
Abstract
Both open and endoscopic methods for ulnar nerve decompression have been described. The purpose of this study is to compare the 6-month results of a minimal invasive open technique with an endoscopic technique. We treated 60 patients with unilateral ulnar neuropathy at the elbow, employing both techniques. Six months postoperative we found no differences in treatment effect on pain and disability scores between both groups, but both techniques resulted in an early postoperative relief of symptoms and good patient satisfaction.
Introduction
Cubital tunnel syndrome is encountered with a frequency second only to carpal tunnel syndrome in the diagnosis of upper extremity peripheral nerve entrapment syndromes (Bartels et al., 1998). Patients with cubital tunnel syndrome classically present with an ache along the medial side of the proximal forearm, tenderness along the posterior groove to the medial epicondyle, dysesthesia, hypesthesia, anesthesia, muscle atrophy and/or motor dysfunction in the distribution of the ulnar nerve.
The cause of complaints from cubital tunnel syndrome is thought to be an entrapment of the ulnar nerve at the level of the elbow. The entrapment can be owing to an associated pathology, but the most common presentation is compression at any of several sites without specific pathology. Common areas of compression include the arcade of Struthers, the medial intermuscular septum, the medial epicondyle, a narrow cubital tunnel, Osborne’s ligament and the flexor carpi ulnaris fascia (Hoffmann and Siemionow, 2006).
The non-operative approach (i.e. rest, splinting, physical therapy) is usually offered as the first option of treatment in patients presenting with mild symptoms (Dellon score 1). When conservative therapy failed, or when patients present with severe symptoms (Dellon score 2 and higher), surgical decompression of the ulnar nerve is indicated (Assmus et al., 2009).
Both open and endoscopic methods for ulnar nerve decompression have been described. The current methods of surgical decompression are simple decompression, medial epicondylectomy or transposition of the ulnar nerve into the subcutaneous or submuscular plane (Novak and Mackinnon, 2009).
Until some years ago, most authors recommended an open procedure for ulnar nerve release at the elbow, making an incision of at least 10 cm. The result is a long scar and potentially a great risk of injury to the posterior branch of the medial antebrachial cutaneous nerve (Ahcan and Zorman, 2007).
The most recent surgical option is the endoscopic release. Contrary to the previous open release, an endoscopic release only needs a much shorter incision, with theoretical lower risk of damaging the posterior branch of the medial antebrachial cutaneous nerve and less extensive and especially no circular dissection of the ulnar nerve. This less radical dissection often leads to a more rapid recovery (Bain and Bajhau, 2005; Watts and Bain, 2009).
The purpose of this study is to compare the 6-month results of a minimal incision invasive open technique with the endoscopic technique described by Hoffmann and Siemionow (2006) (Hoffmann technique).
Methods
From October 2007 to April 2011 we treated 60 patients with unilateral ulnar neuropathy at the elbow, employing the Hoffmann endoscopic technique or an open minimal invasive technique, using an illuminated speculum. All patients gave informed consent for participation in this study.
The inclusion criteria were minimum age of 18 years, no previous surgery in the area of the elbow and primary idiopathic ulnar nerve entrapment syndrome.
The diagnosis was based on history and clinical examination, i.e. positive Tinel’s sign, sensory loss in the area innervated by the ulnar nerve, pain over the medial epicondyle, weakness of the muscles innervated by the ulnar nerve and a positive elbow flexion test. For each patient electrophysiological data were collected.
Patients were classified according to Dellon’s scale of severity symptoms (Dellon, 1989), as grade I (intermittent sensory symptoms, subjective motor symptoms, no muscle atrophy), grade II (intermittent sensory symptoms, objective weakness in pinch and/or grip strength, no muscle atrophy) and grade III (persistent sensory symptoms, objective weakness in pinch and/or grip strength, presence of muscle atrophy).
Surgical technique
We operated at two different departments of our hospital. At one department we used a 30° endoscope following the Hoffmann technique. At the other department we operated using an illuminated speculum. All operations were performed by one surgeon, who had two years of experience with both of the techniques.
