
Abstract
Complex regional pain syndrome type I (CRPS-I) is a known complication after surgery or trauma to the upper extremity and is difficult to treat. A simple and easily tolerated method of treatment that includes intravenous regional anaesthetic block with lidocaine and methyloprednisolone is presented. One hundred and sixty-eight patients with CRPS-I of the upper extremity were treated in a 5-year period. At the end of treatment 88% of the patients reported minimal or no pain. After a mean follow-up of 5 years (range 28 months to 7 years) complete absence of pain was reported by 92% of patients. The symptoms of the acute phase of the syndrome were reversed. Early recognition and prompt initiation of treatment is very important for the course of the disease as symptoms can be reversible when treatment starts early. Permanent results with a functional upper extremity and very satisfactory pain relief can be anticipated.
Keywords
Introduction
Complex regional pain syndrome type I (CRPS-I) is a well known complication that occurs after trauma or surgery involving mainly the upper extremity but often the lower extremity as well (Marshall and Crisp, 2000; Poplawski et al., 1983; Zyluk, 2004). Trauma is the most common cause. This includes fractures, sprains, dislocations, skin lacerations, contusions, crushing injuries of the wrist, hand or fingers, and burns. Independently from the causing factor, CRPS-I can be defined as a situation in which the patient suffers from diffuse burning pain in the affected extremity secondary to injury with variable motor, sensory, and trophic changes (Albazaz et al., 2008; Harden and Bruehl, 2006).
Clinical experience shows that there is not always a strong correlation between severity of trauma and intensity of symptoms accompanying the syndrome (Atkins et al., 1990; Bickerstaff and Kanis, 1994; Kleinert et al., 1973). The syndrome manifests with severe burning pain, hyperesthesia, weakness, atrophy of muscle and skin, vasomotor instability, and osteopenia of the affected part of the body (Albazaz et al., 2008; Harden and Bruehl, 2006).
Recognition of CRPS-I is very important because treatment should start as early as possible. In an early phase all symptoms and pathologic findings can be completely reversible. If the condition proceeds it may not respond to any therapeutic act, and the symptoms and pathologic changes may become permanent (Bickerstaff and Kanis, 1994; Zyluk, 1998a).
Many modalities and protocols of management have been implicated in the treatment of this syndrome with various results regarding efficacy and patient satisfaction (Albazaz et al., 2008; Bickerstaff and Kanis, 1991; Linson et al., 1983; Mockus et al., 1987; Perez et al., 2010; Soucacos et al., 1998; Tountas and Noguchi, 1991; Zyluk, 1998b). Intravenous regional blockades were found to achieve a significant reduction in pain but their side effects can sometimes be difficult for the patient to tolerate (Hanna and Peat, 1989; Hord et al., 1992). The aim of this study is to evaluate the long-term results of a simple method of treatment for Complex Regional Pain Syndrome type I of the upper extremity in a significant number of patients with intravenous regional anaesthesia using lidocaine and methyloprednisolone immediately after recognition of the syndrome during its first stage. It also aims to emphasize the importance of the early diagnosis and treatment of CRPS-I.
Methods
One hundred and sixty-eight patients with CRPS-I of the upper extremity were treated from 2003 to 2007. Ninety-one patients were women and 77 were men with an average age of 53 (range 19–78) years.
Patients were classified into three groups: Seventy-four patients (first group) had post-traumatic CRPS-I (trauma not requiring surgery), 61 patients (second group) had post-surgical CRPS-I after trauma and 33 patients (third group) had post-surgical CRPS-I after elective surgery of upper extremity. The first group included patients with a history of distal radius fracture, wrist or metacarpal fracture, and patients with minor injury or skin trauma that did not require operative treatment. The second group included patients who underwent surgical procedures after trauma/injury including internal and external fixation for fractures of the hand and wrist, tendon and nerve repair, degloving injuries of the hand and forearm, and crushing injuries of the hand. The third group included patients who underwent various elective surgical procedures in the hand or forearm including carpal tunnel release, palmar fasciectomy for Dupuytren’s contracture, and extensor compartment release for DeQuervain’s tenosynovitis. For the above reasons patients were initially treated in five different institutions. All patients were treated for the CRPS-I in the authors’ institution. The other four institutions referred the patients with suspected CRPS-I to the authors’ institution after initial treatment for their trauma or index surgery.
