
Abstract
We describe our experience and outcome with the ‘Proximal first dorsal metacarpal artery free flap’. Ten consecutive cases utilizing the proximal first dorsal metacarpal artery free flap for complex digital defects were studied. Surgical technique, patient demographics, and flap outcome data were collected. Patient satisfaction was analysed using a questionnaire. All defects healed successfully with no loss of free flaps. The short-pedicle proximal first dorsal metacarpal artery free flap enables primary closure of the donor site up to 2 cm of width (in nine of the ten donor sites). The flap is a reliable and versatile alternative in selected cases of complex digital injuries.
Introduction
Defects of the hand and digits can be reconstructive challenges, but the ever-expanding potential list of flap donor sites aids flap selection. We describe another potential donor site using the proximal dorsal first web space skin supplied by the first dorsal metacarpal artery we call the proximal first dorsal metacarpal artery (PFDMCA) free flap.
Independently, Germann and Pelzer described the use of a neurotized free ‘kite flap’ (first dorsal metacarpal artery (FDMCA) flap) for the reconstruction of volar finger defects (Germann et al., 1997; Pelzer et al., 2004). They designed the flap distally on the dorsum of the index finger and metacarpophalengeal joint with a long pedicle, necessitating a skin graft for the donor site in all cases. We describe our modification of this flap using a short pedicle to allow primary closure of the donor site, and reduce the extent of donor and recipient site dissection. The aim of this study was to report on the feasibility and reliability of transferring the PFDMCA free flap to reconstruct defects of injured fingers, and evaluate the outcome, sensory reestablishment, and patient satisfaction after reconstruction.
Methods
A case series review on all patients who had PFDMCA free flap reconstructions, from February 2004 to May 2009, was conducted. A database was maintained that included patient demographics, defect characteristics, surgical technique, flap characteristics, intra-operative findings, complications, and flap outcome. All patients were followed and, in particular, the sensory restoration was monitored in terms of static and moving two-point discrimination. At the end of the study period, all patients were asked to complete a questionnaire about their satisfaction with flap appearance, size, sensibility and durability, and donor site appearance and pain. This survey was based on a visual analogue scale rated from 1 to 10: very dissatisfied (0–2), somewhat dissatisfied (2.1–4), neither satisfied nor dissatisfied (4.1–6), somewhat satisfied (6.1–8), and very satisfied (8.1–10).
Surgical technique
Either general anesthesia or regional nerve blocks were used depending on the extent of injury and patient preference. The skin island was designed on the dorsum of the first web space of the hand with the long axis of the flap centred over the course of the FDMCA. The FDMCA originates from the radial artery at the angle formed where the extensor pollicis longus tendon crosses the second metacarpal. It courses 2–3 mm radial and parallel to the shaft of the second metacarpal. It then divides into its terminal branches at the level of the second metacarpophalangeal joint. Unlike the free kite flap, in our design we did not extend the distal end of the flap onto the digit. By limiting the flap design no farther than the level of the metacarpophalangeal joint, direct closure of the donor site was possible (Figure 1(a)). Under tourniquet control, the incision was initially made on the radial margin of the designed flap and continued 1–1.5 cm proximally over the dorsal wrist. One or two small dorsal veins of diameters comparable to the potential recipient veins were carefully included in the dissection. Usually the cephalic vein is too large for convenient anastomosis. One or two branches of the radial sensory nerve were also dissected with the flap (Figure 1(b)). One has to be extremely careful not to injure any large direct cutaneous artery (Dautel et al., 1989; Sherif, 1994), which may run with the cutaneous nerve, as it may be the dominant supply to the flap instead of the FDMCA. The fascia of the interosseous muscle was then incised at the radial border of the flap and dissection was continued deep to this layer protecting the pedicle. Proximally, the pedicle was dissected to its origin from the radial artery (Figure 1(b)). Finally, the ulnar border of the flap was raised in the subfascial plane to complete the dissection. The donor site was usually closed primarily, otherwise a full-thickness skin graft was utilized. A digital artery and dorsal digital vein in close proximity to the defect were used as the recipient vessels. Nerve repair was performed in all cases in our study. Postoperatively, prophylactic doses of low molecular weight heparin (Clexane, 0.4 ml per day) were given to patients for 7 days and Rheodextran 10% (Infusia, Czech Republic; in continuous infusion 30 ml per hour) was administered for 1 to 2 days postoperatively to all the patients. The average hospitalization time was 7 days.
