
Abstract
Thirty-eight fingers in 27 patients with Dupuytren’s contracture of the proximal interphalangeal joint (PIPJ) in excess of 70° were treated using a staged technique. The first stage involved applying a mini external fixator across the PIPJ for continuous extension over 6 weeks with intensive hand therapy to maintain mobility of the joint and help correct the deformity. Twice weekly during hand therapy sessions the tension of the elastic band across the mini ex-fix was increased, allowing that full active flexion of the PIPJ against the elastic band could still be achieved. The second stage, 4 weeks after the external fixator was applied, involved an open palm technique of fasciectomy for the contracted cords restricting metacarpophalangeal joint movement and dermofasciectomy with full-thickness skin grafting over the proximal phalanx for bands restricting PIPJ movement. The external fixator was used to maintain active extension force until the graft healed. It was generally removed in the outpatient clinic under ring block 2 weeks after the second stage procedure. The patients were followed for a mean of 20.6 (6–48) months. The mean preoperative PIPJ deformity improved from 75° to 37° postoperatively. Overall, 69% of results were rated as good to excellent. Only one patient reported any on-going functional problems. There were eight cases of pin site infections and one case each of loose pins, osteoarthritics at the PIPJ, reflex sympathetic dystrophy, and disease recurrence needing PIPJ fusion. We conclude that our simple staged procedure is a valid alternative in the management of severe Dupuytren’s PIPJ contracture.
Introduction
In 1831, Baron Dupuytren demonstrated a surgical case of his eponymously named disease in Paris (Elliot, 1999). By 1900, eight books and hundreds of articles had been published on the subject of Dupuytren’s disease.
Despite much being known about the disease, difficulty and consternation still remain regarding the treatment of the severest manifestations, whether primary or recurrent. Indeed, in severe digital deformities (defined here as either a flexion contracture of the proximal interphalangeal joint [PIPJ] exceeding 70° or recurrent PIPJ contracture that the surgeon predicts will be difficult to correct), for example, salvage procedures may have to be considered. These include dorsal wedge osteotomy of the proximal phalanx, arthrodesis of the PIPJ, or replacement arthroplasty (Moberg, 1973). Rarely, amputation may have to be considered for the severe or recurrent PIPJ contracture.
The major problem in severe cases is the difficulty of achieving active extension at the PIPJ, which may be held by several cords, contracted check-rein ligaments, and/or scar contracture (McGrouther, 2005). Acute single stage correction of severe contractures may be compromised by the stretching of the neurovascular structures. Skeletal traction has been employed pre- and postoperatively using an external fixation device to improve correction of the PIPJ (Beard and Trail, 1996; Hodgkinson, 1994; Messina and Messina, 1993; Rajesh et al., 2000). In such cases, it has been demonstrated that as well as decreasing deformity, facilitating surgery, and foregoing the need for amputation, the traction also alters the metabolism of the fascia, which results in remodelling and consequent lengthening (Bailey et al., 1994; Brandes, 1994). Concerns about sudden stretching of the neurovascular bundles are alleviated.
The aim of this study was to assess the viability of a simple application of a finger external fixator to achieve progressive correction of contracture at the PIPJ prior to definitive surgery and as an alternative to surgical joint release. Weinzweig demonstrated that direct PIPJ release conveyed no benefit over simple fasciectomy (Weinzweig et al., 1996).
The fixator allowed the treated digit to move throughout the possible range of PIP motion while applying a continuous extension force. Because of its size and position on the dorsum of the digit (Figure 1), it can be employed on any digit. The mode of action of the device is fundamentally an exaggeration of the force normally applied by the central slip of the extensor tendon across the PIPJ.

Insertion of the external fixator across the PIP joint.
Methods
Thirty-eight fingers in 27 patients (three females) with severe Dupuytren’s PIPJ contractures (>70° with metacarpophalangeal joint [MCPJ] fully flexed) were operated on between December 1999 and October 2004 at two different centres (Royal Free and Oldchurch Hospitals, London, UK). Mean patient age was 60.7 (range 29–79) years, and all fingers were grade III/IV according to Tubiana’s classification (Tubiana, 1986). Five of the cases had multiple fingers that underwent the two-stage procedure. Three of the cases had had previous surgery on the affected finger(s).