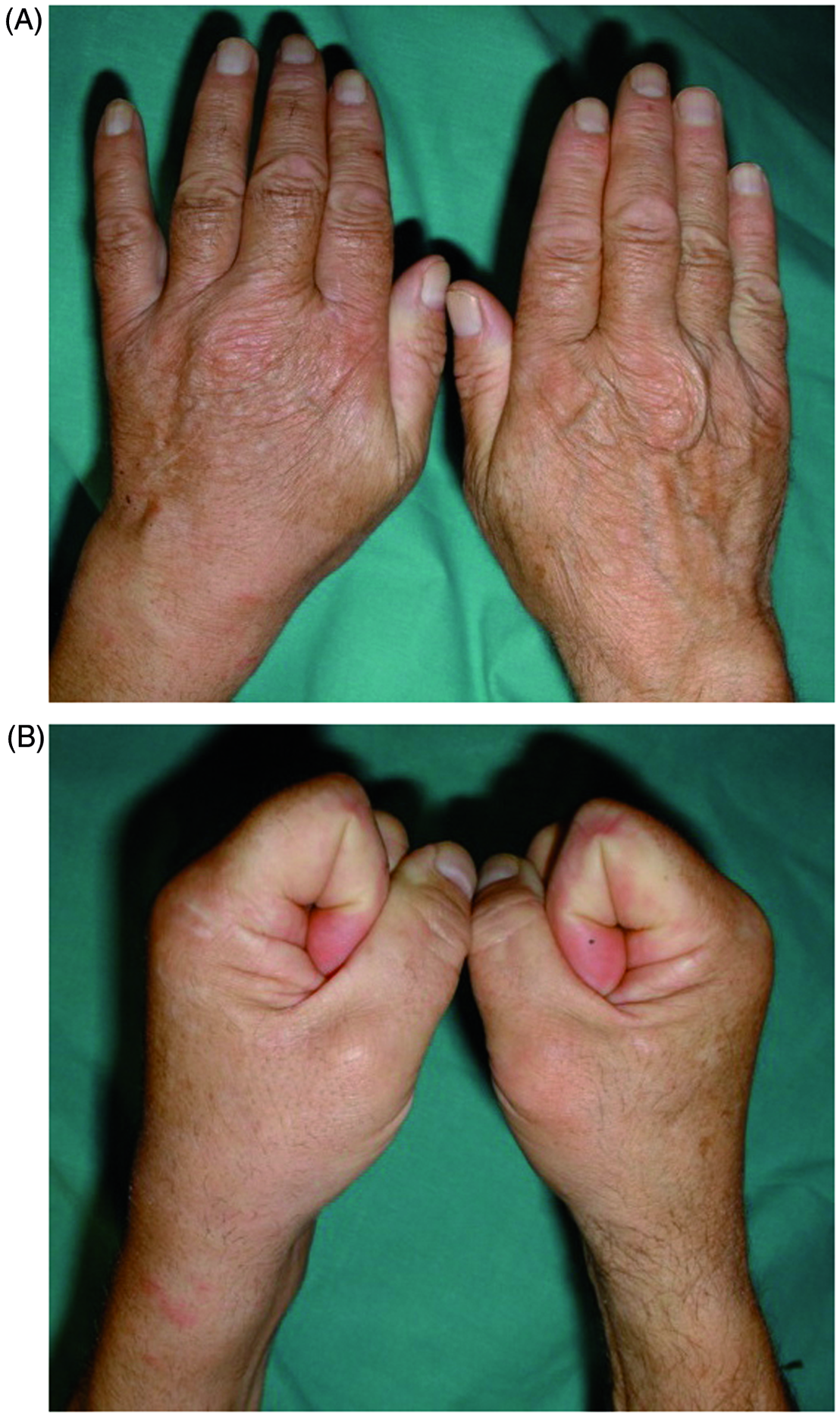
The diagnosis for CRPS-I was made early after its onset (2–6 weeks, with an average of 4 weeks after the initial trauma or surgical procedure) during the first stage of the disease. The treatment was initiated immediately after the diagnosis of CRPS-I in all patients. The patients presented with a variety of symptoms and signs including unexplained diffuse pain, diffuse oedema/swelling, difference in skin colour relative to other limb with reduced ability to wrinkle, difference in skin temperature relative to other limb, hair growth changes, sensory disturbances (evaluated by two-point discrimination test) and stiffness (reduced motion) of the affected hand (Figure 1) (Merskey and Bogduk, 1994; Veldman et al., 1993). Pain was the cardinal complaint of all patients before initiation of treatment. A three-phase bone scan that has been reported for confirmation of diagnosis of CRPS-I was not used in this study (Albazaz et al., 2008; Tountas and Noguchi, 1991; Turner-Stokes, 2002). The diagnosis was based strictly on clinical criteria.
