
Abstract
This review summarizes the literature regarding venous thromboembolism and examines the prophylaxis guidelines with relation to hand, wrist and elbow surgery. We performed an extensive literature search identifying any relevant case reports or outcome studies. Of 680 potential articles, only four contained data relevant to thrombosis after elbow, wrist and hand surgery. No isolated deep vein thromboses and only nine pulmonary embolisms were identified suggesting that the rate of venous thromboembolism is extremely low following this subset of upper limb surgery. We identified nine guidelines, of which only two (the British Society for Surgery of the Hand and the National Institute of Health and Clinical Excellence) addressed the upper limb. We present a set of recommendations based on the results of this review.
Introduction
Venous thromboembolism (VTE), encompassing both deep vein thrombosis (DVT) and pulmonary embolism (PE), is an important cause of both morbidity and mortality following major surgical procedures. The treatment of non-fatal symptomatic VTE and related long-term morbidities is associated with a considerable cost to health services. Most epidemiological and prevention data in orthopaedic surgery have been accumulated from studies of patients undergoing hip and knee arthroplasty. The risk of VTE after lower limb major surgery is considerably higher than elbow, wrist and hand surgery.
Guidelines are generally accepted as a means of ensuring thromboprophylaxis is given to those that may benefit, without incurring disproportionate risk or expense (Warwick et al. 2008). There appears to be very little guidance for hand surgeons. Advice for lower limb surgery could lead to unjustified expense and unnecessary risk of side-effects when translated to the upper limb.
We present a review of the literature quantifying the rate of VTE after elbow, wrist and hand surgery, together with a critique and comparison of thromboprophylaxis guidelines.
Methods
We examined the electronic databases Medline, EMBASE, Cochrane database and CINAHL with no date restriction. We used the following keywords or phrases: deep vein thrombosis; pulmonary embolism; venous thromboembolism; upper limb orthop(a)edic; upper limb plastic; elbow surgery; wrist surgery; hand surgery. The titles and abstracts in English or English translations via the database were downloaded and analysed. All case reports, review articles, outcome studies and trials in relation to VTE following elbow, wrist and hand (elective and trauma) surgery were selected and the full text was examined in further detail. The references cited within the selected articles were examined for any further relevant articles.
The existence of guidelines was derived from the senior author’s work elsewhere in the field of VTE as well as internet search engine results incorporating a variety of regions across the globe. Nine guidelines were reviewed from Europe, North America and Australasia relating to the prevention of VTE. The British Society for Surgery of the Hand (BSSH, 2011); National Institute for Health and Clinical Excellence (NICE, 2010); Scottish Intercollegiate Guidelines Network (SIGN, 2010); International Consensus Statement (ICS) (Nicolaides et al., 2006); American College of Chest Physicians (ACCP) (Falck-Ytter et al., 2012); American Academy of Orthopaedic Surgeons (AAOS, 2011); Institute for Clinical Systems Improvement (ICSI, 2011); National Health and Medical Research Council (NHMRC, 2009); and The Australia and New Zealand Working Party (ANZWP, 2007).
Results
Literature review
We found 737 cited articles within the four databases we searched (Medline 554; EMBASE 145; CINAHL 32; Cochrane 6). We removed duplicates, citations regarding VTE following surgically and conservatively managed shoulder complaints, which is out of the remit for this review, and any other studies that were irrelevant to upper limb surgery. Only four articles were included. In one there were three occurrences of VTE (Duncan et al., 2007), a second highlighted four occurrences (Krenek et al., 2011) and the remaining two identified single occurrences (Basat et al., 2011; Jupiter et al., 2002). The relevant anatomic sites are shown in Table 1.
