
Abstract
The aim of this study was to test the precision and reliability of measurements of the bone mineral density (BMD) of the trapezium in patients with osteoarthritic trapeziometacarpal joints using dual-energy X-ray absorptiometry scans and to assess whether there is an acceptable correlation between the BMD of the trapezium and that of the distal radius, for which normative data exist. We included 66 patients (52 women, 14 men) diagnosed with Eaton–Glickel stage II–IV osteoarthritis and a mean age of 59 years (range 40–77) in a prospective study. We found good intra- and inter-observer agreement of BMD measurements. Reliability was also good in repeated measurements. There was an indication of an increase in BMD with progression in the Eaton–Glickel stage. There was only a moderate correlation between the BMD of the trapezium and that of the radius.
Introduction
Aseptic loosening of the trapezium component in total joint replacement of the trapeziometacarpal (TM) joint is a major problem (Hansen and Snerum, 2008; Hansen and Vainorius, 2008; Hernández-Cortés et al., 2012; Johnston et al., 2012; Kaszap et al., 2012; Klahn et al., 2012; Perez-Ubeda et al., 2003; Wachtl et al., 1998). Many factors may contribute to aseptic loosening such as implant design and insertion technique (Hansen et al., 2011), but poor bone quality of the trapezium may be a major factor, especially in cementless implants.
Unfortunately, the relationship between hand osteoarthritis and osteoporosis is not clear. In a small case-control study in postmenopausal women, Zoli et al. (2006) found that women with clinical osteoarthritis of the hand had a significantly higher percentage of osteoporosis of the lumbar spine than controls without clinical hand osteoarthritis. Kim et al. (2010) examined 180 postmenopausal women and found that women with radiographic osteoarthritis of the hand had lower forearm bone mineral density (BMD) than women without radiographic osteoarthritis of the hand. In contrast, Haugen et al. (2007) found that patients with radiographic osteoarthritis of the hand had increased BMD in the hip and lumbar spine compared with controls without radiographic osteoarthritis of the hand. In a large population study, Schneider et al. (2002) found that clinical osteoarthritis of the hand was not associated with low or high total body BMD.
Researchers have tried to estimate the bone quality in osteoarthritic hands in only a few studies. Haara et al. (2005) found a relation between radiographic osteoarthritis of the distal interphalangeal joint and/or osteoarthritis of the TM joint and radiographic signs of osteoporosis with reduced metacarpal cortical thickness. El-Sherif et al. (2007) looked at the relation between radiographic osteoarthritis of the hand in postmenopausal women and BMD in the middle finger, and found reduced BMD in patients with osteoarthritis of the hand. As there are no data for normative BMD in the hand, measurement of BMD in the distal radius could be used instead of hand BMD measurements if there is a good correlation between BMD in the hand and distal radius. Brownbill and Ilich (2002) found a good correlation between BMD in the hand and BMD in the forearm, hip, spine, and total body in postmenopausal women; the best correlation was between the hand and forearm (Pearson’s r = 0.82).
Predicting poor bone quality of the trapezium before surgery might guide the choice of implant fixation method and potentially reduce the failure of TM total joint implants. The aim of this study was to test the precision and reliability of measurements of the BMD of the trapezium in patients with osteoarthritic TM joints using dual-energy X-ray absorptiometry (DEXA) scans, and to assess whether there is an acceptable correlation between the BMD of the trapezium and distal radius (where normative data exist) indicating if BMD measurement of the distal radius may be used as a clinical screening measure for the bone quality of the trapezium.