Reflex sympathetic dystrophy in a patient who underwent elective surgery for carpal tunnel release of the left hand one month ago. (A) Extension and (B) flexion of the fingers.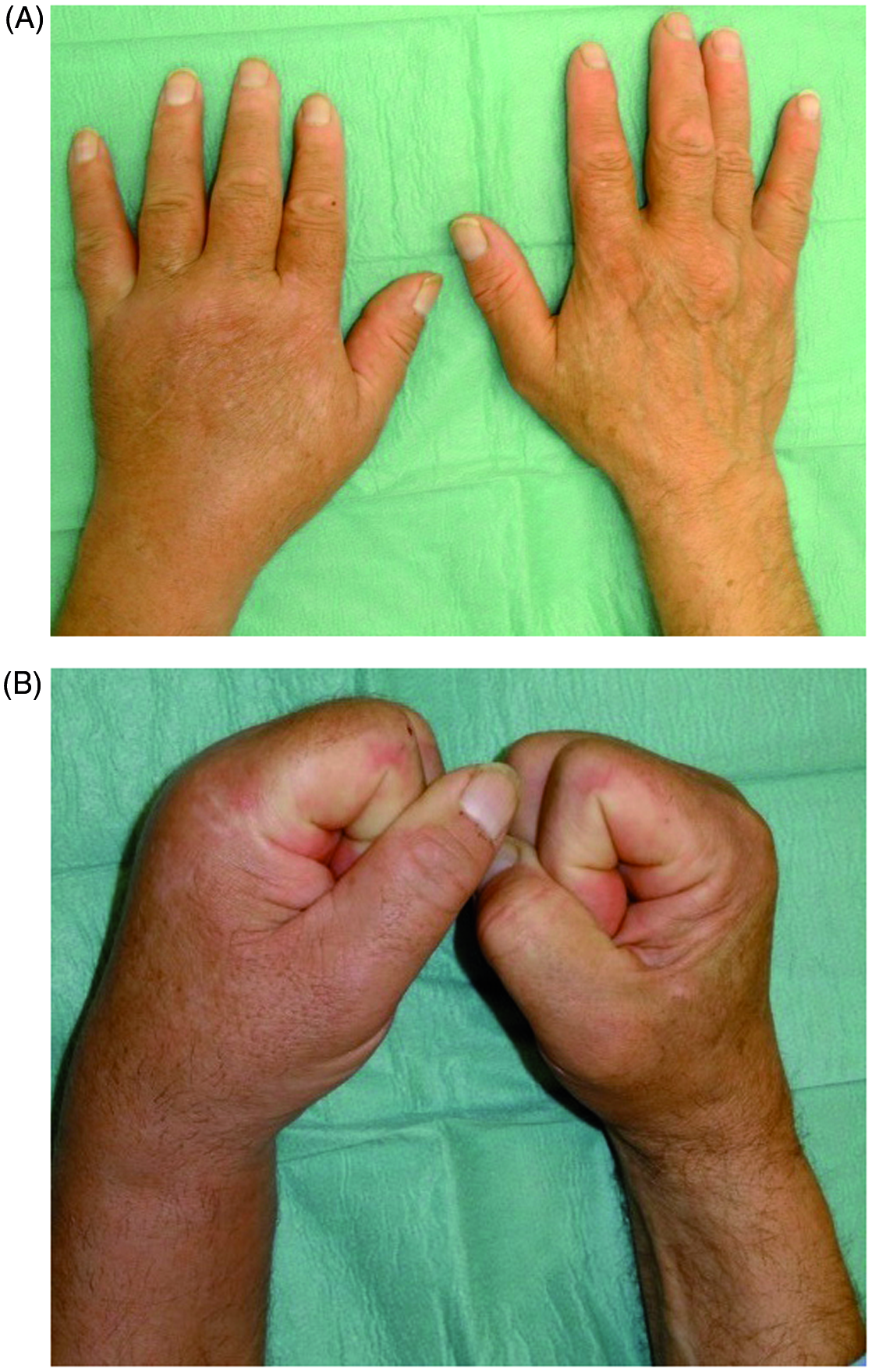
Patients were evaluated before treatment with subjective and objective criteria by the first three authors (S.E.V., L.K.P., and Z.H.D.). Range of motion (ROM) in the hand was evaluated with measurement of the total active motion (TAM) for each finger. Two-point discrimination and grip strength were also documented for objective evaluation. Patients were instructed before treatment on the use of a visual analogue scale (VAS) from 0 to 10 for rating severity of pain (subjective evaluation). A score based on the criteria proposed by Zyluk (2003) was also obtained for every patient. According to this system the following signs and symptoms are considered to be significant: pain, reduction of