Literature search results per region
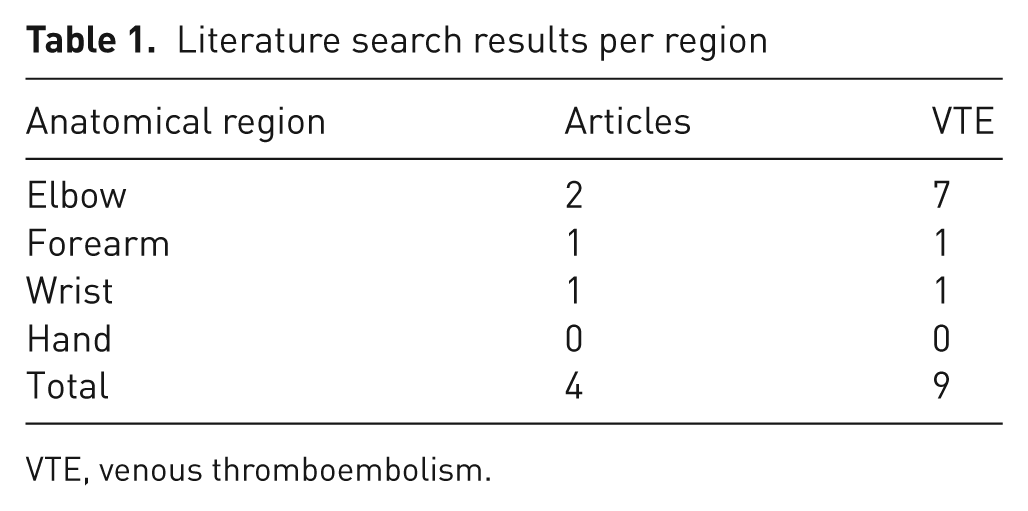
VTE, venous thromboembolism.
Elbow
In a case series from the Mayo clinic, three PEs (one fatal) occurred after 1076 total elbow arthroplasties equating to an incidence of 0.28% (Duncan et al., 2007). Standard mechanical prophylaxis was used (intermittent calf compression device and graduated compression stockings). One patient who had a PE underwent four-limb ultrasound surveillance, which found no evidence of upper or lower limb DVT. This suggests a pelvic DVT possibly as a consequence of immobility during the procedure.
A more recent outcome study from the University of California, Los Angeles (UCLA) had comparable rates with four PEs (two fatal) after 1625 total elbow arthroplasties (0.25%) (Krenek et al., 2011). No details were given regarding associated upper or lower limb DVT nor information about the methods of thromboprophylaxis that were used.
Forearm, wrist and hand
One non-fatal PE occurred after distal radius fixation following an acute fracture (Jupiter et al., 2002). There is no mention of the site of origin (upper or lower limb DVT), nor details regarding the use of mechanical prophylaxis in the operating room; however there had been abdominal surgery 14 days prior to this procedure. This would have independently increased the susceptibility of VTE.
There has also been one report of a non-fatal PE with an associated asymptomatic upper limb DVT following revision osteosynthesis of the proximal diaphysis of the ulna (Basat et al., 2011). This article included no details of the use of prophylaxis; the procedure took 110 minutes.
There have been no reports of VTE following elective or trauma hand and wrist surgery, nor any report of VTE following upper limb orthopaedic or plastic surgery under local or awake regional anaesthesia. None of the above articles recorded the precise anaesthesia used.
Guidelines
The recommendations from the available guidelines are listed below in order of region and year of publication, and in full as written in the individual guidelines. Table 2 gives a summary of these recommendations.
Summary of guideline recommendations
