
Abstract
We prospectively assessed the subjective, objective, and radiographic results at 1, 2, and 5 years in 65 patients who had pyrocarbon proximal interphalangeal prostheses inserted between 2001 and 2010. Further operations were done on 10 of the 89 joints (four for prosthetic extraction and arthrodesis, two for component changes, and four for soft tissue procedures). At 1 year, the visual analogue scale score for pain at rest had improved to 0 cm from a pre-operative 4 cm, pain at activity from 6 to 1.8 cm, and Disability of the Arm, Shoulder and Hand score from 40 to 25. Range of movement and grip strength were unchanged. At 5 years, 31 joints (21 patients) had a complete radiographic follow-up. Seven proximal and 12 distal components showing zones of osteolysis at 1 year had stabilized and were inert or integrated at 5 years. Three proximal and three distal components had osteolytic zones at 5 years. Forty-seven of 59 patients were pain-free at rest at 1 year, and 19 of 21 at 5 years. No late revisions or loosening occurred.
Introduction
The proximal interphalangeal (PIP) joint is important for grip function in the hand. In primary and post-traumatic osteoarthritis, contracture and pain can lead to limitations in daily activities. Arthrodesis is a common surgical method in use for pain relief but other methods, such as palmar plate interposition, silicone interposition, or implant arthroplasty (Merle et al., 2012; Tagikawa et al., 2004), aim to preserve joint motion. In 2001, a pyrocarbon PIP prosthesis (Ascension®, Austin, Texas, USA) was introduced. Pyrocarbon is a form of carbon; it is durable, tissue compatible, and wear resistant compared with previous materials used for small implant arthroplasty. It has an elastic modulus similar to cortical bone, which minimizes shear at the interface and thereby minimizes the relative motion between prosthesis and surrounding bone (Cook et al., 1981). Pyrocarbon was first introduced in medicine in 1969 for use in artificial heart valves, but was soon used for metacarpophalangeal (MCP) joint arthroplasties. Several new prosthetic designs for various joints have been developed in hand surgery since the 12 year follow up of pyrocarbon MCP prostheses by Cook et al. (1999).
We started to use the pyrocarbon PIP prosthesis in December 2001, and patients receiving this prosthesis have since been followed-up consecutively and prospectively, from the pre-operative stage to 1, 2, and 5 years. Our short-term results have been published (Wijk et al., 2010), and showed good pain relief but no improvement in range of motion (ROM). Other centres have also reported good short- to medium-term results with decreased pain and acceptable revision rates, but without major improvement in ROM (Bravo et al., 2007; Chung et al., 2009; Hutt et al., 2012; Nunley et al., 2006; Tuttle and Stern, 2006; Watts et al., 2012). In some centres, concerns have been raised about the fixation (Daecke et al., 2012), prosthetic migration (Herren et al., 2006), and high reoperation rates (Daecke et al., 2012; Pritsch and Rizzo, 2011). A recent medium-term report indicated poor results for the ROM, loss of position of the prosthesis over time, and a high rate of revision (Sweets and Stern, 2011).
In the present study, we report our results of all PIP pyrocarbon prosthesis inserted at our centre between 2001and 2010. We also report a radiographic analysis for the subgroup of the first 34 joints (24 patients) who have attended or were due for the 5 year follow-up.
Methods
Patients
Between 2001 and 2010, 65 patients (89 joints) underwent PIP arthroplasties using the Ascension® PIP pyrocarbon implant. Fifty-six patients were women and nine men. The mean age was 59 (range 39–85) years at the time of operation. Six patients were operated on bilaterally on two or three separate occasions, and 14 patients received multiple joint replacements simultaneously or on separate occasions in up to five joints. Pain was the main indication for surgery in all patients. Four patients (four joints) had hemiarthroplasties, replacing only the distal end of the proximal phalanx. The underlying diagnoses in the patients were degenerative osteoarthritis in 47, post-traumatic or secondary osteoarthritis in eight, and rheumatoid arthritis or psoriasis in 10. Six of the nine men had the operations for secondary osteoarthritis after fractures. Four patients (four joints) were revised due to pain (two) and infection (two), and were excluded from the study. Two patients refused to come for the radiographic and clinical follow-up at 1 year. Three patients refused to come to the hospital for the 5 year follow-up because of long distances, but returned the Disability of the Arm, Shoulder and Hand (DASH) questionnaire/visual analogue scale (VAS) results and had a radiograph at their local hospital.
Surgery
The Ascension® PIP pyrocarbon implant has an anatomical design and a low friction articular surface. The prosthesis is non-cemented and fixed using a press-fit technique. The facilities and two hand therapists responsible for the rehabilitation and evaluation remained unchanged throughout the study. The operations were initially done mainly by one surgeon (PK) and eventually by another three hand surgeons. Surgery was carried out as previously described (Wijk et al., 2010) under general anaesthesia or axillary block and under tourniquet control.
Splinting and mobilization
The first four patients were mobilized in a dynamic splint after 2 weeks. The next five patients were mobilized after 1 week. A rehabilitation protocol was then designed as previously described (Wijk et al., 2010) for the subsequent 56 patients. Mobilization was then started 4–7 days post-operatively with a dynamic splint on the finger that had an extension device and extension block that limited the last 15–20° of extension over the PIP joint. Active flexion exercises were carried out five times a day during the first week of splinting and were intensified to hourly in the following weeks. The dynamic splint was used during the day until the sixth week after operation. The patients then wore a static splint during the night for another 6 weeks.