finger flexion, swelling, temperature changes, discoloration, sensory disturbances, shoulder pain and loss of movement, increased sweating, and hair/nail growth changes. The same preoperative parameters were evaluated after the end of treatment (1 week after the last session) and at the final follow-up (mean 5 years) by the same first three authors.
Total active motion (TAM) of the fingers averaged 119° (from 105° to 130°). Grip strength was measured with a Jamar hand dynamometer (Jamar; Sammons Preston, Inc.) at an average of 17 lb (from 12 to 25 lb). Two-point discrimination ranged from 3 to 10 mm with an average of 5 mm. Patients rated their pain from 2 to 9 with an average of 4.8 in the VAS.
The distribution of symptoms and signs in patients before the treatment
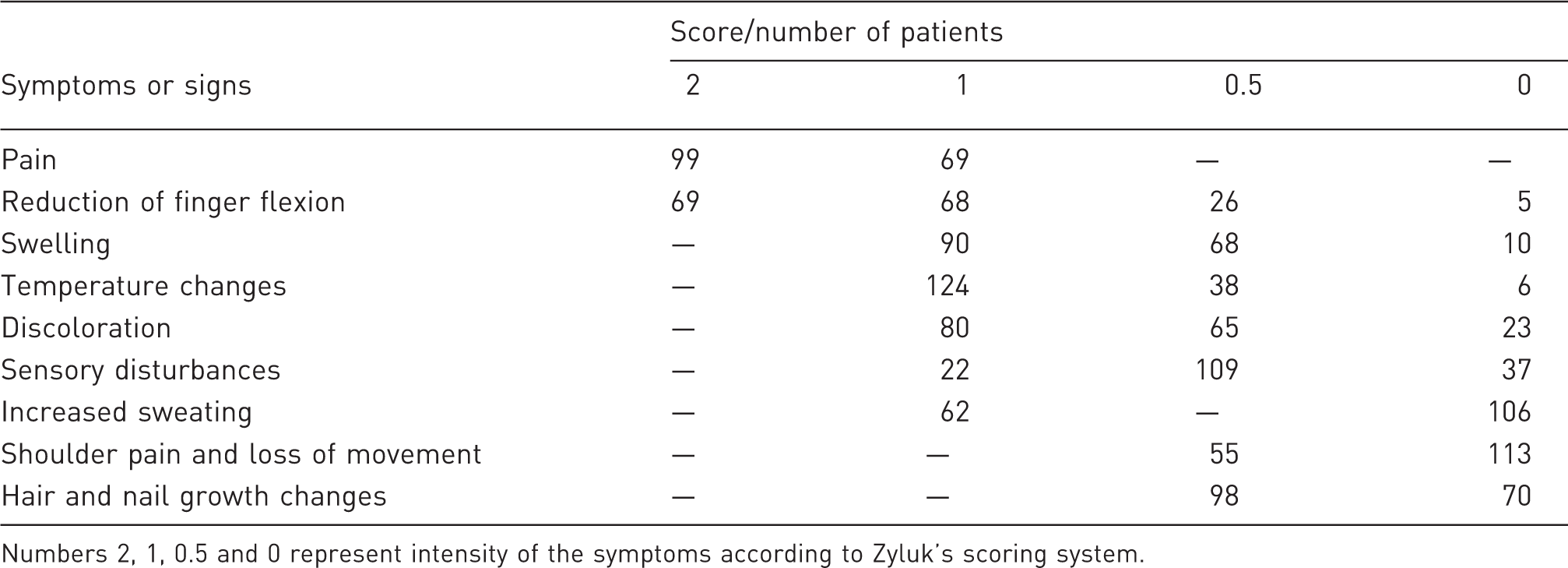
Numbers 2, 1, 0.5 and 0 represent intensity of the symptoms according to Zyluk’s scoring system.
