
Abstract
We have assessed the anti-inflammatory, anti-oxidative and anti-coagulant effects of locally applied natural and recombinant hirudin in a random skin flap rat model. Thirty Wistar rats with venous congested skin flaps were randomly divided into two treatment groups and a control group to receive subcutaneous injections of natural hirudin (6 U), recombinant hirudin (6 U) or physiological saline, respectively. Superoxide dismutase, malondialdehyde and endothelin levels as well as flap survival rates of the skin flaps were measured after surgery. Compared to the control group, the treatment groups had significant higher superoxide dismutase levels and lower malondialdehyde and endothelin levels in the skin flaps. The surviving areas of the flaps were larger in the treatment groups than the control group. Our results demonstrated that hirudin could improve skin flap survival through its anti-inflammatory, anti-oxidative and anti-coagulant activities.
Keywords
Introduction
Flap necrosis caused by ischaemia, venous congestion or haematoma has long been a challenge to plastic and reconstructive surgeons. Partial to complete flap necrosis can lead to future complications, including delayed wound healing, wound dehiscence and wound contracture.
Many chemicals, such as sympatholytics, vasodilators, calcium channel blockers, prostaglandin inhibitors, glucocorticoids and free radical scavengers are known to improve flap viability (de Godoy et al., 2010; Gözü et al., 2010; Livaoğlu et al., 2009; Manchio et al., 2009; Nezami et al., 2009; 2010). However, even with these chemical treatments, flap necrosis may still occur. In addition, a majority of these reagents requires systemic application at relatively high doses, which can produce side effects (Karaçal et al., 2005).
Leech therapy is a clinically proven method to treat venous flaps; however, using live leeches may cause anaemia and transmit infectious diseases such as AIDS or viral hepatitis (Chepeha et al., 2002; Conforti et al., 2002; Soucacos et al., 1994). In recent years, natural hirudin, a peptide extracted from the leech salivary gland, has been used experimentally to treat flap venous congestion. It is generally believed that hirudin can improve the survival rate of the congested flaps through its anti-inflammatory, anti-oxidant and anti-coagulant functions. Recombinant hirudin can be prepared by expressing the cloned hirudin cDNA in bacteria or yeast and it is used for various applications in the United States, Japan, and Europe. Nonetheless, the effectiveness of recombinant hirudin treatment on flap venous congestion has not been reported.
In this study, we aimed to explore the mechanisms through which natural and recombinant hirudin improve random flap survival and to assess the anti-coagulant, anti-oxidant and anti-inflammatory functions of hirudin by measuring superoxide dismutase (SOD), malondialdehyde (MDA), and endothelin (ET) levels. In addition, we compared the effectiveness of natural and recombinant hirudin on flap survival.
Methods
Animals and reagents
The use of 30 Wistar rats (∼250 g) was approved by the Animal Experimental Center of Medical University. The animal handling protocol was in accordance with the Regulations of Laboratory Animal Care (Yin, 2004). The rats were housed singly in polycarbonate cages at 20–22°C in a humidity-controlled environment with a 12 hour day/night cycle during preoperative and postoperative periods. The rats were allowed free access to water and rat chow. Recombinant hirudin (Sigma, Aldrich, USA), natural hirudin (Xike Kang, Nanning, China), the superoxide dismutase kit, the ET kit and the MDA kit (Jiancheng, Nanjing, China) were used in this study.