Under an axillary block or general anesthesia with a high arm tourniquet the arms were operated upon on an arm board. A total of 32 operations were performed following the Hoffmann technique, using a tunneling forceps, an illuminated speculum and an endoscope. The ulnar nerve was released for at least 10 cm both proximally and distally; i.e. 20 cm in total.
In 28 patients we performed a minimally invasive technique using an illuminated speculum. A 2,5 cm longitudinal incision was made midway between the medial epicondyle and the olecranon. The subcutaneous tissue was dissected bluntly down to the fascia of the forearm. The fascia over the ulnar nerve was released distally with the use of tunnelling forceps. The ulnar nerve was released 12 cm both proximally and distally, i.e. 24 cm in total. All operations were completed successfully with no need to convert to a larger incision.
The postoperative plan was the same with initial support with a bulky dressing and mobilization with therapy support from 10 days.
Assessments
The objective assessments incision length, duration of tourniquet control and length of decompression were measured during operation. With respect to the subjective assessments, patients were asked to complete the DASH (disability of arm shoulder and hand) questionnaire just before surgery and approximately 6 months after surgery (0 points reflect minimal disability and 100 points reflect maximal disability). The Bishop rating system was used 6 months postoperatively. The Bishop score is defined as poor (0–2), fair (3–4), good (5–7) and excellent (8–9). Pre- and postoperative pain and patient satisfaction were evaluated by using a visual analogue scale (VAS)-scale (0–10).
Statistical analysis