The first stage involved applying a mini external fixator under local anaesthesia and intra-operative image guidance (Figure 2). Two 1.6 mm diameter pins were placed in line in the midline of the dorsum of the proximal phalanx. The two distal pins were placed in the triangular bare area of the middle phalanx; the first of these approximately 2 mm from the articular surface. Elastic bands were used to adjust the tension across the joint (Figure 3). In the first three patients, tension was set to the maximum comfortable tension as determined by the patient. This was found not to allow active motion, and correction of the deformity occurred rapidly, within 2 weeks. After these three patients, an adjustment to the protocol was made. In the remaining patients, tension was set to the maximum level at which active flexion of the joint remained possible. Twice weekly, the tension of the elastic bands was adjusted such that full active flexion of the PIPJ against the elastic bands could still be achieved. This allowed for continuous correction over 3–6 weeks, as well as intensive hand therapy, including hourly exercises to maintain joint mobility, ensuring that the technique did not lead to any loss of active flexion. In addition, it was hoped that by maintaining active mobility at the joint, there would be less risk of disturbing the normal nutrition of the articulation.
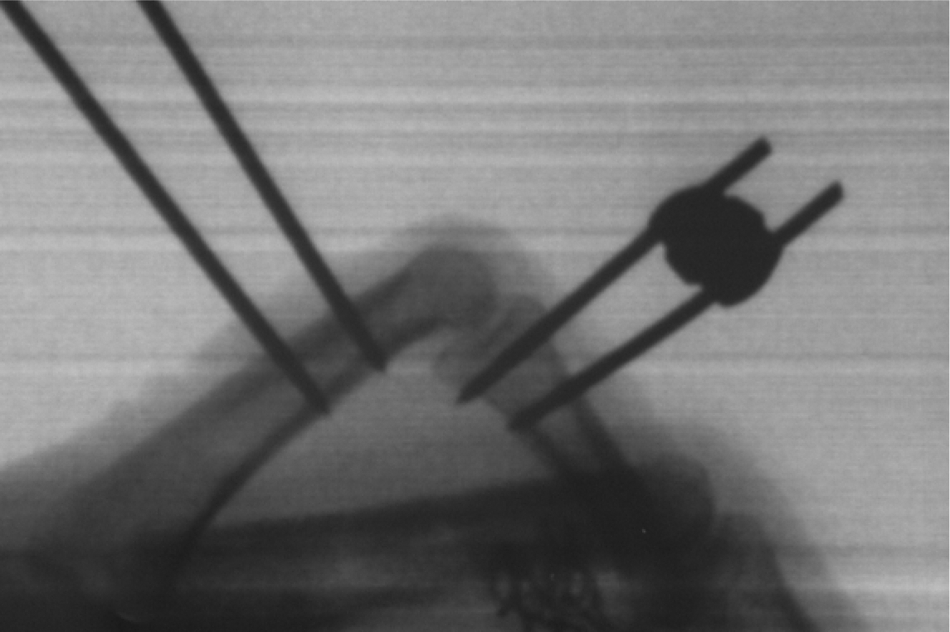
Pin insertion under fluoroscopy guidance.

Tensioning of the external fixator.
Pin sites were also reviewed and cleaned twice weekly, as it was appreciated that active use of the hands with external fixators in situ may be associated with superficial infections. When any sign of inflammation at the pin sites were found, swabs were taken for culture, and oral antibiotics were given and later adjusted for sensitivities.
The second stage, 4 weeks after the external fixator was applied, involved an open-palm technique of fasciectomy for the contracted bands restricting MCPJ movement and dermofasciectomy, with full-thickness skin grafting over the proximal phalanx for cords restricting PIPJ movement. No attempt was made to improve any residual contracture present at the time of surgery, as virtually full correction was achieved prior to operation in most cases.
The external fixator was kept in situ throughout and used to maintain correction until the graft had taken. In a few patients who had residual contracture, a minor improvement occurred during this postoperative splinting period. The fixator was removed in the outpatient clinic under local anaesthetic block 2 weeks after the second stage procedure.
Hand therapists reviewed the patient twice weekly for the first 4 weeks postoperatively, once weekly for the following 2 weeks, and then at 2, 3, 4, 5, and 6 months postoperatively. Patients were reviewed in the clinic at 2 and 6 weeks, and 3 and 6 months, postoperatively, and then annually.
At clinic review the hand therapists used a goniometer to measure active and passive movements at all joints, as well as residual or recurrent deformity. Functional outcome and complications were recorded.
