
Abstract

Dear Sir,
In December 2005 a 37-year-old woman with rheumatoid arthritis underwent a Universal 2 total wrist implant (Integra LifeSciences, Plainsboro, NJ) for increasing stiffness and significant pain in the right wrist, which had been developing over three years. No perioperative complications were associated with the operation. One year later she was extremely satisfied with the result and was able to carry out her normal activities of daily living. The pain at this time had completely resolved and she denied any instability.
For six years she had no problems. Her disability arm, shoulder, hand (DASH) score was 2.5 throughout the first six years. She presented to our clinic in August 2011 complaining of several months of progressive numbness and tingling in the median nerve distribution associated with pain in the right wrist. On examination she had a positive Tinel’s sign, positive Phalen’s sign and positive median nerve compression test. Radiographs demonstrated slight lucency around the radial and middle screws, and some lucency around the carpal component of the arthoplasty. However, the implant appeared stable. Nerve conduction studies showed a mild median nerve neuropathy of the right wrist.
A right endoscopic carpal tunnel release was planned. At operation, a standard 1.5 cm incision was made distal to the thenar/hypothenar musculature in preparation for an endoscopic release. Dissection was carried down through the palmar fascia and a dark soft tissue mass was noted in the carpal tunnel itself. The decision was made to convert to an open carpal tunnel release, and the skin incision was extended proximally past the wrist crease. The antebrachial fascia was released in its entirety, and dark soft tissue debris was noted within the carpal tunnel invading and interdigitating between the flexor digitorus profundus (FDP) and flexor digitorum (FDS) tendons to the ring and small fingers, as well as dark synovium at the base of the carpal tunnel (Figure 1). Tenolysis was done. No clear defects were visualized in the floor of the carpal tunnel. The wound was thoroughly irrigated and closed in the usual fashion.

Intra-operative image of the dark soft tissue mass, interdigitating between flexor tendons.
Histopathology of the excised synovium was reported to show ‘exuberant foreign body giant cell reaction to polarizable foreign material with proliferative synovitis consistent with implant-related arthropathy’ (Figure 2). One month after operation the patient had moderate scar sensitivity, but stated that the numbness and tingling in the digits had completely gone.
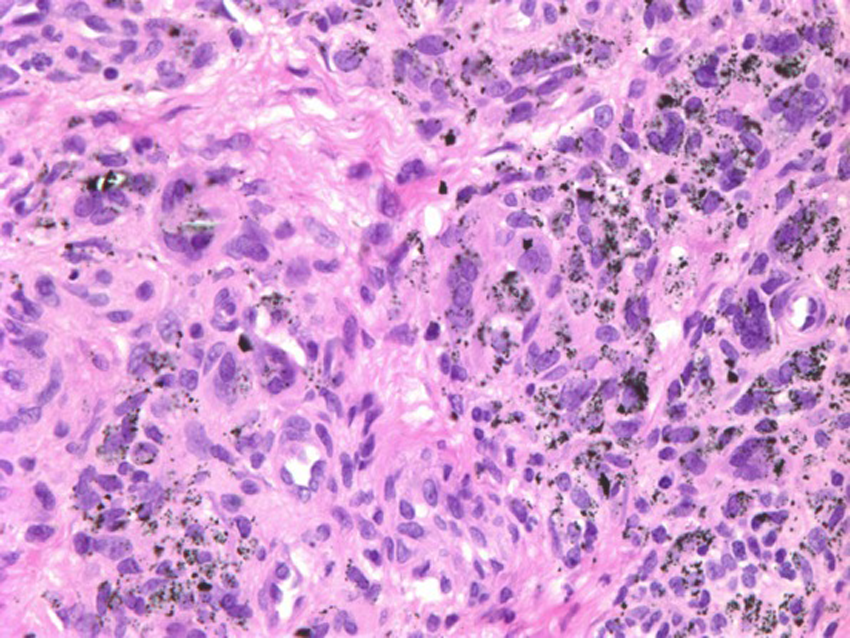
A section from the intra-operative specimen showing the exuberant foreign body giant cell reaction (Courtesy Dr G. Frieling, Beth Israel Deaconess Medical Center Department of Pathology).
Metallosis is a well-known complication of total joint replacement. However, it has primarily been found in weight-bearing joints, such as the hip and knee (Weissman et al., 1991). The incidence of metallosis in non-weight-bearing joints, such as the wrist and elbow, is far less documented (Hopkins et al., 2007; Sayed-Noor and Sjödén, 2010). It has been seen in patients who have undergone total wrist revision arthroplasty or arthrodesis, secondary to instability or loosening of arthroplasties. We have not found a previous report of metallosis causing signs of carpal tunnel syndrome. There has been one previous case report of a patient presenting with symptoms similar to carpal tunnel syndrome following total wrist arthroplasty, but this was a result of silicone synovitis (Siemon et al., 2004). In the case we report it was evident that metallosis within the carpal tunnel was causing a secondary carpal tunnel syndrome. It is difficult to establish where the metallosis originated, but we presume it was from the interface between the screws and carpal component, as well as from some wear in the carpal component. Without operative visualization it would have been difficult to establish that metallosis was the cause of the carpal tunnel symptoms. Pre-operatively we did not consider this condition as a cause for carpal tunnel syndrome in this patient, but it should be borne in mind when symptoms of carpal tunnel syndrome occur after a total wrist arthroplasty.
Footnotes
Conflict of interests
None declared.