A comparison of numerical and binary baseline characteristics between the patients from the two departments was performed with the two-sided t-test with unequal variances and Pearson’s chi-square statistic, respectively. A random intercept model for patients was applied to the longitudinal data of DASH and VAS to investigate the effect of each treatment separately and to investigate a difference in its possible effect between treatments. The effect of treatment was quantified by the inclusion of the covariate time to follow-up (in months) and the difference in treatment effect was estimated by the interaction effect of treatment and time. The type III tests were used since these analyses were corrected for age, gender, duration of complaint and department.
The research protocol was approved by the local ethical committee of the Medical Spectrum Twente, the Netherlands.
Results
Twelve patients in the endoscopic group and six patients in the speculum group were lost to follow-up. The reasons were moving to another city, illness, death and unwillingness to fill in the postoperative questionnaire. Thus there were 20 patients included in the endoscopic group and 22 patients included in the speculum group. One patient from the speculum group had postoperative recurrent symptoms and was operated again (but only the first measurements were used in the statistical analysis). The patients’ characteristics and operation characteristics can be found in Tables 1 and 2, respectively.
Patients characteristics for both treatments.
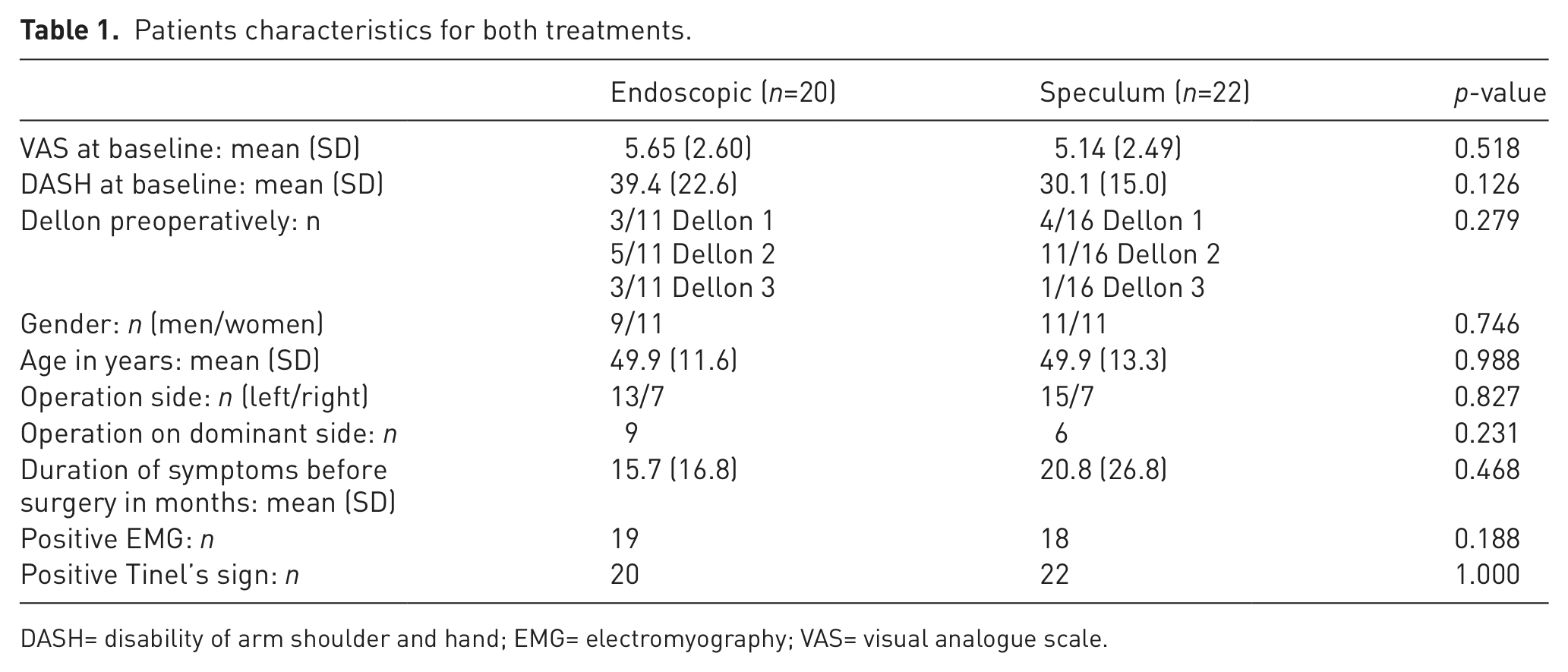
DASH= disability of arm shoulder and hand; EMG= electromyography; VAS= visual analogue scale.
Operation characteristics for both treatments.
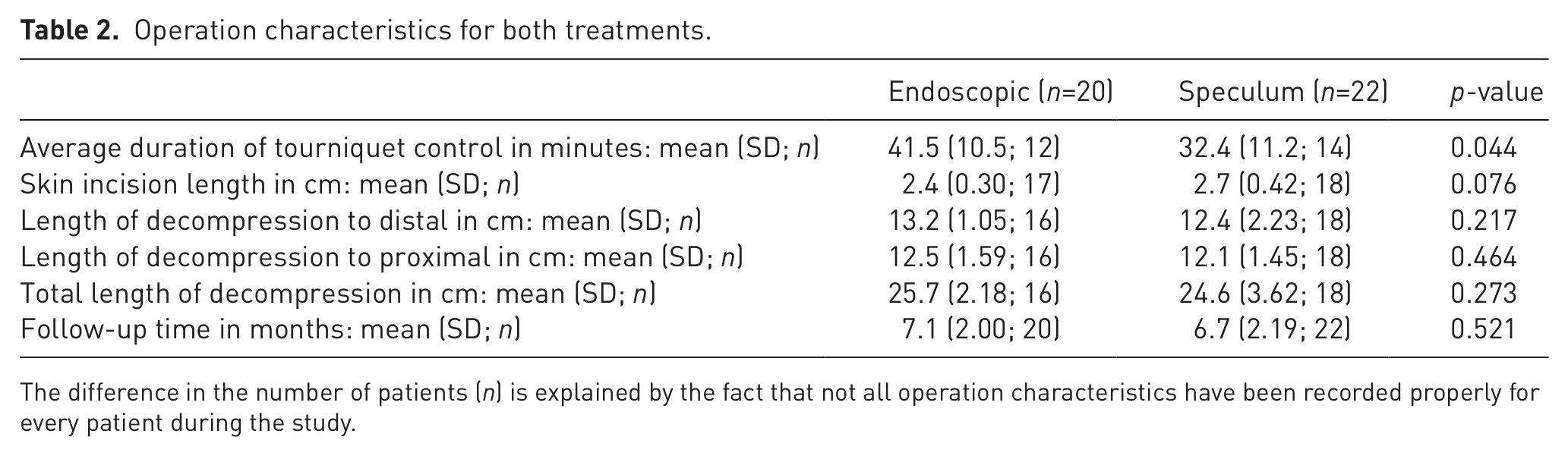
The difference in the number of patients (n) is explained by the fact that not all operation characteristics have been recorded properly for every patient during the study.