Assessment
In the first nine consecutive patients the active ROM was measured using a goniometer and radiographs were taken. A follow-up protocol was then designed, and in the next 56 patients an objective and subjective assessment was done prospectively and consecutively. It included radiographs, ROM, grip strength (Jamar dynamometer; Preston Corp, Jackson, Missouri, USA) and recording of pain at rest and activity (using a VAS). Two validated subjective outcome instruments were also added: the Swedish versions of the DASH questionnaire (Gummesson et al., 2003) and Swedish version of the Canadian Occupational Performance Measure (COPM) (CAOT, 2002). Assessments were made pre-operatively and 1, 2, and 5 years after operation. The first nine patients were also assessed using this protocol.
COPM
With the COPM, changes in the patient’s opinion of his or her performance of activities over time can be discovered and analyzed. During the test, the patient defines the five most important activities in their life and where problems occur in the activities. The patient rates the performance and satisfaction in these activities using a scale with one representing “not able” or “not satisfied” and 10 representing “able to do well” or “extremely satisfied.” An individual difference of a minimum of two scale-points between the assessments is considered to be significant (Law et al., 1999).
DASH
The DASH questionnaire evaluates disability and symptoms related to upper-extremity musculoskeletal disorders (Hudak et al., 1996). It consists of 30 questions to score physical activities, symptom severity, and effect of the injury in regards to social activities. The patient’s disability is calculated and the score converted to a scale from 0 to 100, with 0 being the best result.
Radiography
Radiographs were taken in PA and lateral projections post-operatively and at 1, 2, and 5 years. Radiographic analysis was made in the first 21 patients (31 joints) with the prosthesis still in situ, who were due for the 5 year follow-up, to determine the mid-term radiographic outcome. Subsidence of the prosthesis in the proximal and middle phalanges was measured on PA images from the joint surface of the MCP or distal interphalangeal (DIP) joint, respectively, to the end of the stem of the prosthesis. Subsidence was measured as the ratio between the length of the prosthesis and length of the phalanx, expressed as a percentage. In patients with arthrodesis of the DIP joint, the measurement was made from the end of the distal phalanx. The ratio was then translated into millimetres by using the known length of the prosthetic component used.
All implants were scored on lateral images according to Sweets and Stern (2011) to describe the migration of the prosthesis within the medullary canal. Dorsal, palmar, and coronal migration of each implant within the medullary canal were defined using a four-point scale (Figure 1).
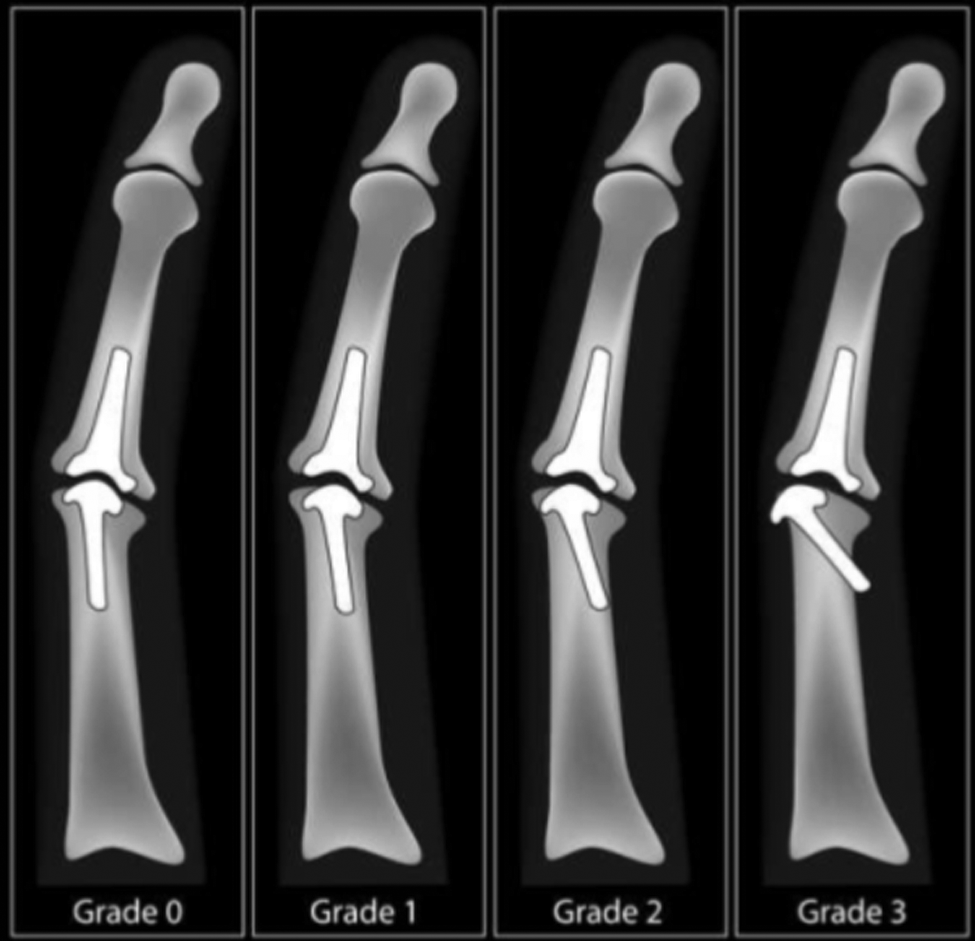
Stern classification of prosthesis position (Sweets and Stern, 2011). Grading of migration of implant within the bone. Grade 0: well-aligned implant; Grade 1: macroscopically evident migration; Grade 2: severe migration with stem opposing cortex; Grade 3: breach of cortex by stem.