Methods
We included 66 patients (52 women, 14 men) with 80 hands diagnosed with Eaton–Glickel stage II–IV osteoarthritis of the TM joint in a prospective study. All radiographs were classified according to the Eaton–Glickel classification (Eaton and Glickel, 1987) by one observer to avoid interobserver variability (Hansen et al., 2012). There were 27 hands with stage II, 40 with stage III, and 13 with stage IV degenerative changes. Mean age was 59 years (range 40–77). DEXA scans of the hands and carpal bones were carried out using a GE Lunar iDXA scanner (GE Healthcare, Waukesha, Wisconsin, USA). Hands were placed with the palm against the scanner bed. All scans were repeated after replacing the hand on the scanner bed for analysis of the precision of the method (scan and analysis repeatability). Thus, the total number of scans was 160. Image files were processed using the software program enCORE version 11.40 (GE Healthcare) by two independent observers. For each patient, the two observers separately outlined the circumference of the trapezium manually, and BMD was calculated based on the outlined area (Figure 1). The same observers repeated the measurement of the trapezium in all patients 8 weeks after the first measurement for calculation of intra- and interobserver variation (Figure 2).
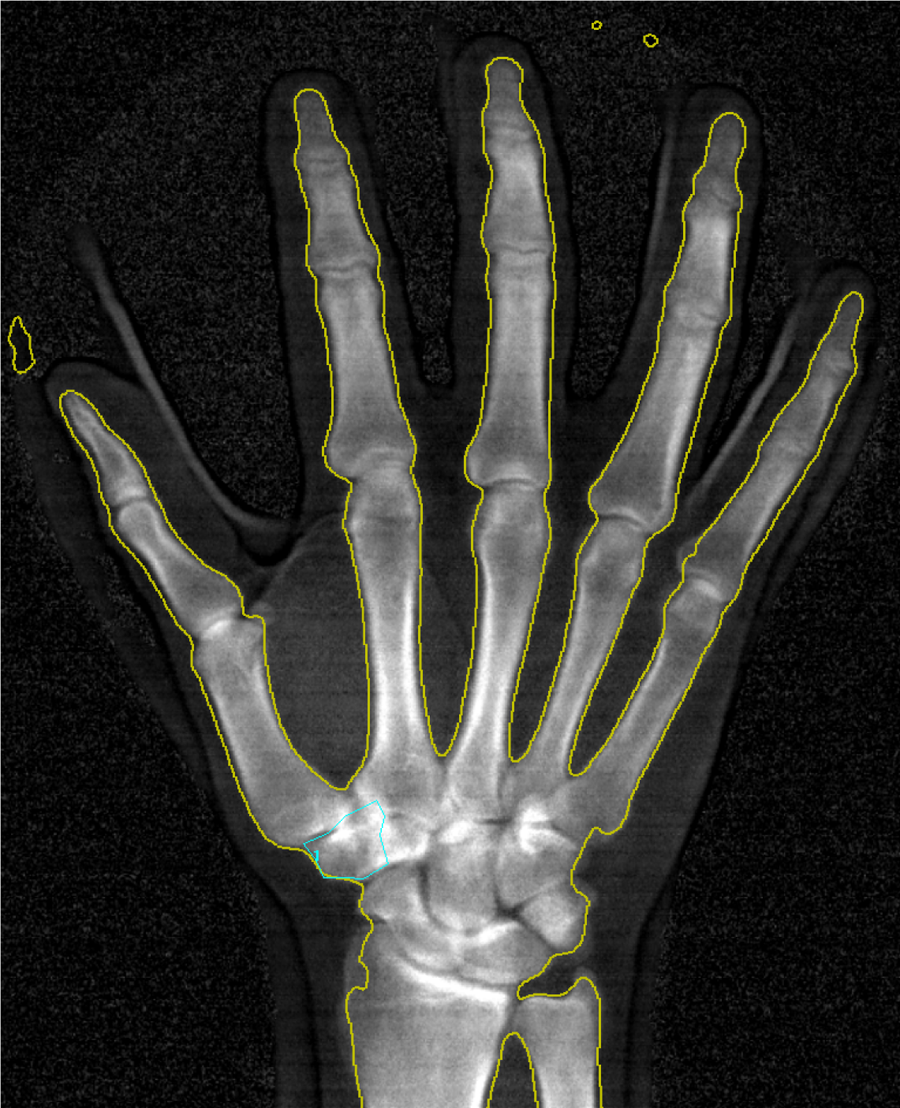
Marking the border of the trapezium for BMD measurement.