Surgical procedure and flap evaluation
All rats were anaesthetized by intraperitoneal injections of xylazine (10 mg/kg) and ketamine (50 mg/kg). The hair of the dorsal skin was removed with 8% sodium sulphide and the skin was sterilized with Betadine (Xinkaiyuan, Boai, China). Caudally based dorsal flaps (10 cm × 3 cm in size) were raised under sterile conditions. The palpable hip joints were used as anatomical landmarks to define the base of the flap. The flap was dissected and detached from the panniculus carnosus and reattached in the original position with separate sutures (Figures 1 and 2). The sites of injection were 1–3 cm distal to the flaps. The time of injection was immediately after surgery and further injections were given at day 3 and day 5 after operation. The injection was carried out approximately 4 mm below skin surface, between the dermis and subcutaneous stratum (Figures 3 and 4). The rats were divided randomly into three groups (ten in each group). In group A, 6 U of natural hirudin was locally applied to each flap. In groups B, 6 U of recombinant hirudin was locally applied to each flap. In group C, isotonic NaCl was locally applied to each flap as a control group. Seven days after surgery, the rats were anaesthetized and the flattened back skin flaps were photographed with a digital camera. The necrotic and viable areas of skin flap were calculated by Image-Pro 6.0 (Media Cybernetics, Inc., MD, USA) software analysis system. The flap survival rate was calculated as the percentage of area of surviving flap in the total flap area.

The sizes of the flaps were marked out before operation.
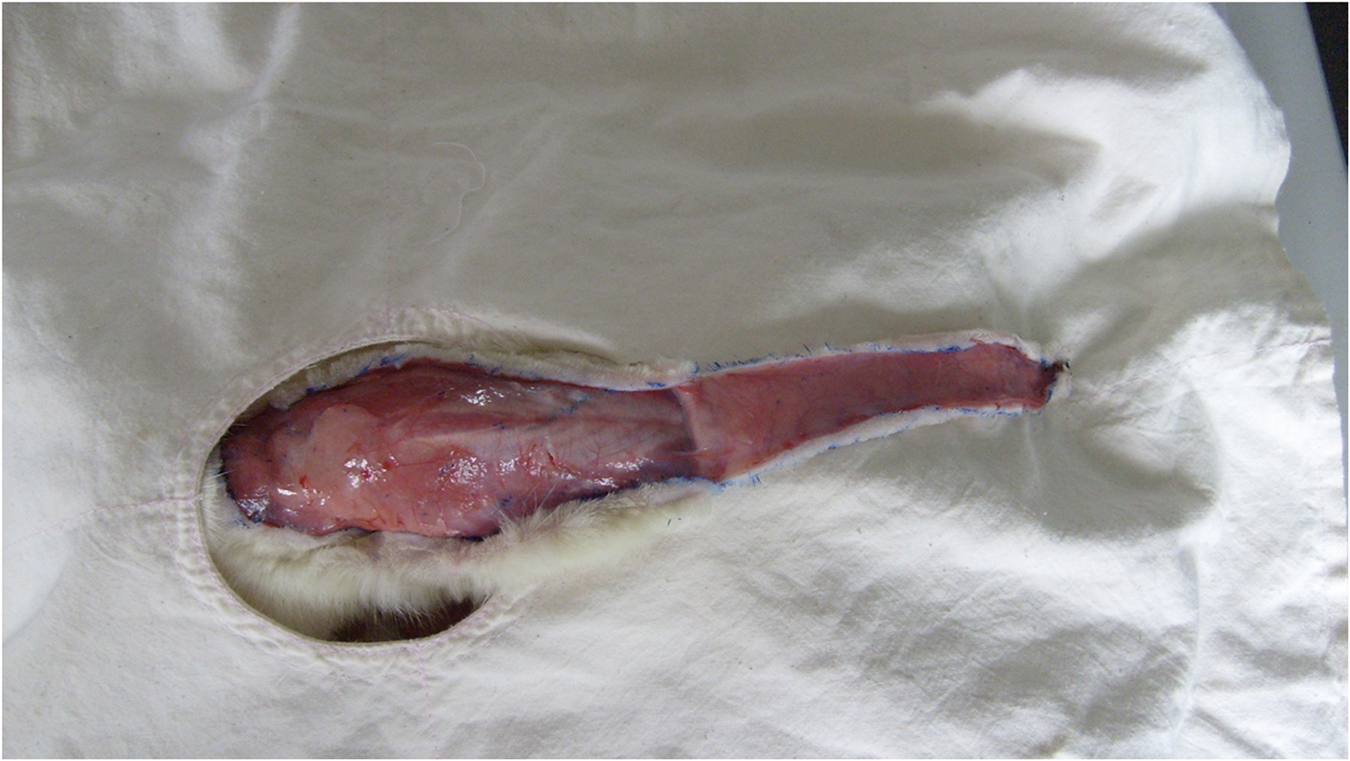
Flaps were raised at surgery.