Bone reaction and osseous stability
To assess the integration of the prosthesis, we used our own scoring system using PA as well as lateral images. The osseous reaction to the load and stability of the inserted prosthesis were noted and categorized into four grades (Figure 2).
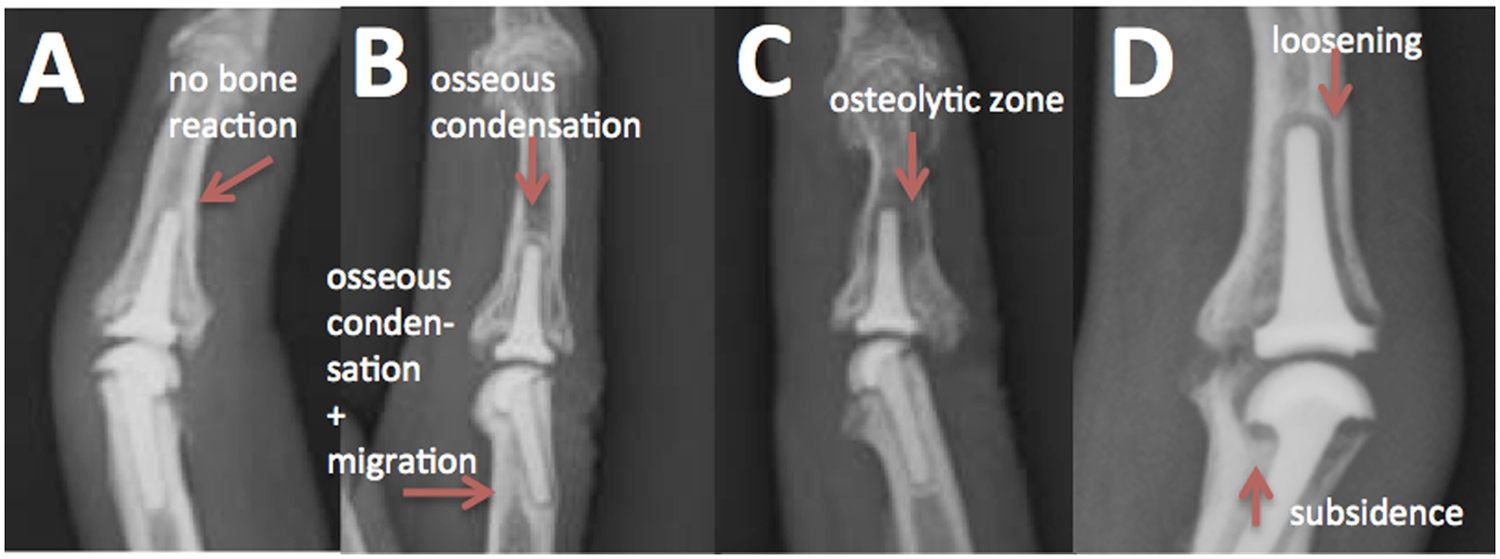
Our own classification of bone reaction around the implant. Bone reaction around the distal component is studied and staged into grades A–D. (A) No or a very limited reaction is seen in the surrounding bone. Immediately post-operatively all prostheses are in grade A. (B) The prosthesis is mechanically integrated and a surrounding osseous condensation has formed around the prosthesis, indicating adaptation by the tissue to the forces transferred from the joint surface to the bone (Anderson et al., 1984; Thomas and Cook, 1985). (C) Local osteolysis is seen around the distal end of the distal implant. This indicates a non-stable situation with a rocking implant causing a local fluid flow that will activate osteoclasts, causing osteolysis.
Statistics
Continuous normally distributed pre- and post-operative data, such as ROM and grip strength, are given as means and standard deviations, and Student’s t-tests were used to test them. For skewed or ordinal data pre- and post-operative data, such as VAS, COPM, and DASH scores, median, ranges, and Wilcoxon’s tests were used. Data are presented as means or medians per finger, but for statistical analysis, multiple measurements were pooled into one single measurement per patient (Sauerland et al., 2003).
Results
During the follow-up period, 10 joints in 10 patients had further operations. Two patients had the prosthesis extracted and a joint arthrodesis because of persisting pain. One patient with rheumatoid arthritis and a previous PIP synovectomy had skin necrosis and infection, and the prosthesis was extracted after 2 weeks. Six months later, a Sutter PIP silicone prosthesis was inserted, which in turn, was later converted into an arthrodesis because of prosthetic breakage. One patient with osteoarthritis had pain and radiographic signs of aseptic loosening and was treated with impaction grafting. Post-operatively, the joint was red and swollen, and an infection was suspected. The prosthesis was removed after 6 months and converted into an arthrodesis. Three patients had limited ROM and had a tenolysis and/or arthrolysis. Another patient had this procedure in combination with a change to smaller prosthetic components due to stiffness and extension defect. Two patients developed hyperextension of the PIP with painful snapping and were treated by a Littler tendonplasty (Littler, 1967), 5 and 16 months after the primary operation. In one of these patients, the components were changed to smaller sizes to improve ROM. In the two patients who had a change of prostheses, the components were radiographically well integrated at the 5 year follow-up.