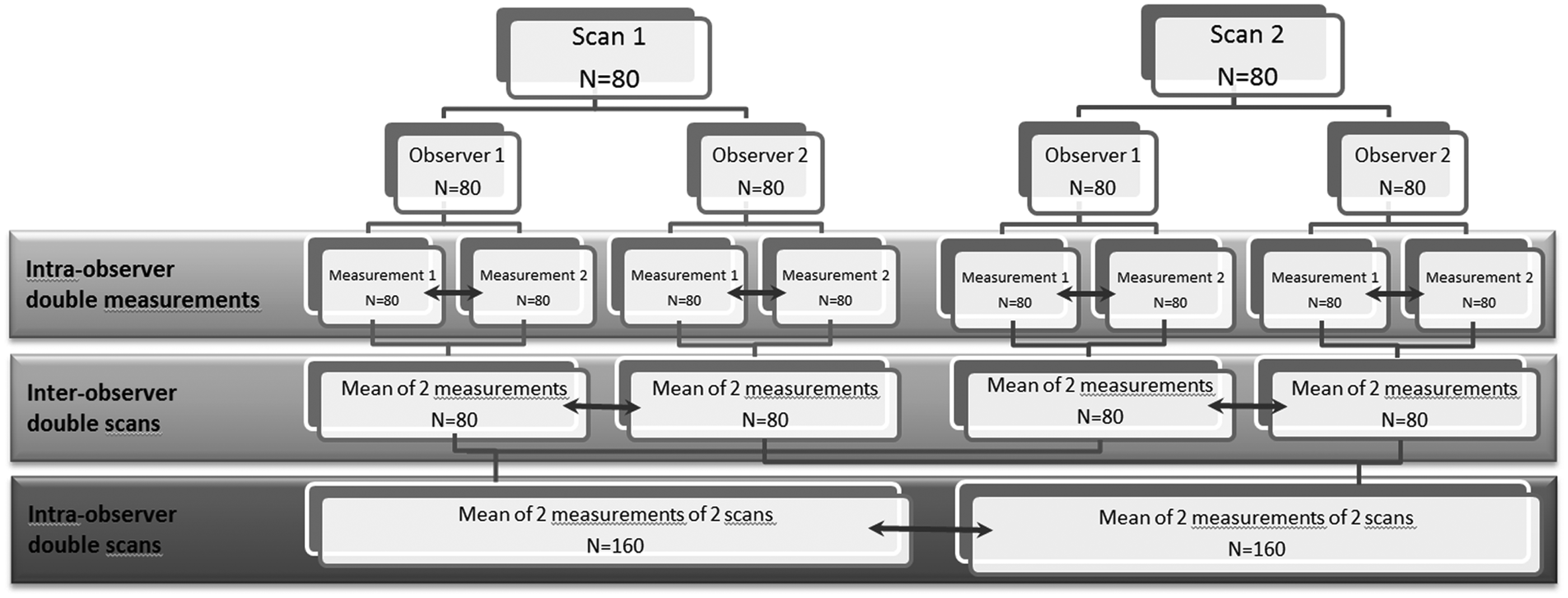
Summary of the analysis of the trapezium BMD measurements.
The correlation between BMD of the trapezium and radius was calculated using the measurements of one observer. In the radius, the enCORE software automatically defined the bone edge of the radius and calculated the BMD of both the distal radius and middle third of the radius. Manual corrections were done when necessary, if the automatic outlining of the radius was incorrect. The data were normally distributed (Shapiro–Wilk test). The correlation between the BMD of the trapezium and radius (both the distal and middle third of the radius) in each patient was calculated using Pearson’s test. The 95% confidence interval (CI) was calculated using Fisher’s transformation. Student’s t-test was used for comparison of mean values.