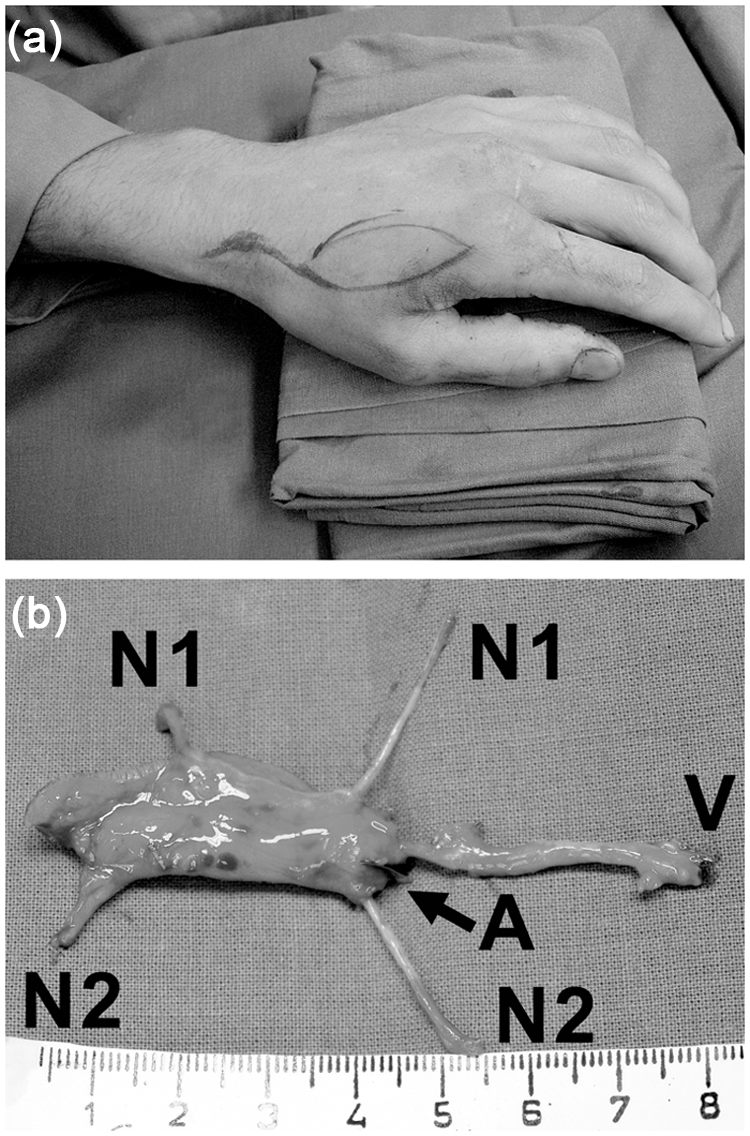
(a) Flap outlined on the dorsum of the hand. (b) Flap dissection complete with radial artery (A); radial sensory nerves (N1, N2); and dorsal veins (V) shown.
Our indications for the PFDMCA free flap included perceived unreliability of local or regional pedicled flaps owing to adjacent trauma (Figure 2); the need for a simultaneous reconstruction of the soft tissue and the digital nerve(s) defect(s) (Figure 3); or reconstruction of the pulp of the index finger or thumb (Figure 4).

(a) Injuries to multiple digits shown, with flap in place over proximal long finger defect. (b) Flap well healed.

(a) Index finger defect with segmental loss of digital nerve. (b) Flap well healed. (c) Donor site well healed.

Index finger pulp contact zone defect.
Results
Results are shown in Table 1. Ten patients were treated for coverage of traumatic volar digital defects. All the patients were males, with a mean age of 31 years (range 16–54). Nine of the ten free flaps were done immediately and one flap was performed for secondary reconstruction of a painful scar with poor durability and tendency to erosion. Except for one case of complex-hand injury requiring four-finger revascularization, all the flaps were ipsilateral.
Comprehensive patient, defect, flap, and outcome data.