The hirudin injection site.

Injection of hirudin after surgery.
Histopathological assessment
The samples were preserved in 10% formalin solution. Transverse sections were taken at the flap base 3 cm (viable area) or 7 cm (necrosis area) distal to the viable–necrotic area boundaries. The tissue samples were embedded in paraffin blocks; 4–6 µm thick sections were cut and stained with haematoxylin and eosin and assessed under a light microscope. The slide assessments were done in a blinded fashion using pre-established criteria and scores. Each slide was assessed and scored by a pathologist and repeated three times in 1 week intervals without particular order to ensure impartiality.
Measurements of total SOD, ET and MDA levels
SOD, ET and MDA levels were measured on day 7 after operation. A full thickness skin specimen of 1.5 cm × 1.5 cm in size was taken at 3 cm distal (viable area) to the flap base and homogenized immediately at 4°C. Total SOD, ET, and MDA levels in skin samples were measured using the protocol of the manufacturer.
Statistical analysis
The results are provided as means and standard deviations. We used analysis of variance (ANOVA) to compare changes among the groups and the Student–Newman–Keuls test to identify the differences. A p-value <0.05 was considered statically significant.
Results
Flap survival
All rats used in this study survived until the end of the study without infection. The necrotic area on the skin flaps was stabilized 7 days after surgery with clear boundaries between the surviving and necrotic areas (Figures 5 to 7). The percentages of the surviving flap area (flap survival rate) are shown in Table 1.

A skin flap in the natural hirudin group 7 days after surgery.

A skin flap in the control group 7 days after surgery.

A skin flap in the recombinant hirudin group 7 days after surgery.
Flap survival rate in each group
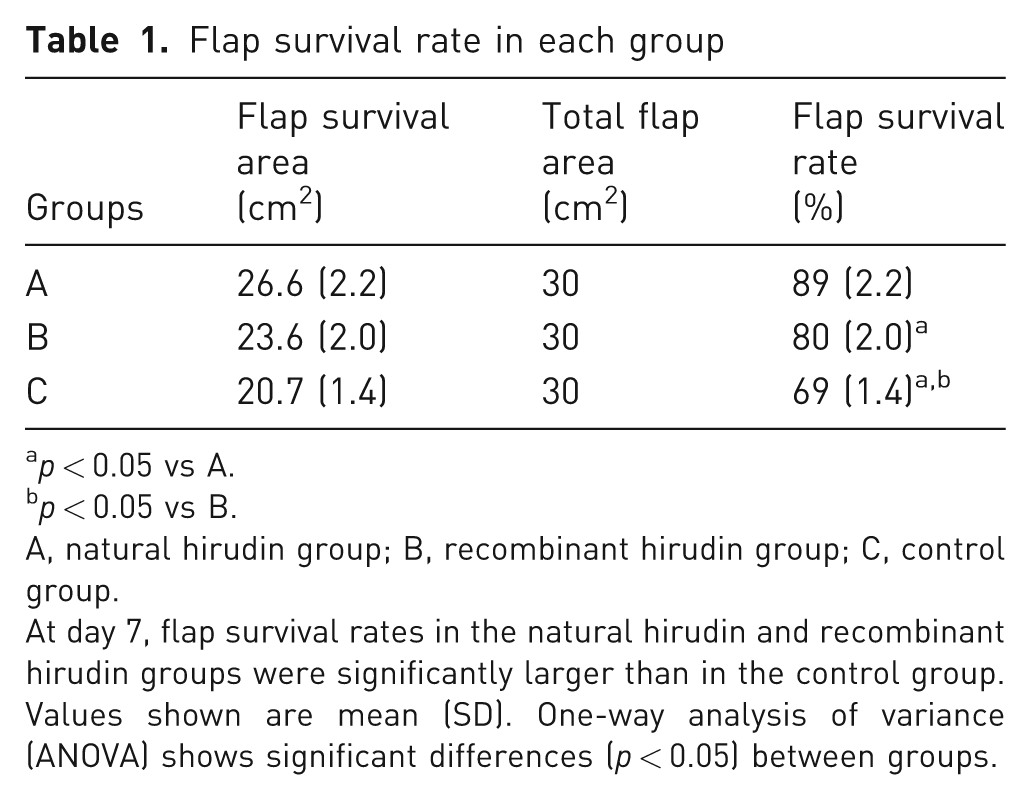
p < 0.05 vs A.