Results
The mean BMD of the trapezium was 0.65 g/cm2 in both repeated measurements and scans (Table 1). The difference in BMD between the two measurements of the trapezium on the same scan showed very good intra-observer agreement and an intra-class correlation coefficient (ICC) of between 0.95 and 0.97. In one observer (observer 2) we found a significant change from the first to the second evaluation of the scans, possibly indicating a learning curve, but the ICC was still 0.95 indicating that the change, although statistically significant, was not clinically relevant. Comparison of the BMD results of the two scans of the same trapezium also showed very good agreement with an ICC of 0.96 for both observers, signifying that the method is reproducible. The concordance correlation coefficient (CCC) of inter-observer agreement between the two observers was 0.96 when looking at the same scan. When combined with the repeated measurements the inter-observer CCC was reduced to 0.89, but this still indicated very good inter-observer agreement and that the method is reliable even in repeated scans with different observers.
Repeatability measurements (intra-observer) and concurrent validity (inter-observer) of trapezium BMD measurements on anteroposterior (AP) DEXA scans
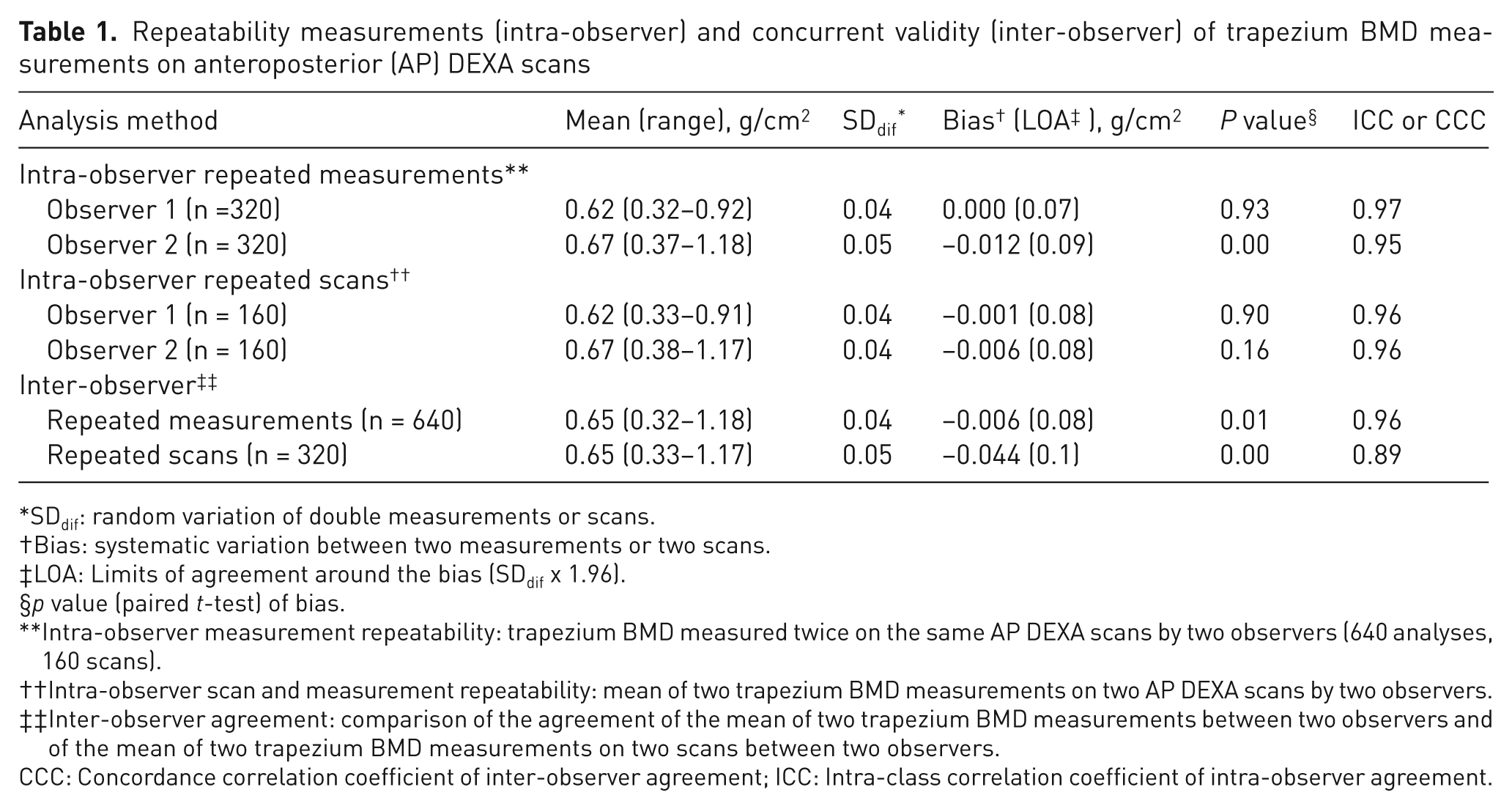
SDdif: random variation of double measurements or scans.
Bias: systematic variation between two measurements or two scans.
LOA: Limits of agreement around the bias (SDdif x 1.96).
p value (paired t-test) of bias.