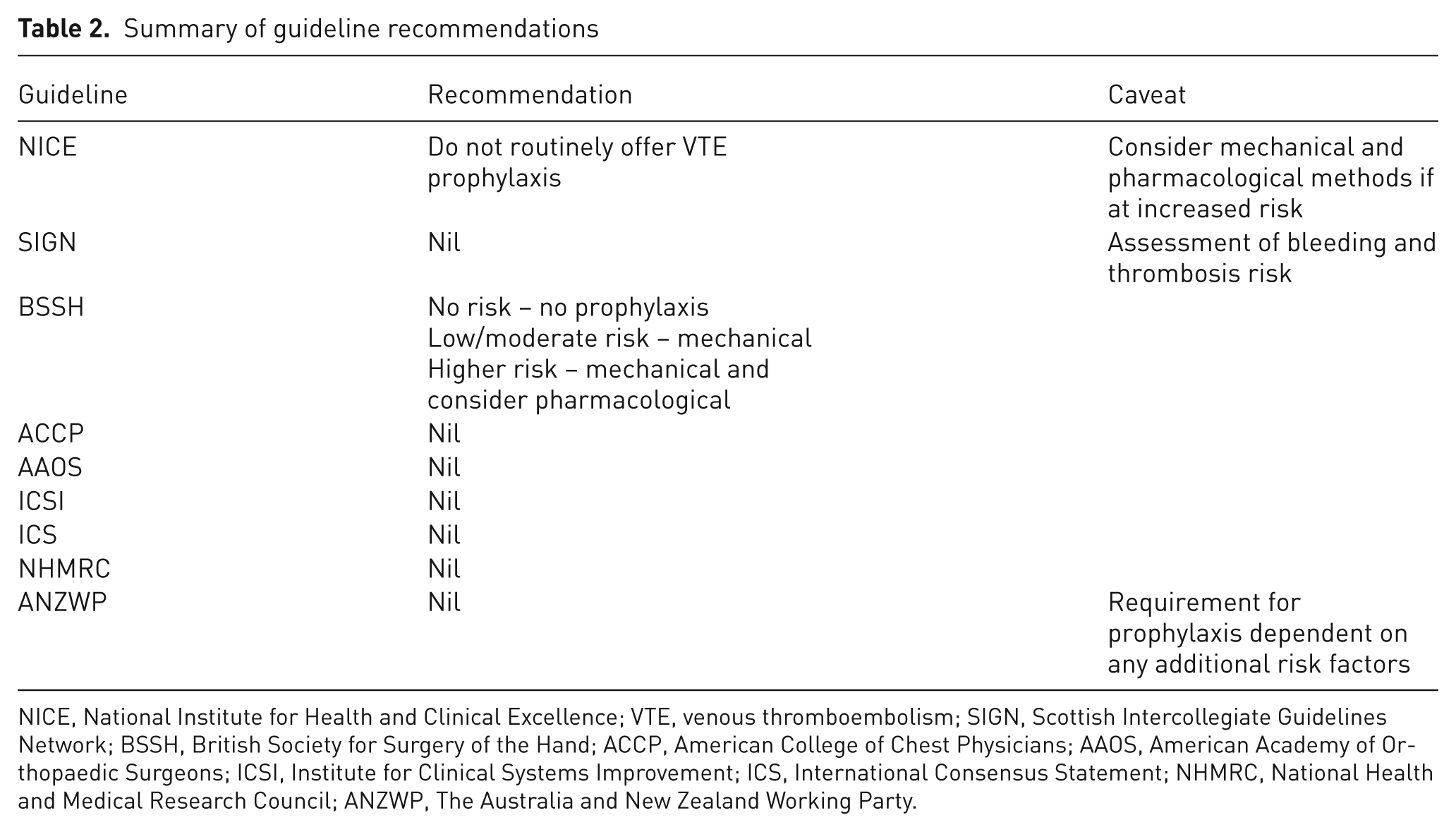
NICE, National Institute for Health and Clinical Excellence; VTE, venous thromboembolism; SIGN, Scottish Intercollegiate Guidelines Network; BSSH, British Society for Surgery of the Hand; ACCP, American College of Chest Physicians; AAOS, American Academy of Orthopaedic Surgeons; ICSI, Institute for Clinical Systems Improvement; ICS, International Consensus Statement; NHMRC, National Health and Medical Research Council; ANZWP, The Australia and New Zealand Working Party.
Europe
No risk
Upper limb procedure under general anaesthesia (GA) <90 minutes duration, without risk factors.
Upper limb procedures under local or regional blockade, with or without risk factors.
No prophylaxis required.
Low or moderate risk
Upper limb procedure under GA >90 minutes.
Upper limb procedure under GA and ancillary lower limb procedure >60 minutes.
Upper limb procedure under GA and one additional risk factor.
Use mechanical compression devices in the operating room and until mobile.
Higher risk
Upper limb procedure under GA >90 minutes and >1 risk factor.
Upper limb procedure under GA and ancillary lower limb procedure >60 minutes and >1 risk factor.
Use mechanical compression devices in the operating room and until mobile.
Consider low molecular weight heparin (LMWH) started no less than 6 hours postoperatively until fully mobile.
Beware alternative risk of bleeding in some procedures.
Carefully document the balanced decision for the individual patient.
Patient may need to continue LMWH after discharge from hospital.
Assess all patients on admission to identify those who are at increased risk of VTE.
Upper limb surgery
Do not routinely offer VTE prophylaxis to patients undergoing upper limb surgery. If a patient is assessed to be at increased risk of VTE refer to recommendation for other orthopaedic surgery.
Other orthopaedic surgery
Consider offering combined VTE prophylaxis with mechanical and pharmacological methods to patients having orthopaedic surgery (other than hip fracture, hip replacement or knee replacement) based on an assessment of risks and after discussion with the patient.