p < 0.05 vs B.
A, natural hirudin group; B, recombinant hirudin group; C, control group.
At day 7, flap survival rates in the natural hirudin and recombinant hirudin groups were significantly larger than in the control group. Values shown are mean (SD). One-way analysis of variance (ANOVA) shows significant differences (p < 0.05) between groups.
Histopathological observation of the flaps
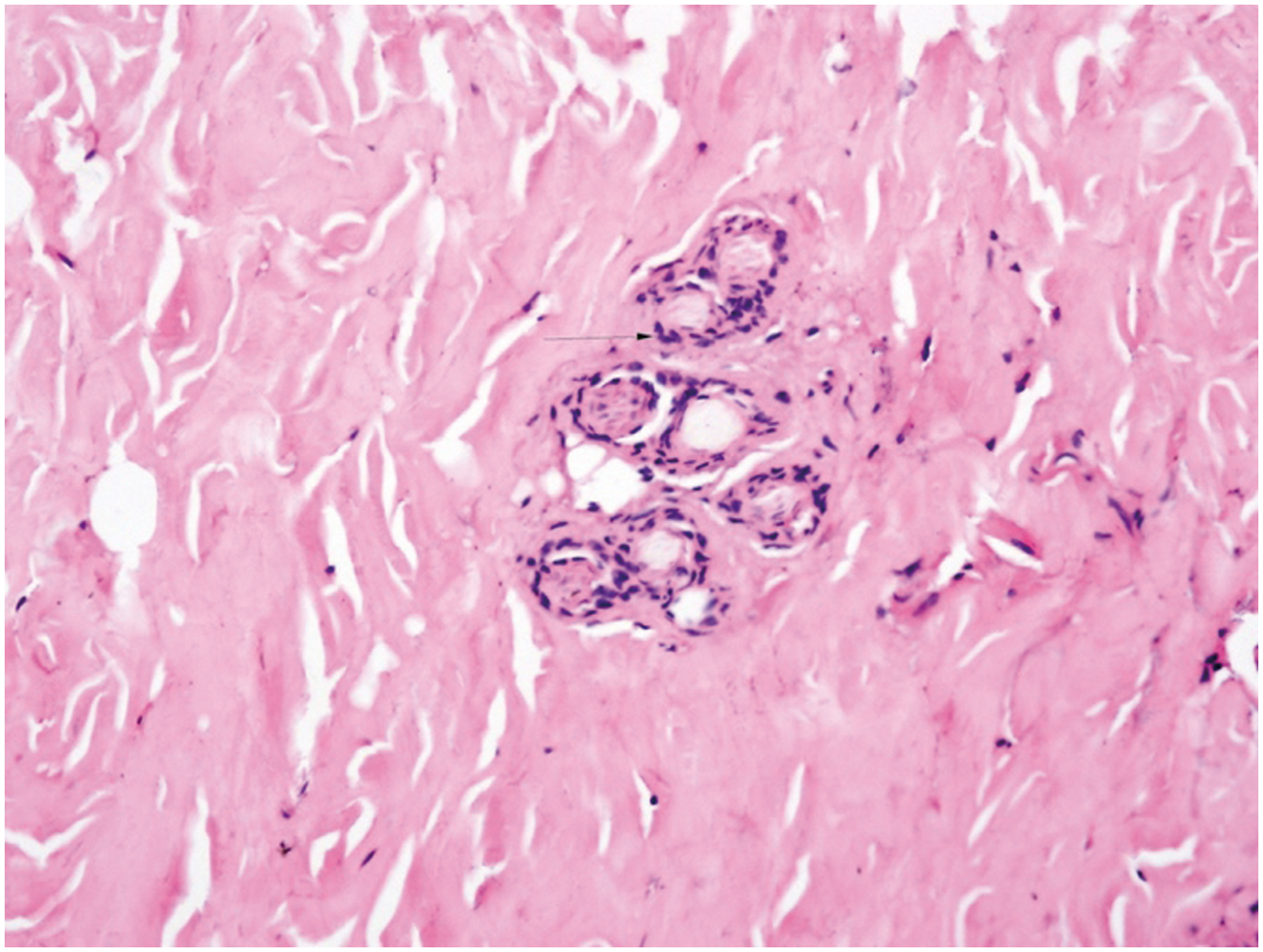