Intra-observer measurement repeatability: trapezium BMD measured twice on the same AP DEXA scans by two observers (640 analyses, 160 scans).
Intra-observer scan and measurement repeatability: mean of two trapezium BMD measurements on two AP DEXA scans by two observers.
Inter-observer agreement: comparison of the agreement of the mean of two trapezium BMD measurements between two observers and of the mean of two trapezium BMD measurements on two scans between two observers.
CCC: Concordance correlation coefficient of inter-observer agreement; ICC: Intra-class correlation coefficient of intra-observer agreement.
The mean BMD of the trapezium was 0.59 (SD 0.12) g/cm2 in Eaton–Glickel stage II, 0.63 (SD 0.14) g/cm2 in Eaton–Glickel stage stage II, 0.63 (SD 0.14) g/cm2 in Eaton–Glickel stage III, and 0.70 (SD 0.21) g/cm2 in Eaton–Glickel stage IV. Comparing the mean BMD between Eaton–Glickel stages we found a significant difference between stage II and IV (p = 0.04), indicating an increase in BMD with progression in Eaton–Glickel stage, but no significant difference between stage II and III (p = 0.24) or stage III and IV (p = 0.15).
Pearson’s correlation coefficient between the mean BMD of the two measurements of the trapezium and distal radius was 0.63 (95% CI 0.51–0.96), and for the middle third of the radius it was 0.60 (95% CI 0.47–0.91). The correlation was moderate in men when the distal and middle radius were compared (Table 2) and better in women when compared with the distal radius. However, there was no significant difference between women and men due to the wide confidence intervals (Table 2).