Treatment consisted of intravenous regional anaesthesia using lidocaine and methyloprednisolone performed in an out-patient system. The blocks were performed by all authors. In all patients a catheter was inserted in the vein in the affected extremity in the dorsal hand or the distal forearm. Patients were taken into the recovery room of the operating theatre and were placed under monitoring control. The affected extremity was exsanguinated with an elastic bandage and a tourniquet was applied. With the tourniquet inflated (100 mmHg plus the systolic blood pressure of patient), 25 ml of lidocaine 0.5% and 125 mg of methyloprednisolone diluted in 10 ml of normal saline were injected (Figure 2) as suggested by Soucacos et al. (1997; 1998) and Tountas and Noguchi (1991). The tourniquet was kept inflated for 20 minutes and then it was gradually deflated, to avoid massive entrance of the injected agents in the circulation. During this period when the extremity was anaesthetized we manipulated the stiff hand and fingers in order to gain more motion. The same process was repeated once or twice a week depending on intensity and persistence of the patient’s symptoms. An average of 4.8 sessions (from a minimum of 3 to a maximum of 6) was needed to relieve the symptoms and provide a functional extremity. Between sessions patients were kept under mild physical therapy, which was not prolonged and not stressful. Analgesics were regularly administered to all patients (1g of paracetamol per day between sessions).