In the natural hirudin group, no atrophy was observed. Only mild hyperkeratosis and inflammatory cell infiltration were present in the flap tissue. There was an increase in subcutaneous vessel densities in the treated group (nine per flap image). In contrast, subcutaneous flap oedema and local ulceration were seen in the control group, with fewer subcutaneous vessels observed (three per flap image). The histopathological features of the recombinant hirudin group were intermediate among the three groups (Figures 8 to 10).
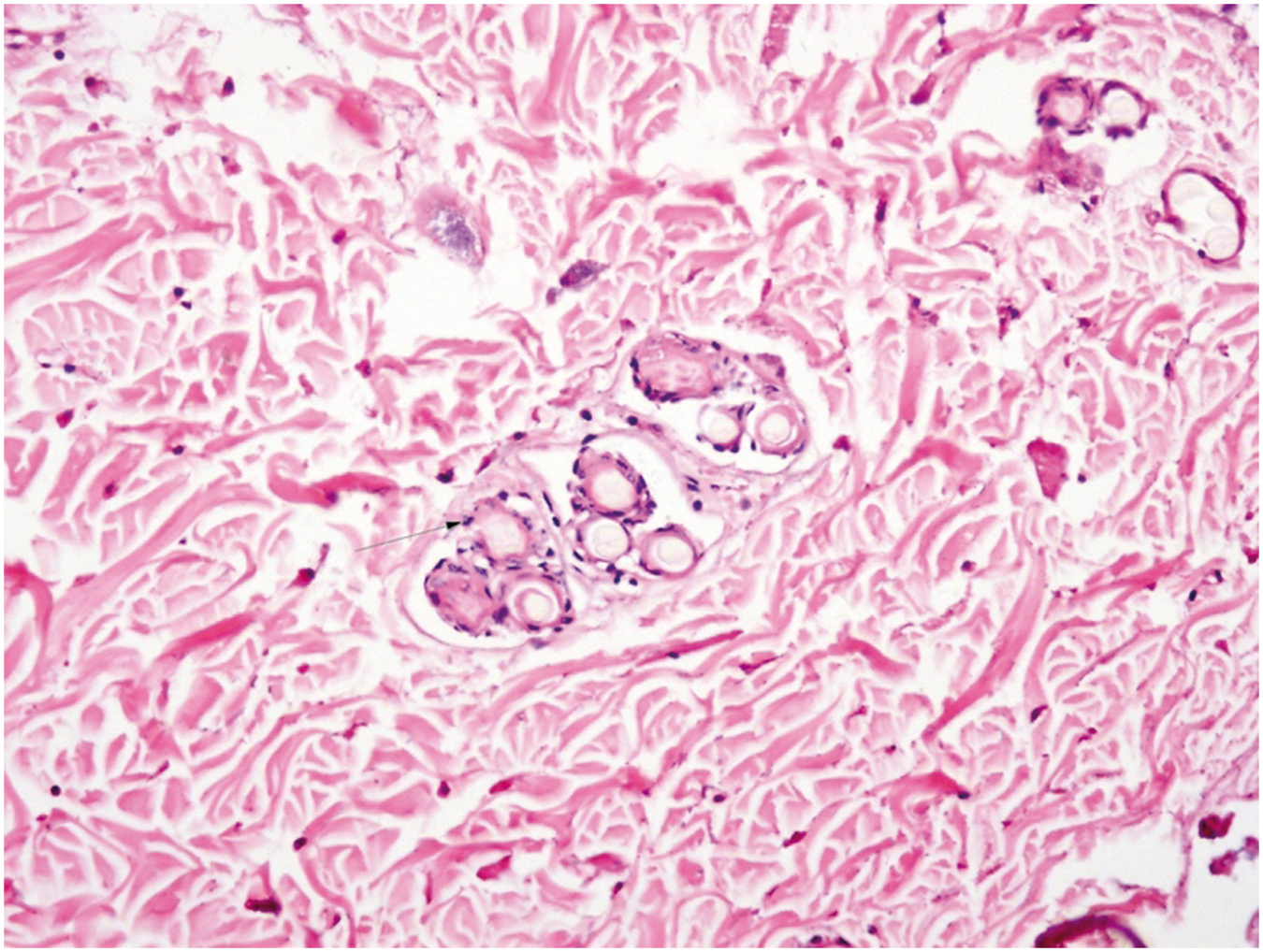