Start mechanical VTE prophylaxis on admission. Choose one of the following, based on individual risk factors: anti-embolism stockings (thigh or knee length), used with caution; foot impulse devices; intermittent pneumatic compression devices (thigh or knee length). Start pharmacological VTE prophylaxis 6–12 hours after surgery. Choose one of: LMWH; unfractionated heparin (UFH) (for patients with renal failure). Continue pharmacological VTE prophylaxis until the patient no longer has significantly reduced mobility.
Local anaesthesia
Do not routinely offer pharmacological or mechanical VTE prophylaxis to patients undergoing a surgical procedure with local anaesthesia (LA) by local infiltration with no limitation of mobility.
No mention of upper limb surgery.
Other orthopaedic surgery
The evidence for, and efficacy of, pharmacological thromboprophylaxis for more minor orthopaedic procedures is weak. Patients with additional risk factors for VTE, such as previous VTE, should be considered for additional extended prophylaxis.
No mention of upper limb surgery.
North America
No mention of upper limb surgery.
Major orthopaedic surgery
For patients receiving LMWH as thromboprophylaxis in major orthopaedic surgery, we recommend starting either preoperatively or postoperatively. For patients receiving fondaparinux as thromboprophylaxis in major orthopaedic surgery, we recommend starting either 6 or 8 hours after surgery or the next day.
No mention of upper limb surgery.
No mention of upper limb surgery.
Australasia
No mention of upper limb surgery.
No mention of upper limb surgery.
All other surgery
The requirement for prophylaxis for all other surgery is dependent on any additional VTE risk factors that the patient may carry including immobility, thrombophilia, oestrogen therapy, pregnancy or puerperium, active inflammation, strong family history of VTE and/or obesity. These factors, if present, will require consideration for prophylaxis. Otherwise there are no specific recommendations regarding prophylaxis other than the option of graduated compression stockings.
Discussion
The literature suggests that the frequency of VTE following hand, wrist and elbow surgery is extremely low. Only nine cases have been reported; all were PE with no occurrences of upper or lower limb symptomatic DVT as a primary diagnosis. Seven of these nine VTE events were secondary to total elbow arthroplasty (three fatal) having an overall incidence of fatal PE of 0.11% and non-fatal PE of 0.15%. This is lower than the 0.34% and 1.20% frequency seen after hip replacement (Warwick et al., 1995). The Scottish Arthroplasty Project identified a fatal PE rate of 0.22% following 44,785 hip replacements (Howie et al., 2005). As a control group, this same study determined a fatal PE rate of 0.12% at one year after cataract surgery having a comparable rate following total elbow arthroplasty as determined from this review.
Chemical prophylaxis carries the risk of complications. Since the overall rate of complications following total elbow arthroplasty is much higher than other joint replacements, especially wound problems and infection (Kim et al., 2011; Voloshin et al., 2011), this may increase further if chemical thromboprophylaxis were to be used. Only those with a particularly high risk of VTE are likely to benefit from chemical prophylaxis; however the published rate of PE would probably justify routine mechanical prophylaxis for elbow arthroplasty.
The length of immobilization is an independent risk factor for lower limb VTE (Heit et al., 2001). According to the NICE guidelines, a patient is at a potentially increased risk of VTE during upper limb surgery if the total anaesthetic and surgical time is greater than 90 minutes. In this situation it is deemed appropriate to use intra-operative mechanical thromboprophylaxis, ongoing if immobility continues postoperatively. This may be pertinent, for example, in cases of complex elbow trauma or when iliac crest grafting is needed.
The use of regional anaesthesia has been shown to reduce significantly the incidence of DVT following hip fracture surgery (Urwin et al., 2000), but owing to the low incidence of VTE following upper limb surgery it is not possible to extrapolate these data. The articles examined in this review did not specify the method of anaesthesia and therefore the length of intra-operative and/or postoperative immobility may be a more significant risk factor.
The prevalence of asymptomatic DVT and PE following elbow, wrist and hand surgery is unknown because there are no relevant studies with routine screening. The only reasonably comparable information is a screening study following shoulder arthroplasty. Willis et al., (2009) identified a DVT rate of 13% in the postoperative period using routine four-limb Doppler ultrasound surveillance for all patients. Over half of these were in the lower limb. This rate is comparable to hip arthroplasty studies (Liebermann and Geerts, 1994; Sudo et al., 2003). It would suggest that asymptomatic upper and lower limb DVTs occur quite frequently following relatively prolonged shoulder surgery. However, it may be that shoulder surgery increases the risk of VTE owing to manipulation of the axillary–brachial vein during joint dislocation and systemic release of thromboplastins during reaming and implant insertion. If so, rates from shoulder surgery should not be extrapolated to elbow, wrist and hand surgery.