The solutions of methyloprednisolone and lidocaine (diluted in normal saline) are injected through a vein in the hand, after the limb has been exsanguinated and the tourniquet inflated.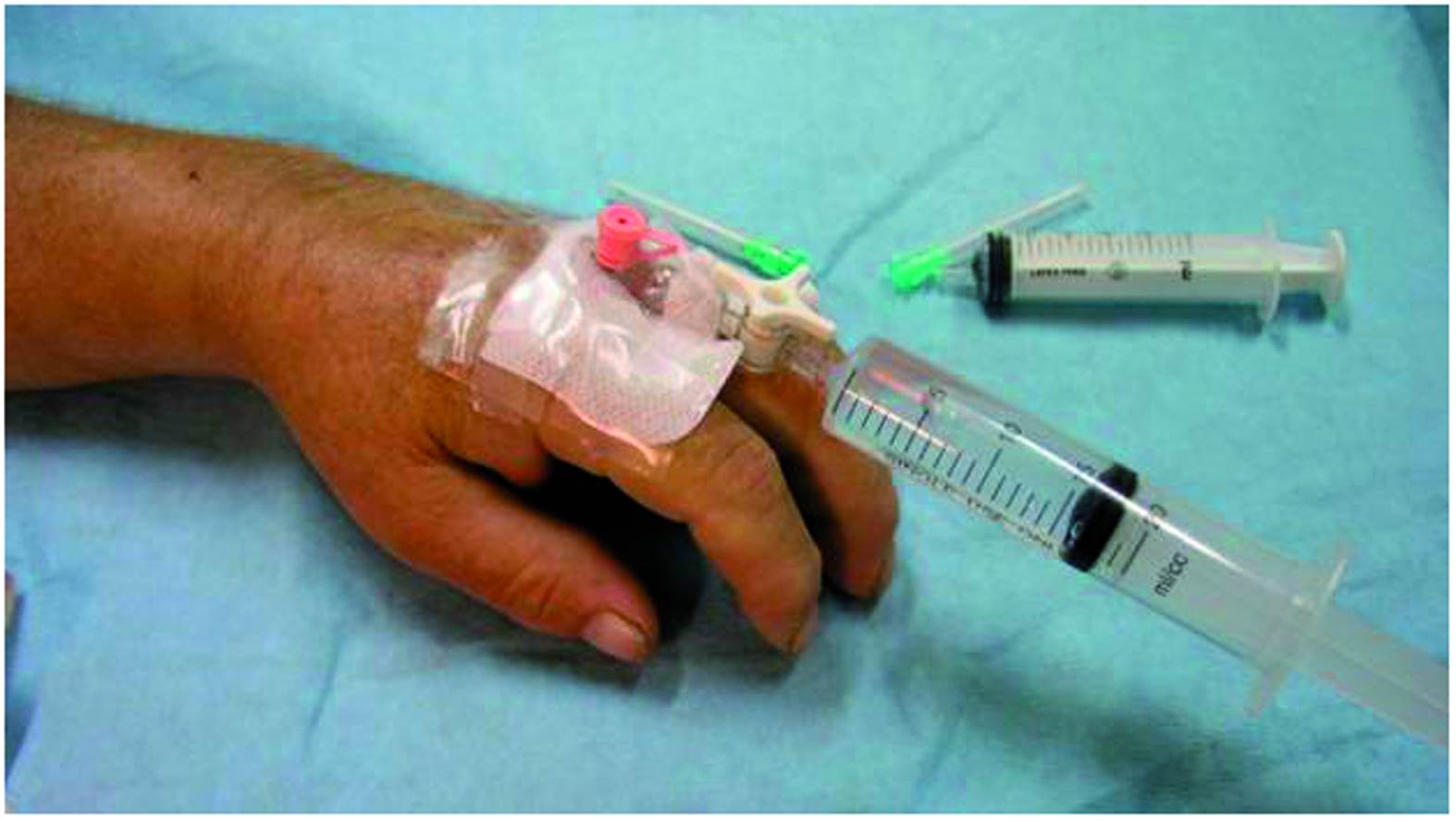
Results
Twelve patients (7%) did not tolerate the tourniquet ischaemia for 20 minutes and the tourniquet needed to deflate between 14 and 17 minutes in their sessions. No patient presented any adverse effects related to the procedure and the entrance of lidocaine and methyloprednisolone in the circulation.
A minimum follow-up of 28 months was required for a patient to be included in the study. Follow-up ranged from 28 months to 7 years with an average of 5 years. At the end of treatment (1 week after the last session) total active motion (TAM) was measured at 205°. Two-point discrimination remained normal and ranged between 3–8 mm, with an average of 4 mm. Grip strength was 42 lb. This was two and a half times the initial value but still only 60% of the unaffected extremity.
One hundred and forty-eight patients (88%) reported minimal or no pain (0–2) on a scale of 10) at the end of their treatment (1 week after the last session). Twenty patients (12%) rated their pain at 3–4 on a scale of 10 (VAS score). These patients, before treatment, rated their pain at 6–8 on a scale of 10. After the last session these twenty patients occasionally received analgesic (paracetamol).