Results
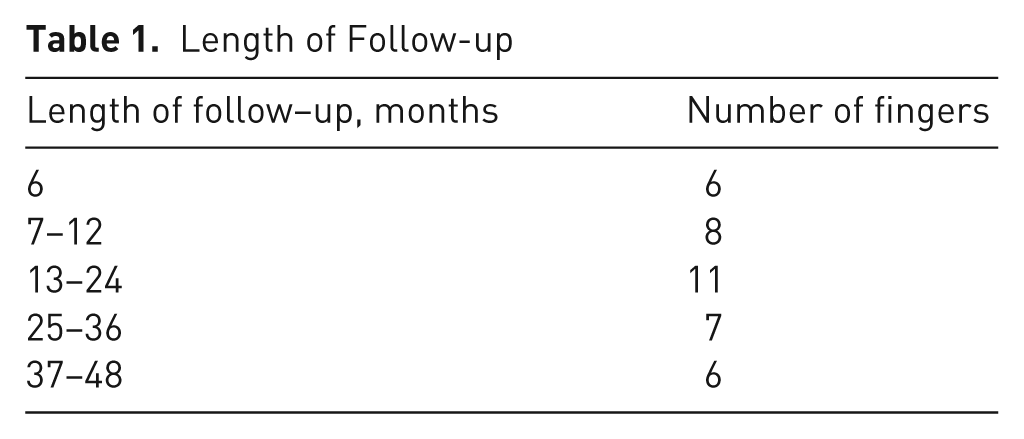
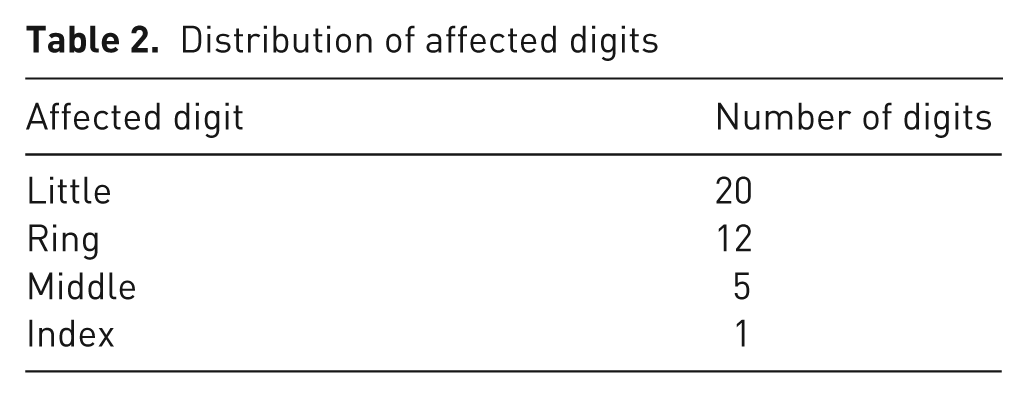
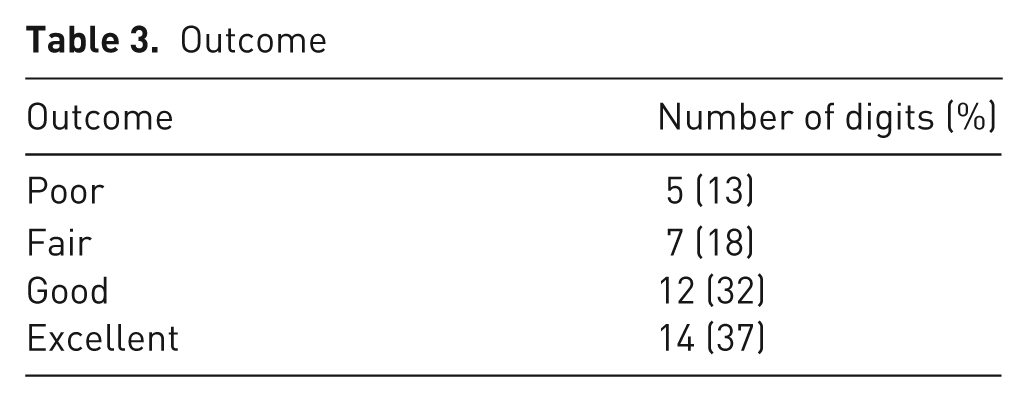
The mean length of patient follow-up was 20.6 months (Table 1). The most commonly affected digit was the little finger (53% of all affected digits) followed by the ring finger (32%) (Table 2). The mean preoperative PIPJ deformity improved from 75° to 37°, postoperatively. Based on Tubiana’s evaluation of Dupuytren’s contractures (Tubiana, 1986) and that the optimal angle for PIPJ fusion is 40°, we devised a scale to assess our results. The flexion deformity at final follow-up was categorized as an excellent outcome if < 20°, good if 21–40°, fair if 41–60°, and poor if > 60° (Table 3). Despite achieving virtually full PIPJ correction (as evidenced by an ability to place the hand and digit flat on the table) in this selected series of severe contractures, around 30% developed a significant relapse.