The limitation of this review is that it is not possible to identify accurately the true rate of VTE following elbow, wrist and hand surgery. This would rely on surgeons reporting complications and therefore the literature almost certainly underestimates the true incidence. The study only looked at databases that search for articles written in the English language and not all non-English language articles. It was therefore not possible to identify the true incidence in the worldwide literature.
Upper limb DVT accounts for 0.15% of hospitalized patients (Mustafa et al., 2003) and for 1–4% of the total DVT rate (Sajid et al., 2007). Several studies have analysed the risk factors and different aetiologies of upper limb DVT and orthopaedic or plastic upper limb surgery was not deemed a risk factor (Joffe et al., 2004; Kommareddy et al., 2002; Lee et al., 2012; Martinelli et al., 2004; Mustafa et al., 2003; Sajid et al., 2007). These DVTs generally relate to malignancy, indwelling venous catheter, proximal venous occlusion or thrombophilia. A previous review examining solely upper limb DVT rates following all types of orthopaedic surgery (including spinal surgery) found no occurrences after orthopaedic elbow, wrist and hand surgery (Smith et al., 2011). Our review has found only one case of a confirmed asymptomatic upper limb DVT that was detected following investigation after a PE occurred secondarily to proximal ulna fixation (Basat et al., 2011). No cases of isolated symptomatic upper limb DVT after hand, wrist or elbow surgery have been identified.
Recommendations
Surgeons operating on the elbow, wrist and hand should realize that VTE is rare but is a possibility after major elbow surgery and major forearm reconstruction.