Correlation between BMD of the trapezium and radius (both distal and middle third) in each patient
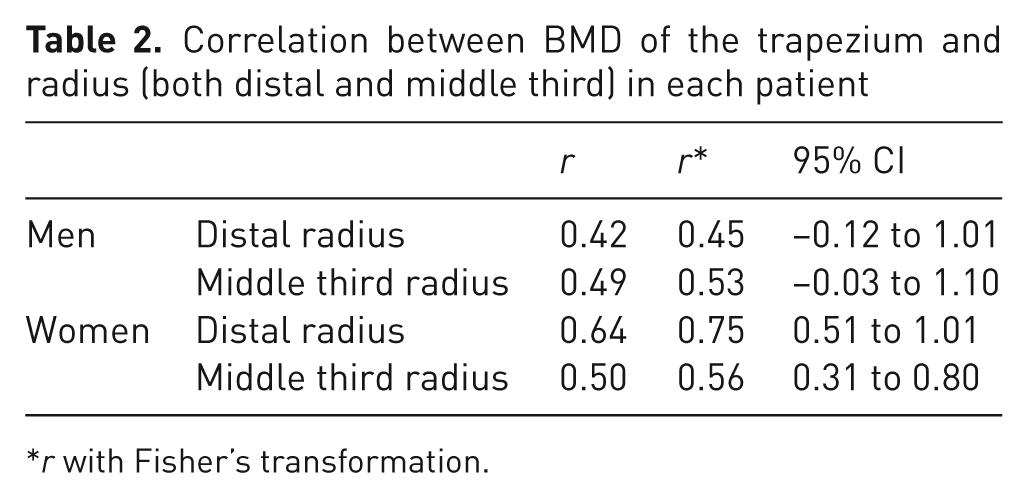
r with Fisher’s transformation.
Discussion
Before deciding on the implant type for treatment of osteoarthritis of the TM joint it would be of value to know the bone quality in the trapezium, because poor bone quality probably increases the risk of implant failure, especially with cementless implants. This study describes a novel and reproducible method for measurement of BMD of the osteoarthritic trapezium and is the first study to report large-scale BMD data for the osteoarthritic trapezium. Osteoarthritis in the TM joint reduces the joint space and changes the shape of the trapezium and centre of joint rotation (de Raedt et al., 2012; van de Giessen et al., 2011). This makes the identification of the borders of the trapezium difficult, as illustrated in Figure 1. Furthermore, the trapezium overlies the other carpal bones in the anteroposterior and most other views, which also makes it difficult to define the bone edge. We were concerned that technical problems with identifying the borders of the trapezium would result in a low precision of the BMD measurements, but analysis by two moderately experienced observers resulted in acceptable precision after repeated analyses, confirming good intra- and interobserver agreement. We accept that the overlap and sclerotic bone may cause a random error in measurements of the trapezium by the untrained observer or a technician with limited anatomical knowledge of the trapezium, and we are currently working on a more simple technique whereby only the BMD in the core of the trapezium is measured. BMD measurements of the trapezium are time-consuming, as the border of the trapezium has to be manually identified. Therefore, the use of available standardized measurements of the BMD of the radius as a surrogate for the BMD of the trapezium would be preferable. In our study the correlation between the BMD of the trapezium and radius was unfortunately only moderate. In contrast to our results, Brownbill and Ilich (2002) found a good correlation between the BMD of the hand and forearm (r = 0.82). However, they did not include the proximal carpal row in the BMD measurements and used the distal carpal bones plus the metacarpal and phalangeal bones as a measurement of the total BMD of the hand. The long bones of the hand and odd shape of the carpal bones are auto-identified as bone on a hand scan; however, the carpal bones are not outlined separately but are counted as a “block of bone” in the BMD measure of the hand. This makes the analysis of the total hand much simpler than outlining a single carpal bone. Brownbill and Ilich (2002) only included postmenopausal women, whereas in our study 21% of participants were men, which may be part of the explanation for our different results.
A study limitation is that we only compared the trapezium with the radius and not with other anatomical regions, but as BMD measurements of the hip do not predict BMD of the upper extremity (Wilson et al., 2009), we chose not to investigate whether another region such as the hip or lumbar spine correlated better with the trapezium than the distal radius.
Our study indicates the possibility of measuring the BMD of the trapezium alone with sufficient precision for clinical use. We were not able to look into the influence of gender and age on the BMD of the trapezium due to the relatively small number of patients in our study and because the variation in the BMD in our study group was large. Therefore, a study that includes more patients is needed before variation in the BMD of the trapezium can be sufficiently described. If direct measurements of the trapezium are not available, the BMD of the distal radius can provide only an indication of the bone quality in the trapezium.
Footnotes
Conflict of interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.