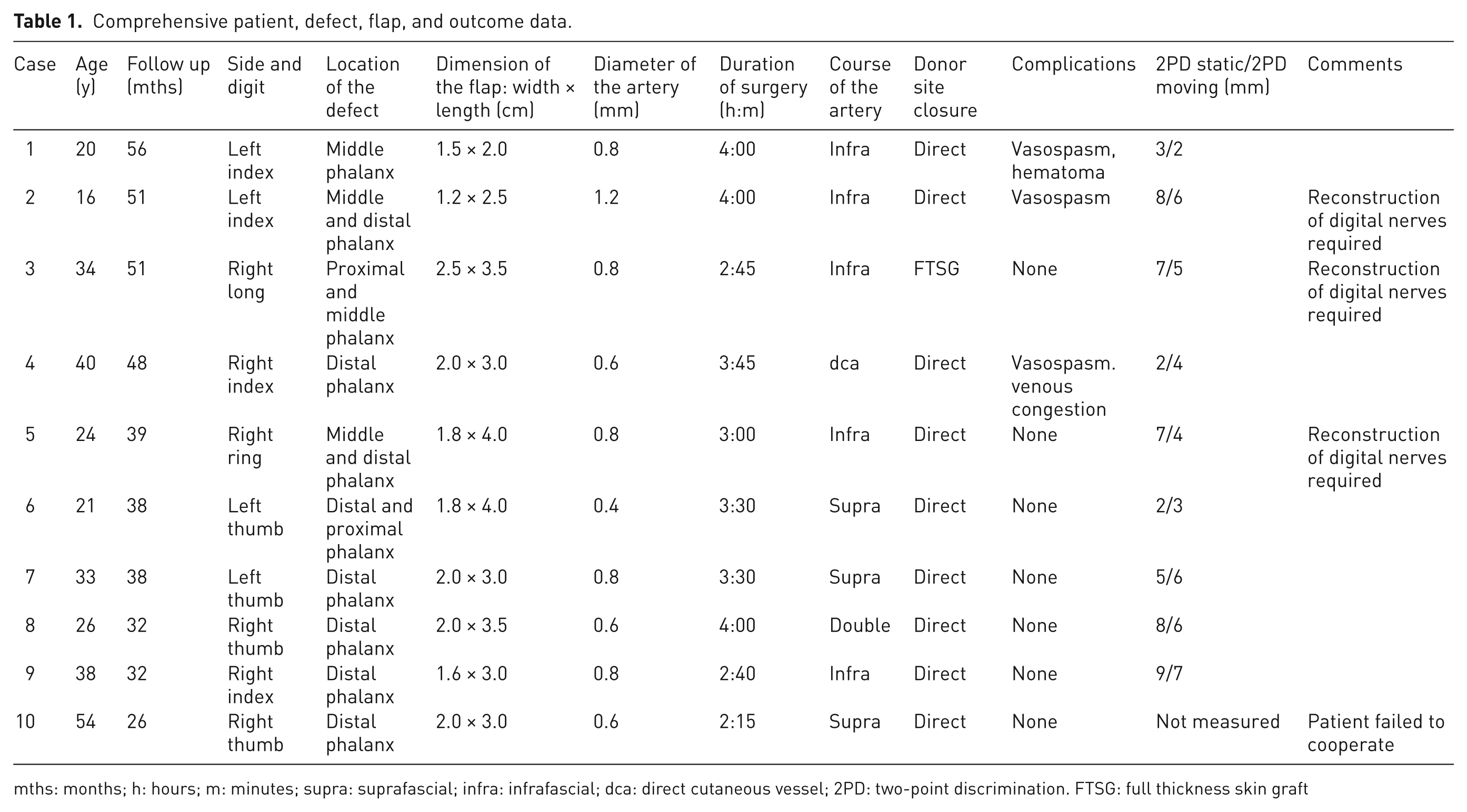
mths: months; h: hours; m: minutes; supra: suprafascial; infra: infrafascial; dca: direct cutaneous vessel; 2PD: two-point discrimination. FTSG: full thickness skin graft
The mean defect area was 5.89 cm2 (range 3–8.75). Four thumb and six digit defects were reconstructed. The mean diameter of the artery (FDMCA) was 0.75 mm (range 0.4–1.2). During the harvest of the flap we observed some anatomical variations of the pedicle: a dominant single FDMCA with a subfascial course (n = 5, 50%), a dominant single FDMCA with a suprafascial course (n = 3, 30%), two co-dominant FDMCAs with both a suprafascial and subfascial course (n = 1, 10%), and one dominant direct cutaneous artery without a sizeable FDMCA (n = 1, 10%). The mean duration of surgery was 3 hours and 20 minutes (range 2 hours, 15 minutes to 4 hours).