Objective and subjective results
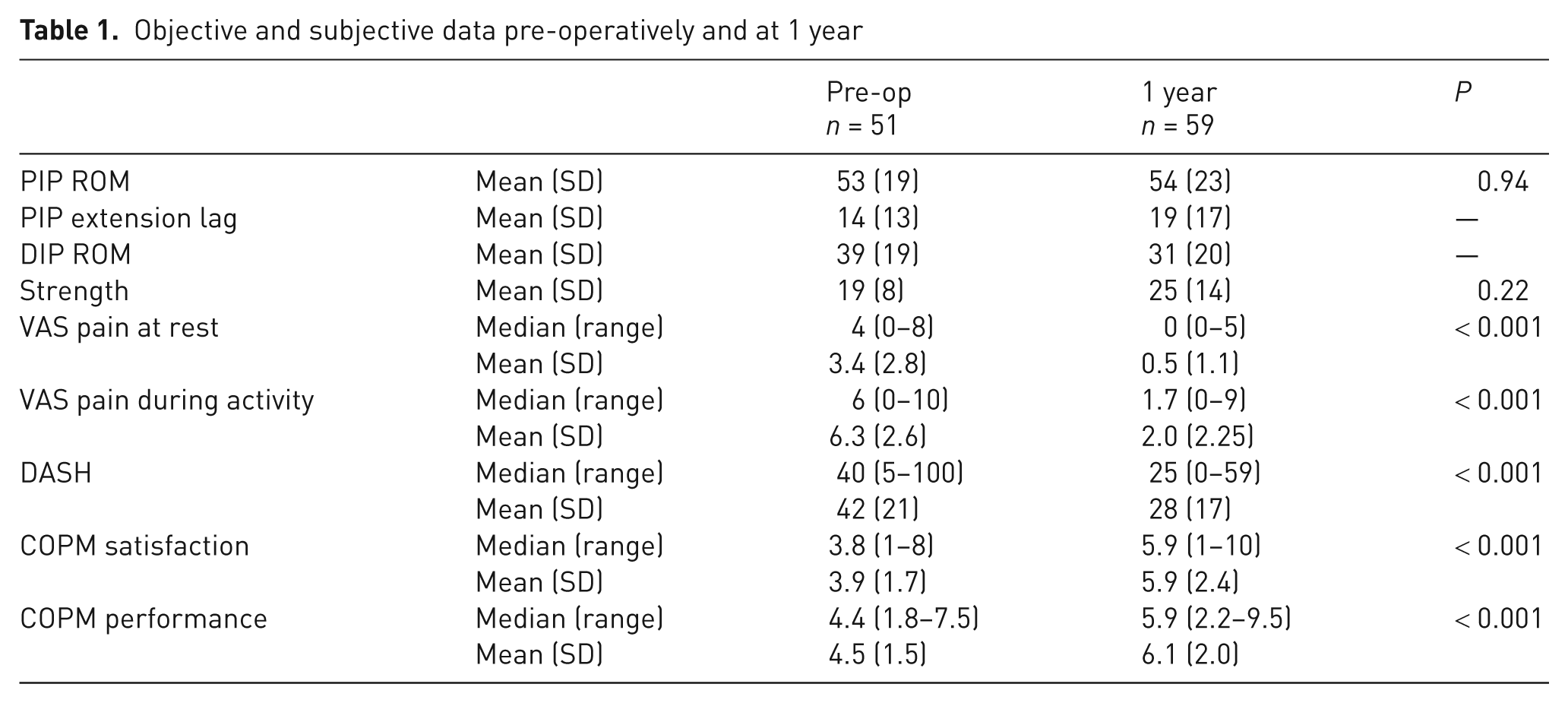
Pain at rest and pain on activity both decreased at 1 year (Table 1). ROM and grip strength did not change from pre-operatively to the 1 year follow-up. Four joints had hyperextension at 1 year, after the change of the rehabilitation protocol.
Objective and subjective data pre-operatively and at 1 year
At the 5 year follow-up, all 21 non-revised patients had a radiograph taken and filled out the DASH and VAS. Twenty of the 21 non-revised patients were free of pain at rest (VAS 0 cm), and 11 of the 21 non-revised patients were free of pain upon activity (VAS 0 cm). The median DASH score was 28 (0–59). In the 18 non-revised patients who came to the 5 year clinical follow-up, ROM of the PIP joint was 54° (SD 29°).
Radiography
The prosthetic position according to the Stern classification changed gradually, with about half of the implants being Stern grade 0 at 1 year without a change in prosthetic position. At 5 years, the prosthetic position had changed in about two-thirds (Stern grade 1), both for the proximal and distal prosthetic component (Figure 3). At 5 years, about 20% were in the Stern grade 2, reaching the cortex, but none were in Stern grade 3, breaching the cortex.