Objective assessments
There are no significant differences between the two treatment groups for patient characteristics and skin incision length, except for an average duration of tourniquet control, which was 9 minutes lower for the minimal invasive treatment.
Subjective assessments
There was no statistical difference between the speculum and endoscopic treatment for the changes in pain score (p=0.752) and the disability score (p=0.737) (Table 3). Both treatments demonstrated significant changes in VAS (p<0.001) and DASH (p<0.001). The pain score dropped with approximately three points and the disability score reduced by approximately 15 points. Postoperatively, patients were asked if they were satisfied with the result of the operation. Satisfaction was 80% in the endoscopic group and 86 % in the speculum group. An excellent or good result on the Bishop Scale, 6 months postoperatively was scored by 91% of the endoscopic group and 93% of the speculum group (see Table 3).
Characteristics after follow-up for both treatments.
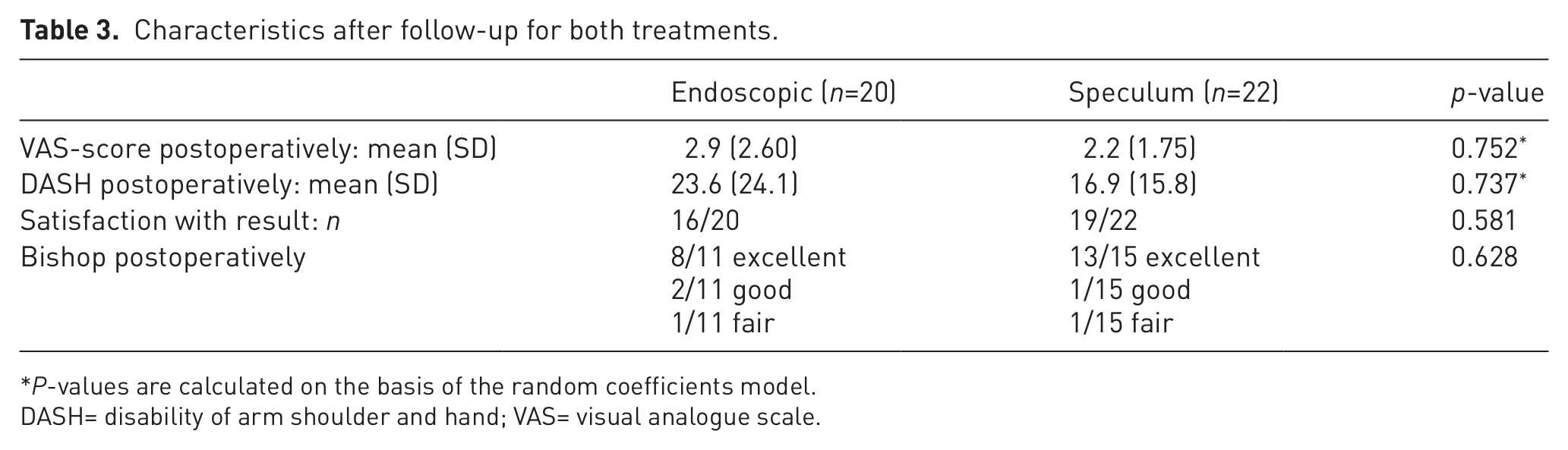
P-values are calculated on the basis of the random coefficients model.