All ten free flaps survived and defects healed completely. The mean follow-up time period was 38.1 months (range 26–56). The re-established mean static two-point discrimination was 5.6 mm (range 2–9); and moving two-point discrimination was 4.7 mm (range 4–7).
Complications
One flap (Case 4) developed venous congestion and was explored 6 hours post-operatively. The dorsal vein was kinked and needed to be shortened, which resolved the problem. We observed intra-operative flap ischemia from prolonged and persistent (> 20 minutes) vasospasm in three flaps (Cases 1, 2, and 4). One flap (Case 1) had a hematoma and needed it evacuated 5 hours after surgery. The other two flaps required subadventitial injection of 10% magnesium sulfate (Biotika, Slovenska Lupca, Slovak Republic) to relieve the vasospasm.
Donor site closure and morbidity
The donor site was closed directly in nine cases (Figure 3(c)), all with widths ≤ 2 cm. The only site (Case 3) that required a full thickness skin graft from the groin had a width of 2.5 cm. No donor site morbidity or problems with abduction of the thumb were observed.
Patient satisfaction questionnaire
As can be seen in Table 2, of the ten patients, nine completed the questionnaire at the end of the study (patient 2 did not cooperate). On average, patients were ‘somewhat satisfied’ (mean score of 7.0/10) with flap and donor site appearance and size. On average they were ‘neither satisfied nor dissatisfied’ (mean score of 5.3/10) with the flap sensibility and durability. Two patients had residual pain at the donor site. No patient with thumb defect reconstruction reported cortical misrepresentation.
Data from patient satisfaction questionnaire.
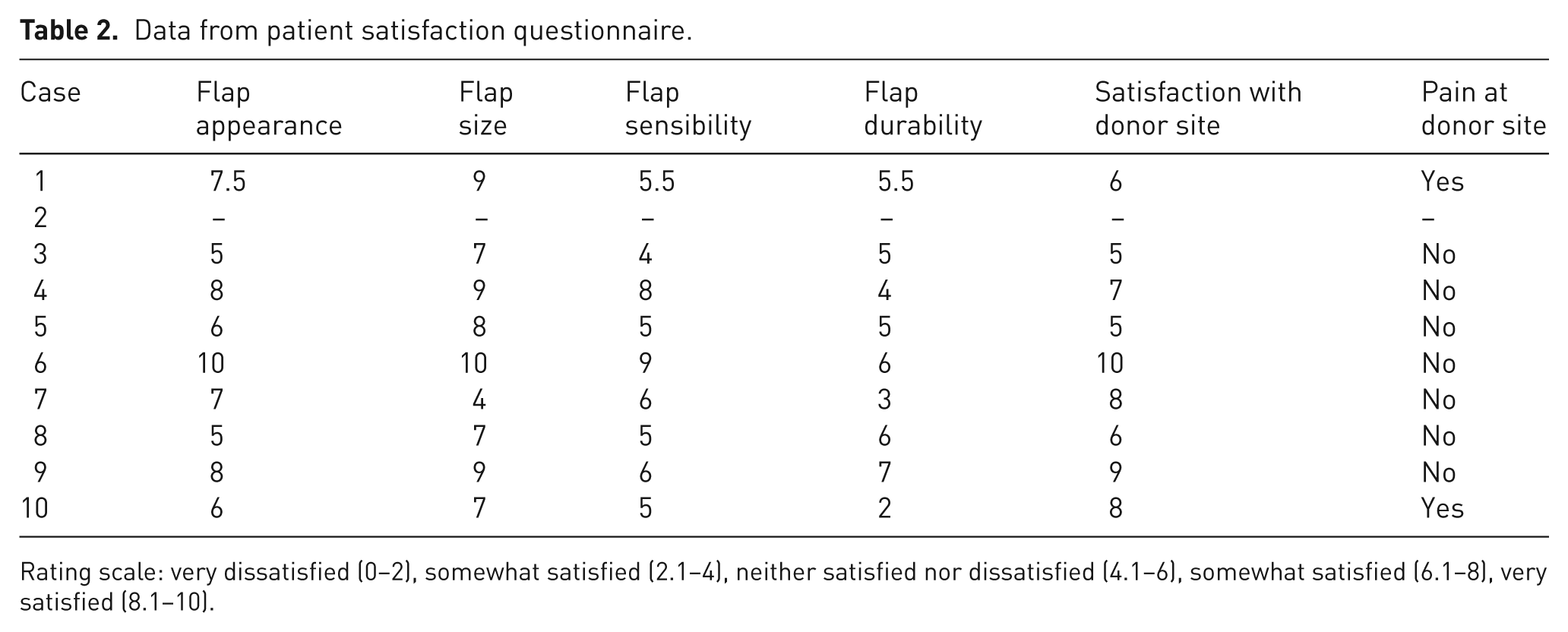
Rating scale: very dissatisfied (0–2), somewhat satisfied (2.1–4), neither satisfied nor dissatisfied (4.1–6), somewhat satisfied (6.1–8), very satisfied (8.1–10).
