndrome (Lefebvre et al., 1986), hydrocephalus (Fernell et al., 1992), cleft lip and/or palate (Leonard et al., 1991) and Noonan syndrome (Lee et al., 2005). To our knowledge, this is the first systematic study of self-concept with Piers–Harris assessments of school age children who have undergone surgery for hand deformities or upper limb reductions.
By and large, self-concept appears to be good in this group. When contrasted with a healthy comparison group of Swedish children, no significant differences on Piers–Harris total or subscale scores were found. However, this conclusion needs to be tempered by the fact that the comparison group was rather small (n = 49), slightly older (9–13 years, compared to 9–11 years in the surgery groups), and it had been examined under slightly different circumstances some years prior to the examination of the surgery group.
Nonetheless there were differences between the mild and severe hand deformity groups with significantly lower scores in the mild deformity group for two subscales. On seven of the 80 items, the group with mild hand deformities had lower scores than the group with severe hand deformities. These items represent what children assume that another person might be thinking about them, what they themselves think about the future, and what they think about themselves. All these items reflect concepts which are very important for the development of self-esteem.
Boys in the mildly affected group had significantly lower self-esteem than boys in the severe hand deformity group both for total PHCSCS scores and on the subscales ‘Behaviour’, ‘Intellectual and School Status’ and ‘Physical Appearance and Attributes’. One possible explanation for this could be that boys with severe hand deformities would try to compensate for their physical limitation by achieving better results in school.
Girls with severe hand deformities showed lower self-esteem than boys on the subscales ‘Happiness and Satisfaction’ and ‘Anxiety’. The difference in the ‘Anxiety’ scores was similar to that found between boys and girls within the comparison group. No significant difference in scoring was seen comparing girls with mild or severe deformities with the comparison group. However, boys with hand deformities had significantly lower scores in the subscale ‘Popularity’ than boys in the comparison group. It appears that boys suffered more than the girls regarding self-esteem as reflected by subscale ‘Popularity’, compared to the comparison group. The pattern of lower scores for milder versus severe deformities, seen in the overall group of children with deformities, was very similar to that seen among boys. No such difference was seen in the group of girls. It appears that the girls were generally more stable regarding their self-esteem except for the group with severe deformities which scored lower than the boys for ‘Happiness and Satisfaction’.
The results of this study indicate that children with hand deformities in this age group generally have as high self-esteem as children in a comparison group. However, children with mild hand deformities have poorer self-concepts than those with severe deformities. Surprisingly the group with severe deformities scored even higher than the comparison group regarding the subscale ‘Intellectual and School’ which might be explained by a compensation mechanism regarding school-work. The children with mild deformities showed lower self-esteem than the comparison group as well as the group with severe deformities. Whilst this finding may at first seem surprising it is explicable. Clinical experience suggests that children with severe deformities receive a lot of sympathy and understanding from the very beginning. It is impossible to ‘hide’ the disability and the handicap is obvious both to the child and the people around them. Other studies of children with different kinds of impairments have also reported average or above average self-esteem among those who received psychological support by a specialized team (LeDoux et al., 1996). Children with milder disabilities may appear to be ‘almost normal’ and they – and their parents – may want to hide the deformity. Both the lack of extra support/sympathy and the attempts to ‘hide/dismiss’ the deformity may contribute to poor self-concept.
Varni et al. (1989; 1991; 1992) studied perceived physical appearance in children with congenital/acquired limb deficiencies and found that higher levels of perceived social support, peer acceptance and scholastic and athletic competence were associated with higher perceived physical appearance.
We found overall levels of self-esteem and well-being to be good in children with hand deformities. Nevertheless, those with milder deformities had considerably poorer self-concepts than those with severe deformities, and this tended to be particularly true for the boys. These findings need to be considered when services for children with hand deformities are developed in order to take into account the psychological and social aspects of the condition.
Footnotes
Acknowledgements
We are grateful for statistical support by Nils-Gunnar Pehrsson and Bengt Bengtsson, Statistiska Konsultgruppen, Gothenburg.
Funding
This study was supported by grants from Felix Neubergs stiftelse, Gothenburg and FoU in West Sweden.
Conflict of interests
None declared.