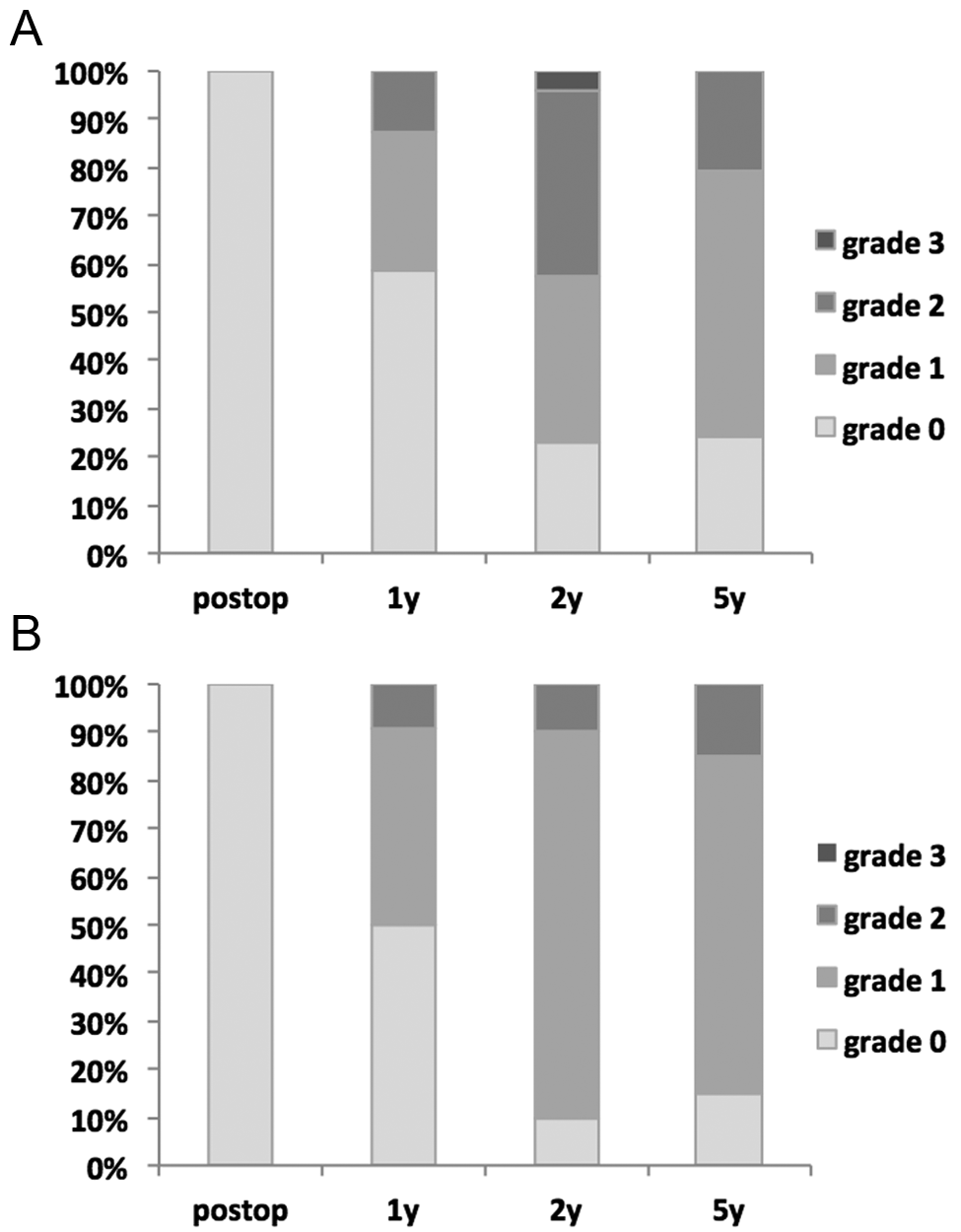
Stern classification at 5 years in the (A) proximal and (B) distal component. Bar charts of the progressive change of implant migration pattern in the 21 patients (31 joints) with the prosthesis still in situ at 5 years.
A bone reaction to the implant was noted over time in the majority, but not all (Figure 4). A surrounding osseous condensation developed in about three-fourths of the prostheses during the 5 years (Figure 5). Also, prostheses showing initial subsidence seemed to be surrounded by an osseous condensation at the final follow-up, as were the prostheses changing position either ulnar/radial or palmar/dorsal directions (Figure 6). Only one joint deteriorated between year 1 and 5 (Figure 7). Seven proximal and 12 distal components showing local osteolytic zones (own classification grade C) or a full surrounding loosening zone (own classification grade D) at 1 year had stabilized and were inert (own classification grade A) or integrated (own classification grade B) at the final follow-up.