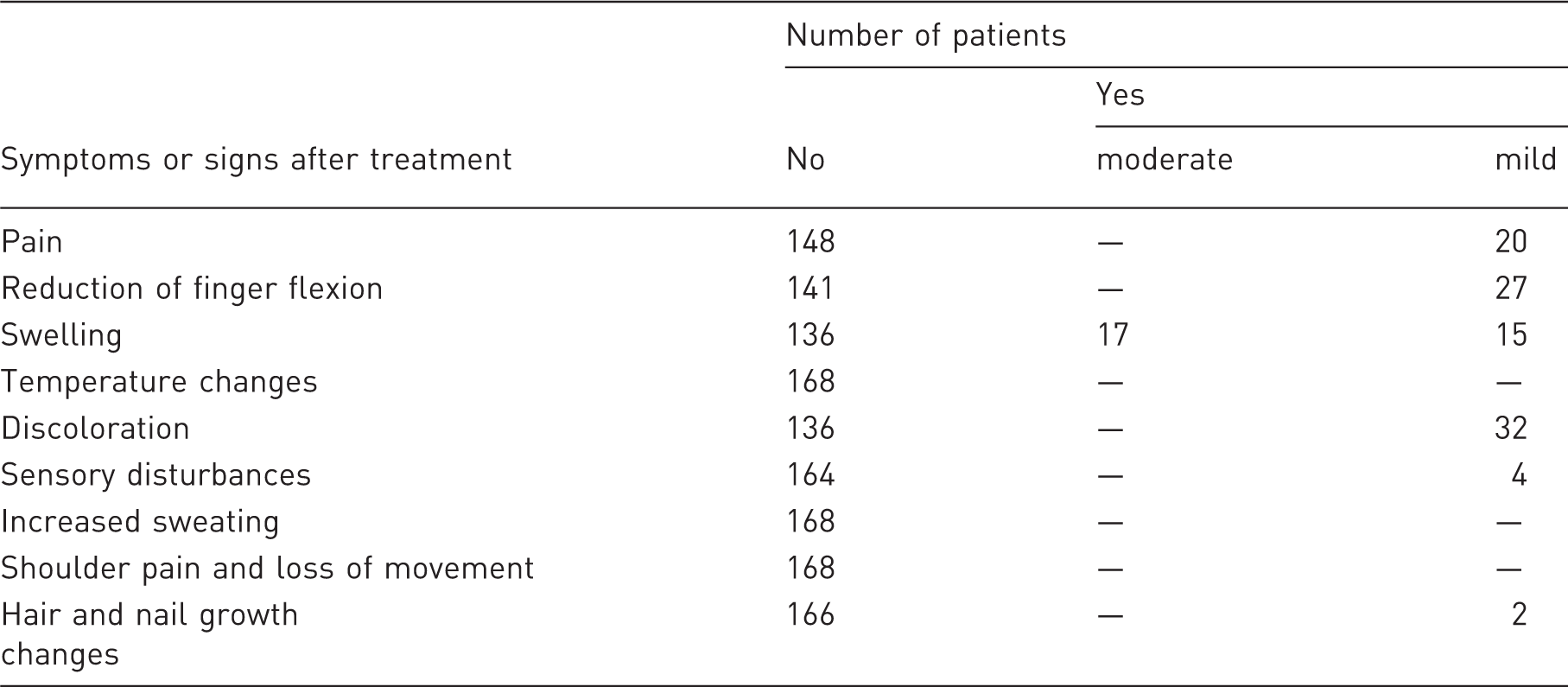
The distribution of symptoms and signs in patients after the treatment
A and B. The same patient after four sessions of intravenous regional anaesthesia with lidocaine and methyloprednisolone. Swelling is minimal and flexion of the fingers normal.
At the final follow-up of the study (mean 5 years) 146 patients (86% of the total number) presented for re-evaluation. Twenty-two patients were not found due to various reasons. Total active motion was measured at 210°. A reason for the reduced TAM (normally 270°) is that trauma or a condition that caused CRPS-I could also render a reduced TAM. Two-point discrimination averaged 4 mm and grip strength increased to 60 lbs. One hundred and thirty-four patients (92%) reported no pain and only 12 patients reported mild pain (1 to 3 in the Visual Analogue Scale) for which they occasionally received analgesics. According to the scoring system proposed by Zyluk no patient had a score greater than 2.
Discussion
Various methods and agents like drugs, nerve blocks (stellate ganglion block, a supraclavicular, an infraclavicular, or an axillary block), surgical or chemical sympathectomy, physical therapy and psychological consultation can be used for treatment of CRPS-I. Many drugs have been used orally for treatment of CRPS-I including analgesics, anxiolytics, antidepressants, muscle relaxants, non-steroidal anti-inflammatories, neurolytics, vasodilators, calcitonin etc. (Bickerstaff and Kanis, 1991; Perez et al., 2010).