Few inflammatory cells were observed in the natural hirudin group flaps (original magnification: 400×).
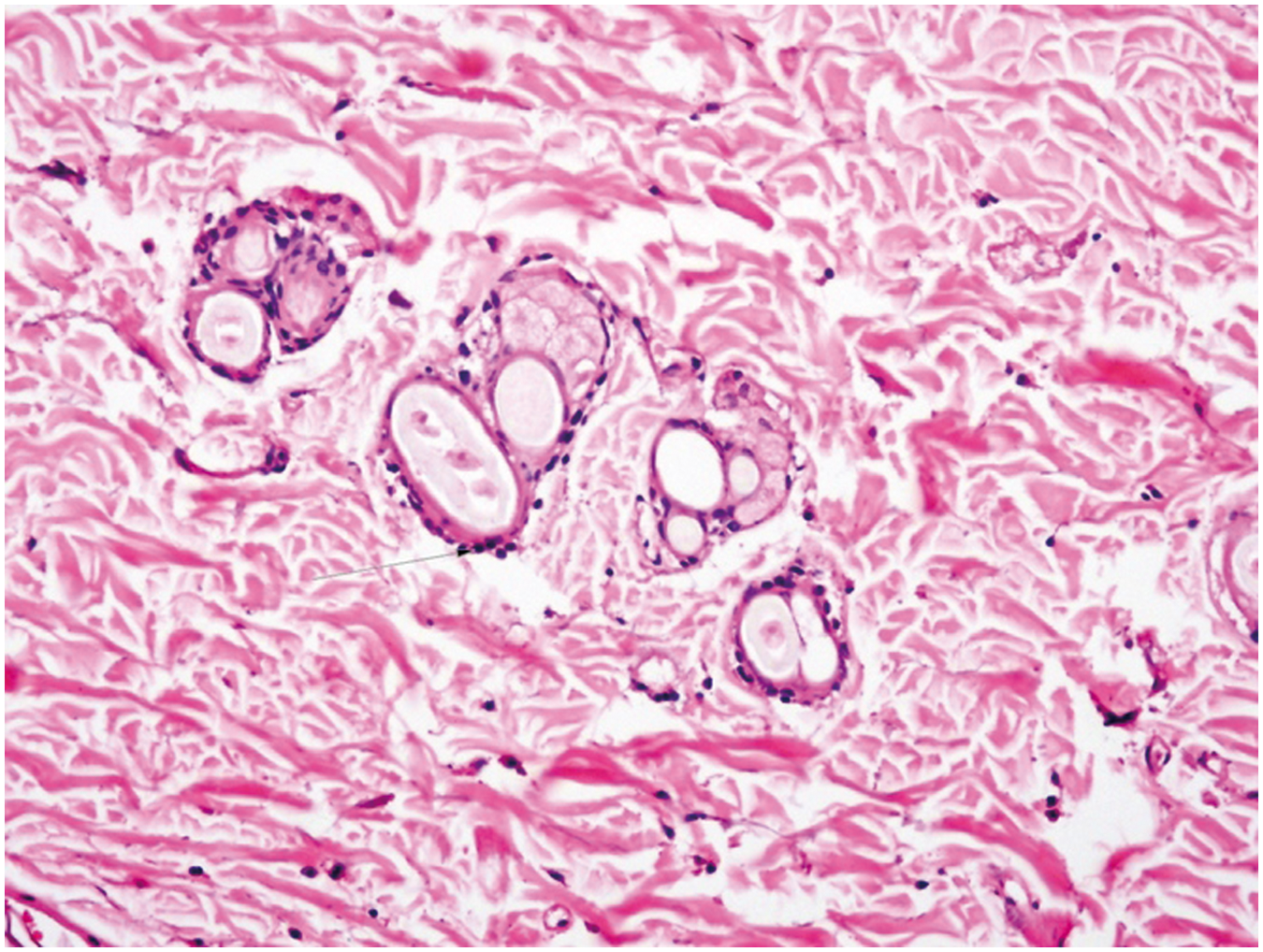
More inflammatory cells were found in the recombinant hirudin group flaps (original magnification: 400×).
A large number of inflammatory cells were found in the control group flaps (original magnification: 400×).
MDA, SOD, and ET levels in the flaps
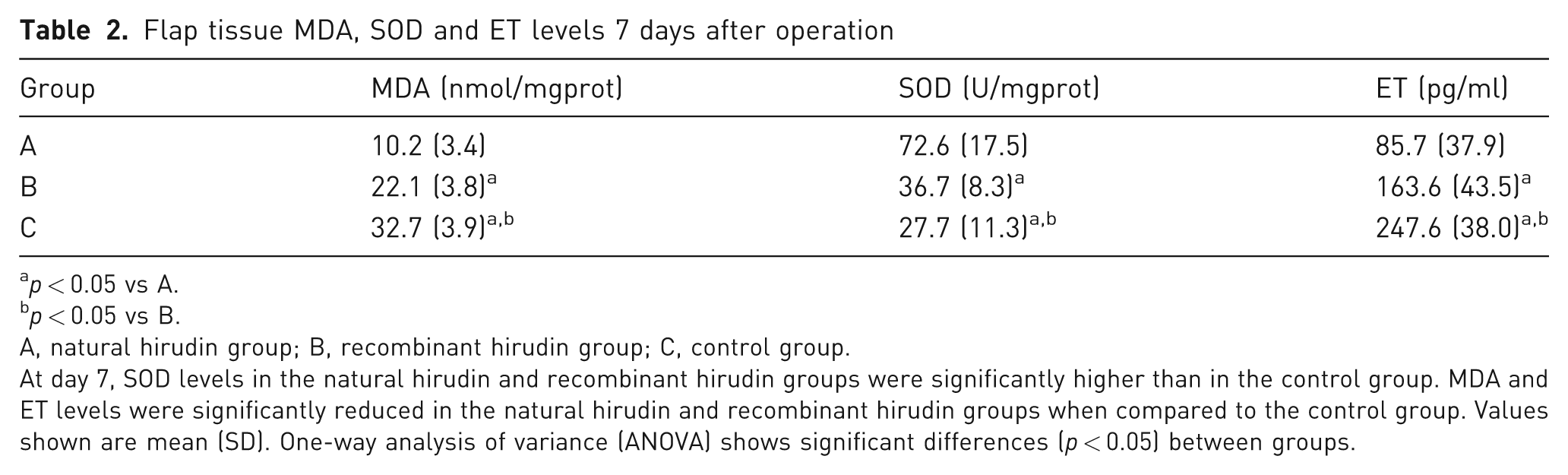
Hirudin treatment effects on MDA, SOD, ET levels in flap tissues are shown in Table 2. MDA levels in both hirudin treated groups are significantly lower than in the control group. SOD levels in the hirudin treated groups were significantly higher than that of the control group. The natural hirudin group had the highest SOD level among the three groups. Similar to MDA, the ET levels in both hirudin treated groups were significantly lower than control group. The natural hirudin group had the lowest ET level among the three groups.