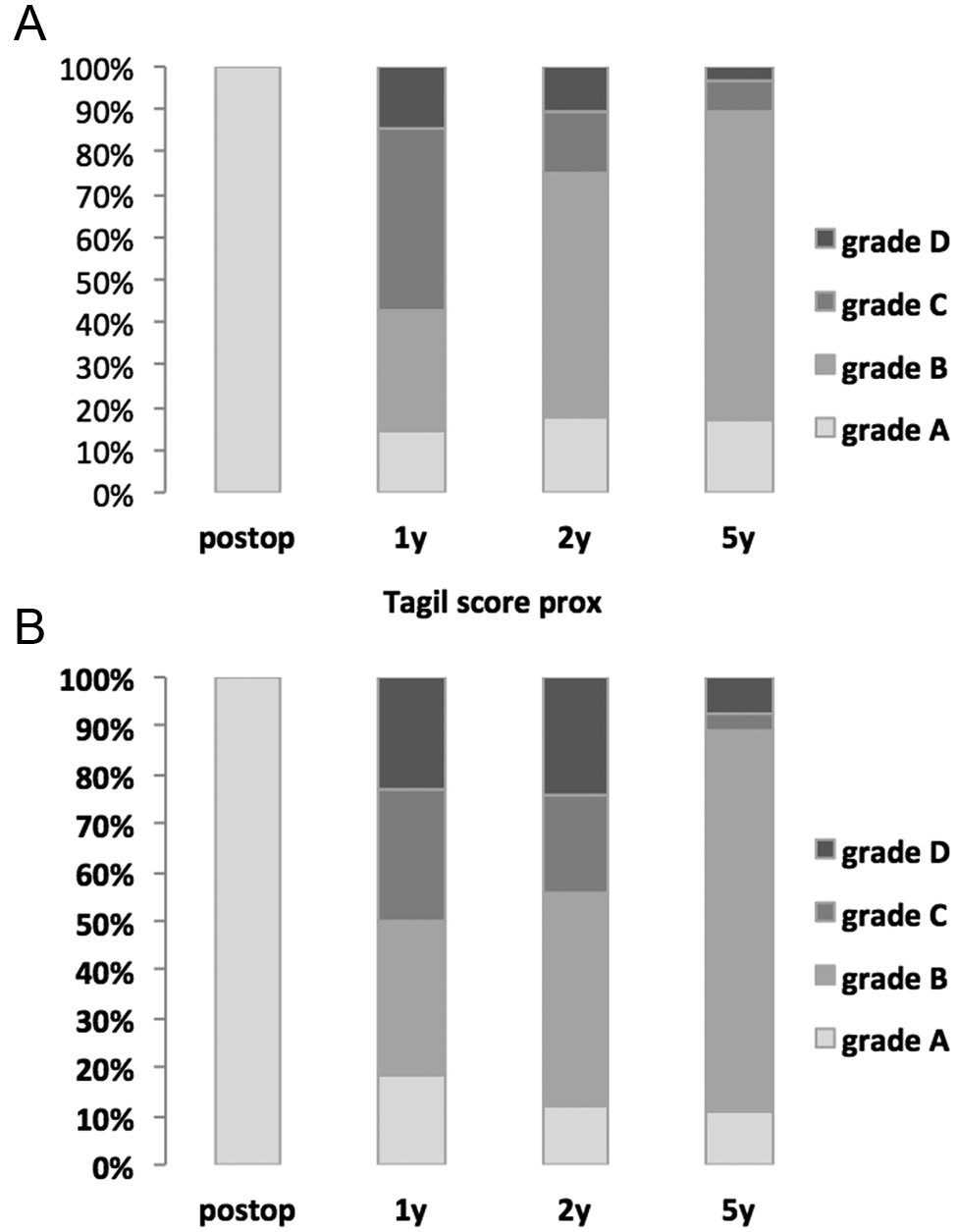
Our classification of bone reaction around the implant in the (A) proximal and (B) distal component plotted over time. As expected, no osseous condensation is found around the prostheses immediately post-operatively (100% grade A). After a year, about a third have stabilized (grade B), and after 5 years, almost all prostheses are surrounded by an osseous condensation indicating relative stability. The prostheses are still, however, capable of migrating within this osseous envelope as seen in the Stern classification (Figures 1 and 2), but this involves a slow remodelling process.
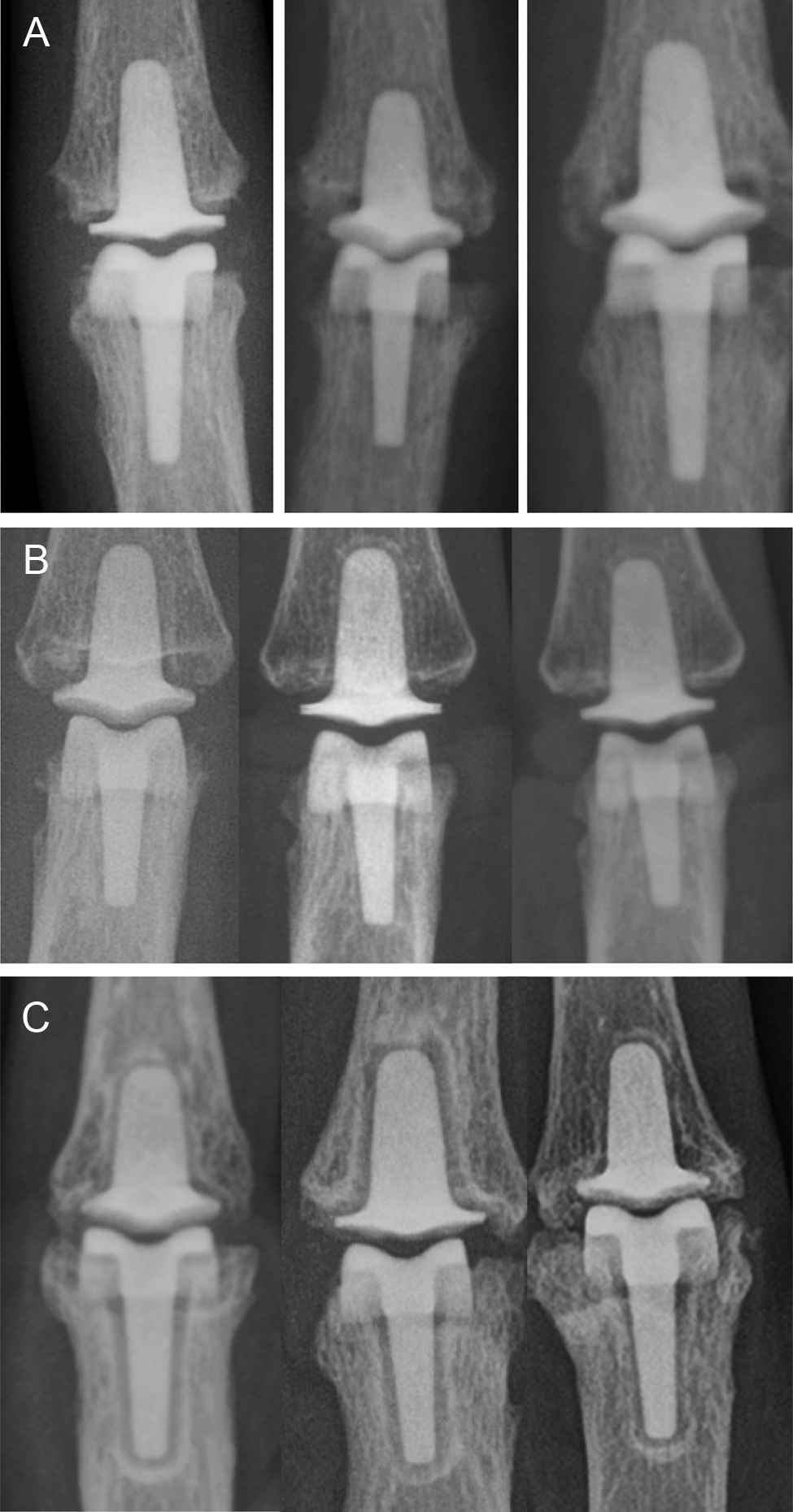
Varying osseous reactions over time in three joints. In (A), as expected, no osseous reaction is seen in the post-operative radiographs. In (B), there is still no osseous reaction after 5 years. In (C), also after 5 years, distinct osseous condensation lines surround both components in all three patients.
