
Abstract

Dear Sir,
Chronic hyperextension of the thumb most commonly occurs at the metacarpophalangeal joint (MCPJ). It is associated with degenerative, inflammatory and congenital conditions, as well as being a sequela of hyperextension injury (Tonkin et al., 1995). A number of procedures have been described to correct this with satisfactory results. Of these, sesamoid arthrodesis can be successful, durable and advantageous over MCPJ fusion, as a functional range of flexion is maintained (Tonkin et al., 1995; Gwilym et al., 2005).
Chronic hyperextension instability of the thumb interphalangeal joint (IPJ) is less frequently described but can be functionally disabling (Figure 1). There are few surgical options specifically for the thumb IPJ. Those available usually describe the repair of the volar plate in acute injuries (Engber, 2000). We performed a sesamoid arthrodesis to correct symptomatic chronic hyperextension instability of the thumb IPJ in two patients with an intact volar plate.
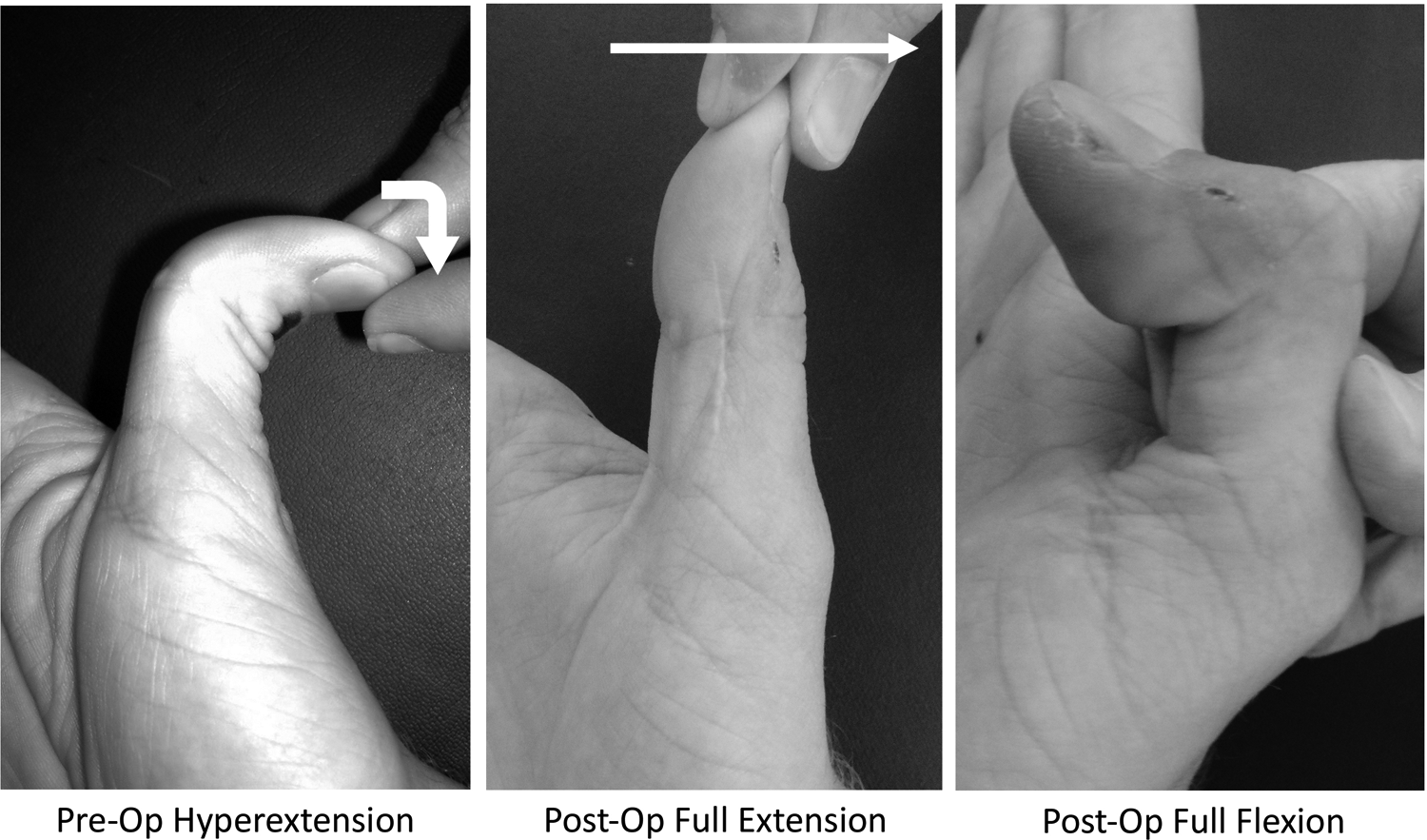
Demonstration of preoperative hyperextension, postoperative full extension and flexion (Case 2).