Length of Follow-up
Distribution of affected digits
Outcome
We asked all patients to answer the following to assess their functional outcome: Do you have any difficulty with the following: 1) putting your hand through your sleeve, 2) putting your hand in your pocket, 3) washing your face, 4) turning a round door handle, and 5) handling money. Only one patient was having any difficulty with any of these issues.
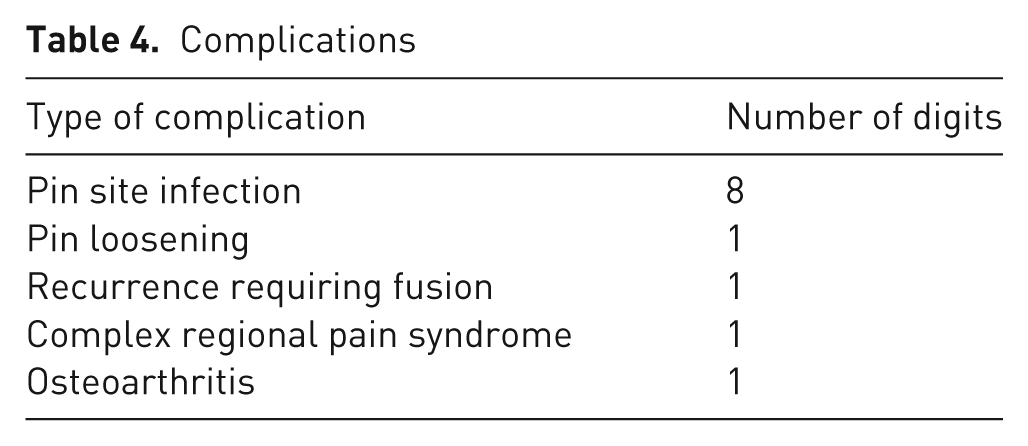
The overall rate of complications was 32% (Table 4); however, the major group (66% of complications) was of pin-site infections that resolved with antibiotic therapy, and no further intervention was required. No on-going infections occurred.
Complications
Discussion
Addressing the PIPJ deformity with surgical correction has been shown to significantly contribute to the improvement in hand function postoperatively, more so than the MCPJ (Draviaraj and Chakrabarti, 2004).
This study was intended to determine whether the application of an external fixator that allowed active joint motion was a viable method of correcting severe PIPJ deformities. Many of these cases would have been considered for amputation; this technique was initially developed as a preferable alternative. The encouraging results from this pilot study have led us to advise this method as a definitive option in such severe cases. From the results, it can be observed that 69% of patients had an excellent or good correction of PIPJ contracture and there was a mean PIPJ deformity correction of 37°.
In Citron and Messina’s (1998) series, 9 of 13 cases developed complex regional pain syndrome (CRPS), which was attributed to the speed of the correction of their deformity. Concern has also arisen regarding the increased risk of development of CRPS when the fixator is applied following fasciectomy (Beard and Trail, 1996; Citron and Messina, 1998), the feeling being that this provides too great a stress on the hand with resultant stiffness. This pilot study only gave rise to one case of CRPS, which may be because the fixation permits joint motion rather than continuous distraction, and is applied as the first of the two stages. The one case in which degenerative change in the PIPJ was observed was one of the first three patients in whom the maximum tolerable tension had been set, rather than set to maintain active motion.
It is reported that recurrence rates can be as high as 60% following surgery, but dermofasciectomy combined with skin grafting has been demonstrated to be well suited for severe primary and recurrent disease, with lower recurrence rates (Ketchum and Hixson, 1987).
There is also a theoretical concern that joints that undergo treatment with an external fixator where compression rather than distraction is combined with extension force may be prone to developing early osteoarthritis. One patient applied maximum tolerable force and achieved correction in 1 week. He was subsequently noted to have radiological changes of joint narrowing. The joint has, however, retained its range of motion and is asymptomatic at 12 years. In light of this experience, we restrict the elastic extension force to a point where the patient is able to maintain active flexion against the bands.
Although an unvalidated outcome measure was used to assess postoperative function, the majority of patients were pleased with their outcome, and only one patient had difficulty performing the daily tasks in question.
This pilot study demonstrates that this two stage procedure for severe or recurrent Dupuytren’s contracture can be performed safely, with reliable, reproducible correction of the deformity. It can be performed on any digit, because of its size and position, and is acceptable to patients. Any mini external fixator that uses 1.6 mm pins and allows two pins to be connected by a clamp can be used. This technique may be an adjunct for the hand surgeon to improve results, simplify, reduce risks in definitive surgery, and minimize the need for salvage procedures or amputation in severe or recurrent cases.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interests
None declared.