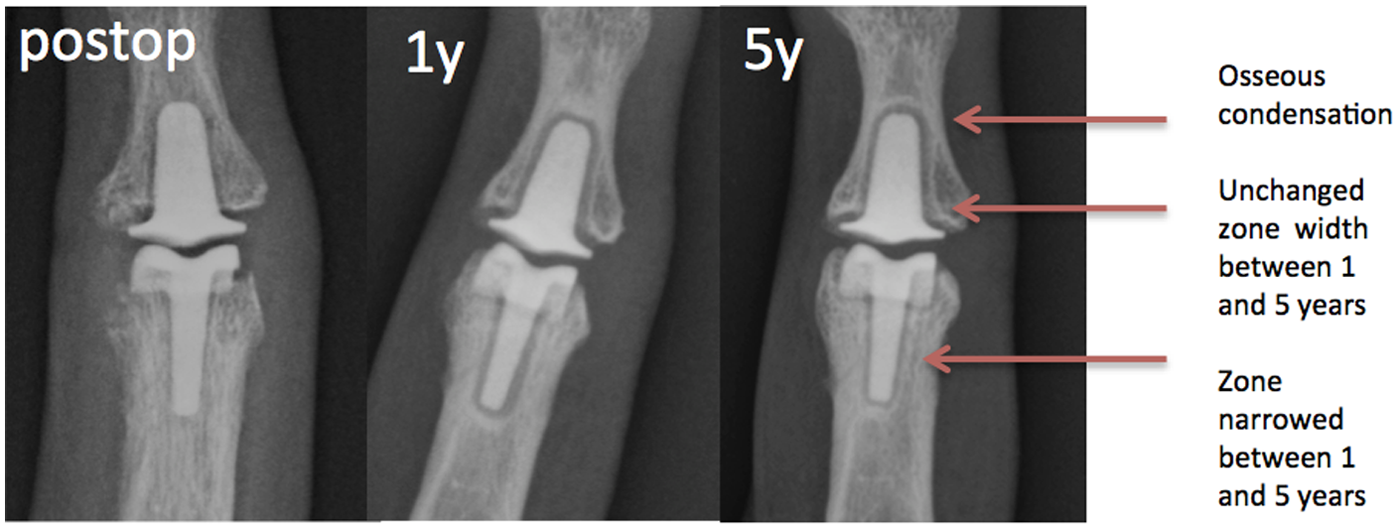
PIP prosthesis post-operatively and at 1 and 5 years as an example of biological stabilization over time. (A) As expected, immediately post-operatively no zone and no ossification can be seen, and the prosthetic components rest on the cancellous bone. (B) At 1 year, zones can be seen around both components representing a fibrous tissue membrane. (C) After 5 years, the zone around the proximal component has decreased in size, but no ossification line is visible, in contrast to the distal component where the loosening zone remains.

PIP prosthesis post-operatively, at 1, 2, and 5 years showing radiographic deterioration, the only one at the 5 year follow-up. After a possibly suboptimal post- operative bone contact, a shift in the prosthetic position can be seen as the proximal component goes into extension (Stern classification grade 2). The shift is slow, as seen by the surrounding bone envelope indicating some stability (our classification grade B, Stern grade 2) at 1 year. At 2 years, a local osteolysis has developed at the tip of the prosthesis (our classification grade C, Stern 2), and in time, penetration of the cortex might appear.
The proximal prosthetic components subsided up to 7 % of the length of the phalanx, and four prostheses subsided more than 1 mm (1.0, 1.2, 1.4, and 2.0 mm). All measurable subsidence took place in the first 2 years, whereas no component migrated more than 1 mm between year 2 and 5. Three proximal prostheses had osteolytic zones at the 5 year follow-up. The distal prosthetic components subsided up to 8% of the length of the phalanx. Three prostheses subsided more than 1 mm (1.0, 1.1, and 1.3 mm), all in the same patient and all stabilized between 2 and 5 years. One of these joints fused spontaneously. Three distal prostheses had osteolytic zones at the 5 year follow-up.