Intravenous regional block (Bier’s block) is another efficient method of treatment for CRPS-I. Agents that are injected include lidocaine (Perez et al., 2010; Soucacos et al., 1998) and cortisone (Perez et al., 2010; Soucacos et al., 1998; Taskaynatan et al., 2004; Tountas and Noguchi, 1991; Zyluk, 1998b). Intravenous regional anaesthesia using reserpine and guanethidine provides good results but adverse effects, with various severity and intensity, related to these two agents (Blanchard et al., 1990; Eulry et al., 1991; Hannington-Kiff, 1974; Livingstone and Atkins, 2002).
Studies with intravenous regional blocks have provided various results. Paraskevas et al. (2006) studied the outcome of the treatment of CRPS-I of the hand in 17 patients with intravenous regional sympathetic blocks using guanethidine and lidocaine. They reported very satisfactory result in their patients after a series of 25 sessions (in almost 3 months) for each patient. Their follow-up ranged from 15 to 33 months with an average of 2.1 years.
Tountas and Noguchi (1991) evaluated the effect of intravenous regional blocks with 80 mg methyloprednisolone and 20–40 ml of 0.5% lidocaine in 17 patients with post-traumatic CRPS-I (12 upper extremity, 5 lower extremity). The number of intravenous blocks given ranged from one to four (average 2.4). Assessment of these patients showed that 11 patients had total or almost total relief of their symptoms at 6 months and at the last follow-up (average 28 months).
Similarly, Taskaynatan et al. (2004) investigated the effect of intravenous regional block with 40 mg methylprednisolone and 10 ml of 2% of lidocaine in 22 patients with stage II of CRPS-I. Each patient underwent three sessions at the most. They found that this intravenous regional block resulted in significant pain relief 1 h after the block but did not provide long-term benefits in CRPS-I.
In our study, we evaluated a significant number of patients with CRPS-I of the upper extremity after treatment with intravenous regional block using 125 mg methylprednisolone and 25 ml of 0.5% lidocaine. All 168 patients were in the early stage I of CRPS-I and underwent an average of 4.8 sessions (from a minimum of 3 to a maximum of 6) of blocks. We found that very satisfactory results (relief of pain and restoration of range of motion) were achieved at the end of treatment (1 week after last session). It is interesting to note that 146 patients continued to present this clinical improvement until the final long-term follow-up (mean 5 years) and no patient presented with relapsing symptoms. It is possible that the early stage of CRPS-I and the different doses of methylprednisolone and lidocaine in comparison with previous studies may have played a role in the better clinical results that were noted in our study.
For our patients we selected intravenous regional block using 25 ml of 0.5% lidocaine and 125 mg of methyloprednisolone. Lidocaine acts in different ways. It interrupts the abnormal sympathetic arc through somatic nerves by blocking afferent (centripetal) impulses. It blocks C sympathetic fibres, which conduct afferent impulses and dull aching somatic pain. As an anaesthetic agent it alleviates local pain when injected into the affected extremity. Methyloprednisolone reduces swelling and stiffness by acting in the cell membrane of the tissues in the affected extremity. It also alleviates pain with its analgesic effect. The doses that are used do not justify fears for aggravation of local osteopenia, worsening of pre-existing diabetes, or causing osteonecrosis in the skeleton. With the tourniquet inflated for 20 minutes the two injected agents are allowed to have prolonged action through prolonged contact with the local tissue environment and apply all their local properties. Patients tolerated the procedure without any adverse effects. Analgesics and physical therapy were important adjuvants in the treatment.
Early recognition of the syndrome and prompt initiation of treatment was the key to achieved outcome. All of our patients were in the acute phase of the syndrome and thus their symptoms – and course of the disease – were reversible. This very encouraging outcome seems to be permanent as the follow-up is long enough to permit reliable conclusions.
A weakness of the study is that there is no control group. We believe that when treating a multifactorial syndrome like CRPS-I the treating surgeon must apply all measurements that he or she believes are necessary for the desirable outcome. For this reason there is no control group. We also believe that the main factor for the successful treatment was the action of the intravenous regional anaesthesia, using lidocaine and methyloprednisolone.
Based on our results, we suggest the use of intravenous lidocaine and methyloprednisolone along with physical therapy and oral analgesics, as a treatment modality for patients in the acute phase of the complex regional pain syndrome type I.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interests
None declared.