Flap tissue MDA, SOD and ET levels 7 days after operation
p < 0.05 vs A.
p < 0.05 vs B.
A, natural hirudin group; B, recombinant hirudin group; C, control group.
At day 7, SOD levels in the natural hirudin and recombinant hirudin groups were significantly higher than in the control group. MDA and ET levels were significantly reduced in the natural hirudin and recombinant hirudin groups when compared to the control group. Values shown are mean (SD). One-way analysis of variance (ANOVA) shows significant differences (p < 0.05) between groups.
Discussion
Maintaining flap survival is considered as one of the most important goals for random skin flap surgery. In order to achieve this goal, many physical and chemical treatments have been studied (Emsen, 2007; Hart et al., 2006; Holzbach et al., 2010; Ozler et al., 2010; Russo et al., 2006).
Skin flap viability can be influenced by internal and external factors (Brown et al., 2003). Adhesion of inflammatory cells at the damaged flap edge, activation of the coagulation system, vascular thrombosis, and venous congestion are the main causes of skin flap necrosis (Atchabahian and Masquelet, 1996; Kroll et al., 1996; Vedder et al., 1994a; 1994b; Yajima et al., 1993). Venous congestion of the flap causes an increase in free radicals, which leads to the loss of membrane integrity (Harashina et al., 1977; Yan et al., 2010).
As a product of lipid peroxidation, MDA is closely related to free radical metabolism. The MDA level is a critical indicator of tissue damage (Eskitascioglu et al., 2009; Gideroglu et al., 2009). Our results showed that the MDA levels in both hirudin treated groups are significantly lower than that of the control group. The natural hirudin group had the lowest MDA level among the three groups. A higher percentage of flap survival correlated with lower MDA level in the treated groups, suggesting that hirudin can improve flap survival by reducing MDA level in the congested flap.
SOD plays an important role on the oxidation balance (Kanth et al., 2010). Although the MDA level is an indicator of free radicals, the level of SOD indirectly reflects the body’s ability to eliminate free radicals (Gulubova and Vlaykova, 2010; Shuvaev et al., 2010). SOD levels in the hirudin treated groups were significantly higher than in the control group. The natural hirudin group had the highest SOD level among the three groups. The percentage area of surviving flap correlated with high SOD levels in the treated groups, suggesting that hirudin can improve flap survival by increasing the level of SOD in the flap.
ET is a strong vasoconstrictor that plays a key role in vascular homeostasis. Kara et al. (2001) reported that an increased ET level in the skin flap is able to induce small artery contraction and spasm. Contraction in the microcirculation system may result in flap necrosis (Tane et al., 1995). Similar to MDA, the ET levels in both hirudin treated groups were significantly lower than in the control group. The natural hirudin group had the lowest ET level among the three groups. A higher percentage area of surviving flap correlated with lower ET levels in the treated groups, suggesting that hirudin can improve flap survival by reducing ET level in the congested flap.
In summary, our study demonstrated that natural and recombinant hirudin treatments led to increases in SOD level and decreases in MDA and ET levels, which may potentially contribute to the hirudin-mediated effects of improving skin flap survival, via various molecular mechanisms such as anti-inflammatory, anti-thrombotic and anti-coagulatory pathways (Alibeik et al., 2010). Our study also showed that natural hirudin is more potent in preventing flap necrosis than recombinant hirudin, probably due to the chemical difference and the purity of the reagents.
Footnotes
Acknowledgements
The authors gratefully acknowledge the help of my supervisor, Professor Zhou Yanayn. I also owe a special debt of gratitude to all the professors in laboratory.
Funding
This study was supported by Foundation item Natural Science of Guangxi Zhuang Autonomous Region (2010GXNSFA013141).
Conflict of interests
None declared.