Discussion
In the present series of 65 patients (89 joints) treated from 2001 to 2010, the rate of re-operation was 10/89 joints. In the first 24 patients (34 joints) with 5 years follow-up, the rate of re-operations was higher (7/34 joints) and only three re-operations were done in the last 55 joints. This could indicate an initial learning curve, but there are also potential risks of future failures as others have reported late revisions due to subsidence, malposition, or pain (Sweets and Stern, 2011). In the present series, however, all re-operations occurred within the first 2 years after operation. The first two re-operated patients had slowly developing hyperextension, which made us change the post-operative rehabilitation protocol after nine patients (Wijk et al., 2010). The protocol appears to be effective, as after the change only four of 74 joints in total had hyperextension at the 1 year follow-up. In the patients followed for 5 years, only one joint showed deterioration in the radiographic appearance between the 1 and 5 year follow-up. The two patients who were re-operated and had their components simply changed to smaller sizes did not show any radiographic signs of deteriorating prosthetic position, osteolytic zones, or subsidence at the 5 year follow-up. There are no pending revisions. Heers et al. (2013) followed 13 joints in 10 patients for 6 to 9 years, and two joints were re-operated due to stiffness. In spite of the presence of radiolucent lines and zones in half the joints, as well as prosthetic migration in four joints, no revisions were made due to loosening. Watts et al. (2012) reported a revision rate of 15 out of 89 patients after a mean of 5 years, with revisions occurring mainly during the first 2 years; this similar to our findings (10/89). Others have reported a higher incidence of revisions at a mean of 5 years (6/31; Sweets and Stern, 2011), including not only early but also late revisions. With shorter term follow-up, the revision rate varies between 0% to 40% after 1 to 3 years (Bravo et al., 2007; Daecke et al., 2012; Herren et al., 2006; Mashadi et al., 2012; McGuire et al., 2012; Meieret al., 2007; Nunley et al., 2006; Petscavage et al., 2011; Sweets and Stern, 2011). The rates are difficult to interpret, as the indications for revision differ between centres.
Pain is the major indication for almost every osteoarthritic joint procedure. The clinical result in this series, with complete pain relief at rest in 47/59 non-revised patients attending the 1 year follow-up, must be considered good but also durable, with 19/21 non-revised patients still pain free at rest after 5 years. Arthrodesis has been suggested as a safer alternative to prosthetic arthroplasty (Sweets and Stern, 2011). It would be equally successful in substantially reducing the pain, although to our knowledge there have been no reports in recent years of PIP arthrodesis as a primary operation. Although pain is the main indication for surgery, the overall function is probably better when pain-free motion is retained in the PIP joint.
To assess the results of surgery at a more detailed level than simply recording pain, ROM, and revision/re-operation rates, two function scores were added: COPM and DASH. In the first nine patients, DASH and COPM were not recorded pre-operatively, and therefore a comparison between pre- and post-operative data is not possible at the 5 year follow-up. In the subsequent 56 patients, the occupational performance at 1 year, measured by COPM, had improved from the pre-operative level by more than the two scale-steps suggested to be clinically relevant by the designers of the COPM outcome instrument (Law et al., 1999). This indicates that tasks considered important by the patient were improved. Also, the DASH score at 1 year had improved substantially from a median of 40 to 25 in all patients.
Pyrocarbon is a material which, in contrast to steel, titanium, and polyethylene, has not been used extensively in orthopaedics and hand surgery, and the experience of tissue reaction to pyrocarbon over a longer time is limited. It has been suggested that the isoelasticity of pyrocarbon relative to bone might be of advantage (Cook et al., 1981). Due to the isoelasticity, limited shear forces and micromotion will occur between the bone tissue and prosthesis on loading or in flexion and extension, as they will theoretically deform identically. Remodelling will take place in the bone surrounding the prosthesis as a response to the mechanical load (Figures 4–6). Due to the loading pattern and remodelling stimuli, the prosthesis might rotate very slowly over time and flex or extend within the phalanx, as described by Sweets and Stern (2011). This could lead to cysts or a fibrous membrane surrounding the whole prosthesis and lead to increased subsidence, as shown in animal studies comparing pyrocarbon and metal prostheses (Daecke et al., 2006). However, the prosthesis might stabilize, as we saw in our radiographic analysis, and the remodelling could then lead to equilibrium between bone formation and resorption, seen as an osseous condensation surrounding the prosthesis (Figure 5). Perhaps the pyrocarbon simply behaves in a different way from a steel prosthesis, due to the modulus of elasticity. The initial radiolucency surrounding the prosthesis is difficult to interpret. Because these radiolucency lines have led to a fear of progressive bone resorption, some authors have done early revisions and have revision rates up to almost 40% in the first years (Daecke et al., 2012). In our series, only one joint (Figure 6) showed progressive loosening, whereas in the majority (seven distal and 12 proximal components) the zone was inert or decreased between the 2nd and 5th year.
Patients were content with the results and we believe that the prosthesis is a step towards improved treatment of pain in PIP osteoarthritis. Based on our results, patients can expect a good outcome from the operation regarding pain relief, but should not expect increased ROM. Similar conclusions were drawn in another mid-term study (Watts et al., 2012). Other centres have raised concerns, with worse results and higher revision rates as well as a decreased ROM with time (Sweets and Stern, 2011). As seen in the present study, there is an initial learning curve in the use of this prosthesis. This type of surgery is probably better done in centres where there is a higher volume and cumulative experience of these techniques. Randomized studies are needed before we can say that prosthetic replacement is better than arthrodesis or other kinds of arthroplasties, or in comparison with the natural course of PIP osteoarthritis.
Footnotes
Acknowledgements
The authors thank occupational therapists Ulrika Wijk B.S. and Margareta Wollmark B.S. for reviewing the patients. The project was supported by the Swedish Research Council (project 2031), Greta and Johan Kock, Alfred Österlund, Maggie Stephens, Thure Carlsson foundations, and the Medical Faculty of Lund.
Conflict of interests
P. Kopylov and M. Tägil are consultants and design surgeons for the implant manufacturer. No other conflicts declared.
Funding
The project was supported by the Swedish Research Council (project 2031), Greta and Johan Kock, Alfred Österlund, Maggie Stephens, Thure Carlsson foundations, and the Medical Faculty of Lund.