The guidelines written by BSSH are the most comprehensive, but have not been published in the literature. This article aims to present the literature base and rationale on which these guidelines were prepared, since the senior author of this article was engaged by the BSSH to prepare their guidelines. The published guidelines from Europe, North America and Australasia do not include specific stratification for the use of thromboprophylaxis in forearm surgery and indeed most do not even allude to this surgical sub-speciality.
We recommend that risk factors should be sought for those having prolonged elbow and osseous forearm surgery because of the potential for VTE suggested by the literature (Table 3). For the small subgroup deemed to be at risk, prophylaxis is recommended (Table 4). For those patients undergoing short-duration elbow, wrist and hand soft tissue surgery using local or regional anaesthesia, risk assessment is not required given the negligible risk of VTE. Formal exclusion of such cohorts from routine risk assessment would save unnecessary assessment time.
Risk factors for VTE
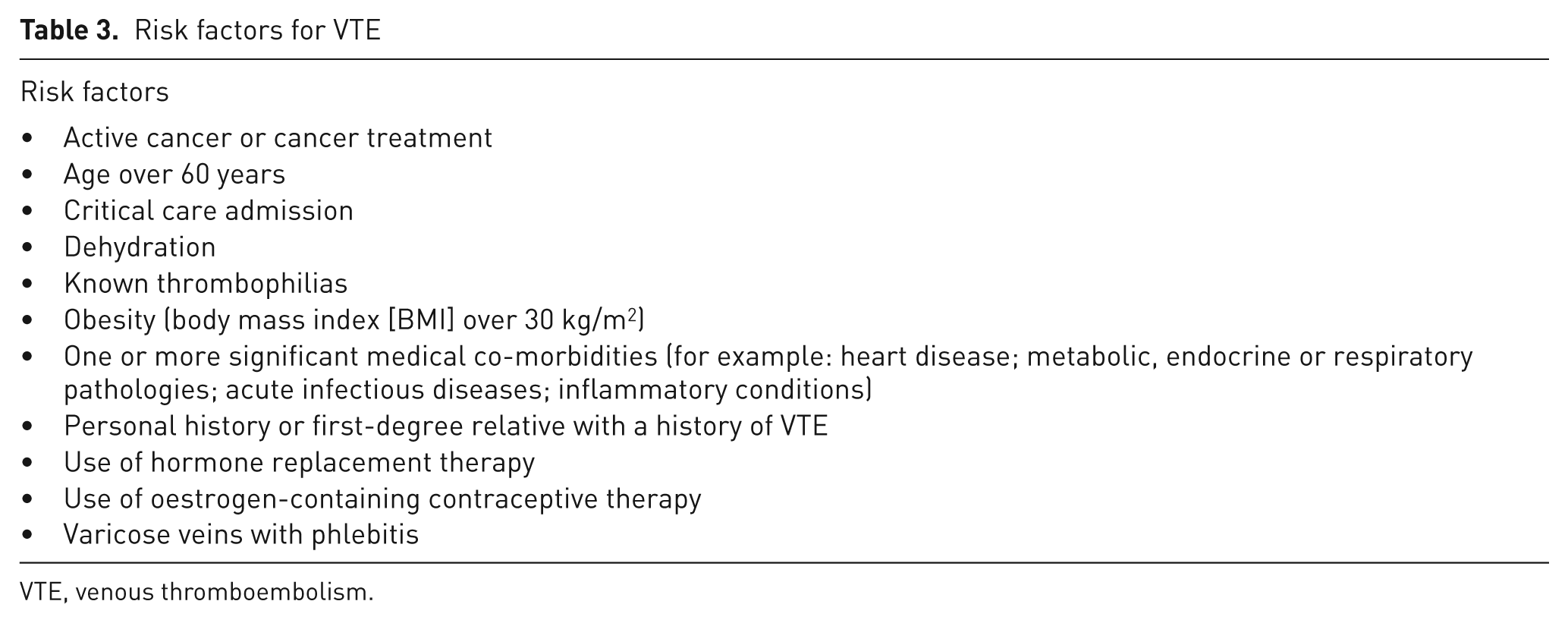
VTE, venous thromboembolism.
Recommendation for prophylaxis in hand, wrist and elbow orthopaedic surgery
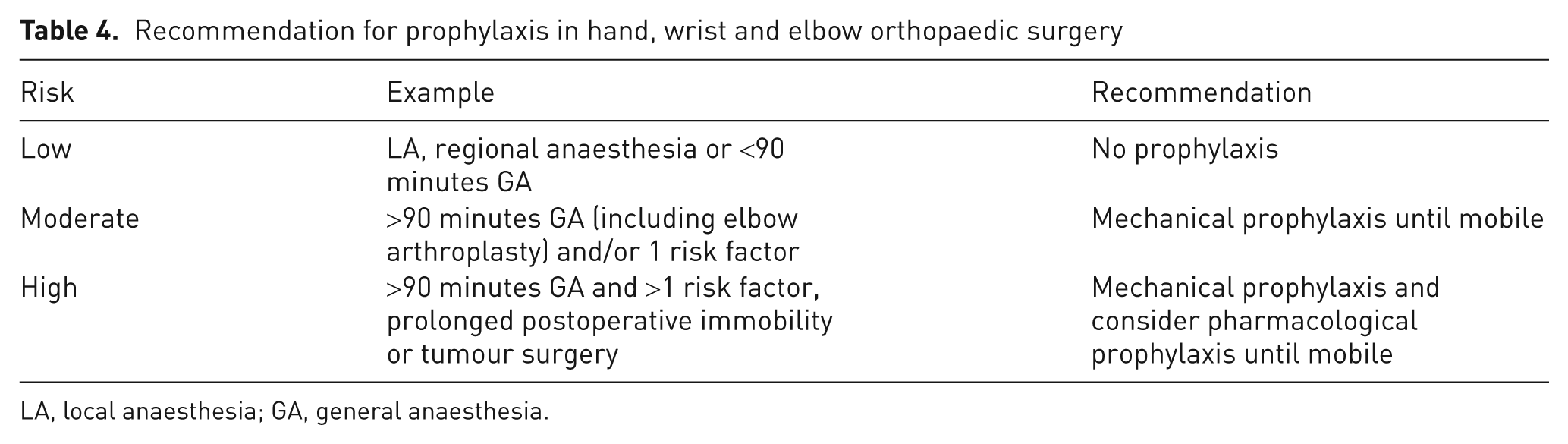
LA, local anaesthesia; GA, general anaesthesia.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interests
David Warwick is an editorial member of the International Consensus Statement and a member of the NICE Orthopaedic VTE Guidelines Group. He has in the past received honoraria and travel funding from various companies involved in VTE prophylaxis to include Bayer, BMS, Sanofi Aventis, Orthofix, Novamedix, Boehringer Ingelheim, Novamedix, Glaxo, Covidien. He is currently involved in research into novel mechanical prophylaxis techniques.