Discussion
Traumatic injuries of the hand that require flap surgery for soft tissue defects are common problems encountered by reconstructive surgeons.
Free tissue transfers have the potential to circumvent some of the disadvantages of pedicled loco-regional flaps, such as: the sacrifice of one of the digital arteries/nerves (Niranjan and Armstrong, 1994; Sapp et al., 1993); the need for skin grafts to close donor sites (Koch et al., 2005; Pelisier et al., 1999); poor sensibility of the transferred flap (Lassner et al., 2002; Nicolai and Hentenaar, 1981); and possible venous congestion in reverse flow flaps (Takeishi et al., 2006; Vuppalapati et al., 2004). There are some definite advantages of using free flaps, including easier inset of the flap and less dissection of the donor site. Another advantage may be decreased ‘double sensibility phenomenon’ or cortical misrepresentation in comparison with heterodigital pedicled neurovascular flaps (Adani et al., 1994; Markley, 1977; Rose, 1989; Stice and Wood, 1987). On the other hand, the potential thrombotic complications leading to flap failure and longer surgical time may discourage many from pursuing this reconstructive option.
The pedicled first dorsal metacarpal artery flap, originally described by Foucher and Braun (1979), and referred to as the ‘kite flap’ is able easily to reach the tips of the index finger or thumb (Pelisier et al., 1999; Takeishi et al., 2006; Vuppalapati et al., 2004). The free ‘kite flap’ is well suited for coverage of digital defects with many favourable attributes, including its constant anatomy (Dauphin and Casoli, 2011), relatively simple dissection, sensory potential, and the capability to perform the procedure under locoregional anesthesia (Germann et al., 1997; Pelzer et al., 2004). Although glabrous skin would be ideal for the reconstruction of pulp and border contact areas, the dorsal skin of the hand in the free kite flap is rather durable.
The proximal short pedicle modification that we describe ensures that the FDMCA is not as exposed because most of the pedicle is covered by the flap at all times. It also means that the flap is not dependent on the small terminal vessels of the FDMCA, but rather more proximal, larger, perforators. This potentially makes the flap more reliable and its perforators less prone to vasospasm, supported by the 0% flap loss rate in our study. Improved sensory reestablishment is another possible advantage of the PFDMCA free flap. The two point discrimination after non-innervated pedicled flaps have been reported at 9 mm (Freedlander et al., 1986), compared with the mean of 5.6 mm our study reports.
Two flaps in our case series required treatment of the vasospasm using magnesium sulphate (Hyza et al., 2009). At the time of the study, Rheodextran 10% was administered postoperatively although its routine use in microsurgery was controversial. Currently it is not used in our department.
In certain clinical situations, the PFDMCA free flap may be particularly well suited, such as when microsurgery is being utilized for digital nerve or vessel repair, when the defect is large, or when scars or injuries prevent the use of pedicled homodigital or heterodigital flaps. Another imaginative use of the PFDMCA free flap is in cases of digital nerve loss in which the nerve of the flap can be used as an interpositional, vascularized nerve graft.
Conclusions
Local flaps of the hand remain the technique of choice for the reconstruction of most digital defects; however, the PFDMCA free flap is a viable alternative in selected cases of complex digital injuries. This flap is reliable and versatile, with low donor site morbidity and good patient acceptance. The disadvantage of the flap is longer surgical time in comparison with pedicled flaps.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of intrests
All named authors hereby declare that they have no conflicts of interest to disclose.