A 16-year-old male reptile handler presented with symptomatic chronic 45° hyperextension of his dominant thumb IPJ (Case 1) without a history of injury. The other patient was an 18-year-old male professional golfer (Case 2) who presented with symptomatic chronic 90° hyperextension of his dominant thumb IPJ (Figure 2). There was a history of minor trauma several months previously, but magnetic resonance imaging demonstrated no soft tissue injury and revealed an intact volar plate. Initial treatment with extension-blocking splints failed to give lasting benefit, so we recommended surgical stabilization.
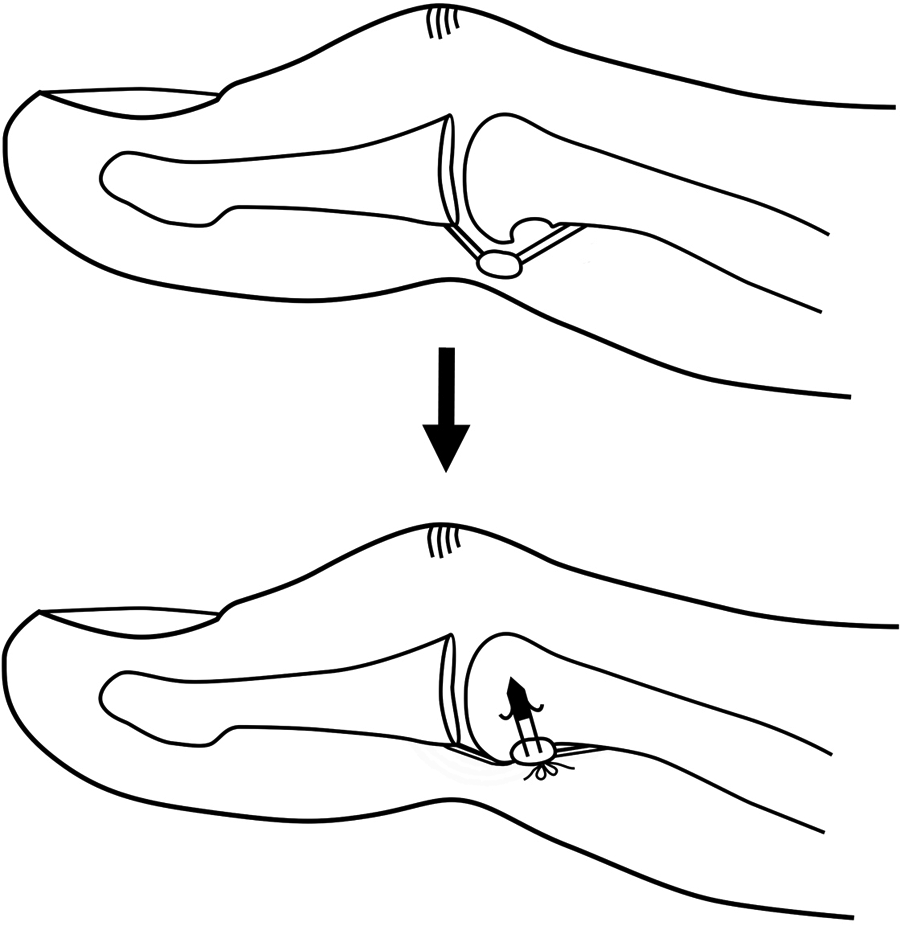
Cortical area created over the neck of the proximal phalanx, sesamoid bone secured with a suture anchor.
A sesamoid bone at the thumb IPJ is essential for this technique and must be seen on plain radiographs. Cadaver and radiological studies suggest a variable rate of patients having a thumb IPJ sesamoid, with most being bilateral (Joseph, 1951). The sesamoid is embedded within the middle of the joint capsule and is distinct from the tendon of flexor pollicis longus that overlies it (Engber, 2000).
The surgical technique was similar to the sesamoid arthrodesis of the thumb MCPJ (Tonkin et al, 1995). A radial mid-lateral incision was made, elevating and protecting the neurovascular bundle. The accessory collateral ligament was elevated and the IPJ capsule incised. The sesamoid was identified and its articular surface decorticated using a burr. The corresponding area of the proximal phalanx neck was similarly decorticated (Figure 2) and a mini anchor (DePuy Mitek©, MA, USA) inserted through this defect in the neck of the proximal phalanx. The sesamoid bone was then sutured, stabilizing the palmar aspect of the joint (Figure 2). Alternative methods to secure the sesamoid in place, such as screw fixation, may be considered. The joint capsule and skin were closed in layers. A bulky dressing and thumb spica forearm splint immobilized the joint for 2 weeks. A thermoplastic extension-blocking splint was applied for a further 4 weeks, after which active flexion and extension exercises were started.
No postoperative complications were encountered. At follow-up (Case 1: 41 months and Case 2: 27 months) hyperextension had been abolished (Figure 1) and a functional range of flexion had been preserved (Case 1: 0-0-90°, Case2: 0-0-80°). Both returned to their previous level of activity. Potential sources of failure include stretching of the volar plate or pulling out of the suture anchor, though neither have occurred.
Footnotes
Conflict of interests
None declared.
Patient consent obtained.