DASH= disability of arm shoulder and hand; VAS= visual analogue scale.
Complications
There was one postoperative wound infection in the endoscopic group, which was successfully treated with antibiotics.
Discussion
Until some years ago, most authors recommended an open procedure for ulnar nerve release at the elbow. Recently, minimal invasive techniques to decompress the ulnar nerve are described. The principle of a minimally invasive approach is similar to an in situ decompression, where the nerve is completely decompressed, but through a smaller incision. The handling of the nerve and surrounding tissue dissection is kept to a minimum (Karthik et al., 2012).
Recent articles by Lequint et al. (2013) and Konishiike et al. (2011) describe the advantages of a minimal invasive open approach without and with endoscopic assistance, respectively. In their studies they also transpose the nerve, which we believe unnecessarily reduces blood supply to the nerve (however they claim not to) and creates a larger wound surface. Ochi et al. (2013) stated that simple decompression, without transposition of the nerve, is the favourable surgical procedure for cubital tunnel syndrome in terms of decompression and reduction of strain in the ulnar nerve.
The endoscopic approach to the cubital tunnel syndrome was introduced as a minimally invasive alternative for decompression of the ulnar nerve at the elbow, aiming to minimize the trauma to the tissues and improve postoperative recovery of the patients, with an even longer decompression of the ulnar nerve. Its theoretical advantages over the classical open approach are the faster recovery of the patient, decreased invasiveness, minimal vascular complications and less scar discomfort (Ahcan and Zorman, 2007).
The use of the endoscopic technique for decompression of the ulnar nerve at the elbow started in 1999 by Tsai et al. Since then, several techniques have been described, however, there is no standard in the method of the technique itself, and each surgeon usually develops his/her own approach for the endoscopic procedure (Flores, 2010).
In this study we compared a minimal invasive open technique with the endoscopic Hoffmann technique. The basic steps of the procedure are the same in both techniques. In the minimal invasive technique a pocket is built in the subcutaneous tissue over the fascia with tunnelling forceps. An illuminated speculum, held by an assistant, is essential to pull the skin and subcutaneous tissue off the fascia. The fascia over the ulnar nerve is released under direct vision with the use of a pair of long scissors, as in the endoscopic technique.
After evaluating the results of both techniques, we did not see significant differences in the pain score, disability score, treatment satisfaction and the Bishop scale between both treatment groups. However, sample sizes are small, which means that the power may be too limited to detect clinically relevant differences.
A significant difference in operational characteristics between both groups is the average duration of tourniquet control: 41.5 minutes in the endoscopic group and 32.4 minutes in the speculum group. This implicates that the total operation time is shorter in the speculum group. This technique is also more cost-effective, because it does not need an endoscope.
There are significant weaknesses in this study. We did not randomize patients. We operated at two different departments of our hospital. At only one department we had access to a 30° endoscope, necessary for the Hoffmann technique. Patients presenting to that department were therefore automatically operated endoscopically. The baseline characteristics, however, do not suggest a significant difference between the two groups of patients. The number of patients enrolled in the study is not very large. We were dependent on the patients that were available in the 3.5 years that the study was run. The numbers are, however, similar to other studies. There was also a significant loss of patients from this study. The sample size was sufficient to demonstrate a positive effect of both methods with similar improvement of the patients’ symptoms, even though it might be too small to detect a significant difference between both treatments.
The strengths of the study are that all patients were operated by one surgeon. We made a comparison between two, almost similar techniques. Both techniques are new and have not been compared with each other before. The good results as to relief of symptoms of both techniques compared with the former standard technique show that both techniques are valid alternatives. Advantages lie in quick recovery and high patient satisfaction.
In conclusion, the minimally invasive and endoscopic techniques seem to give comparable results, although a larger randomized controlled study would be needed to reliably show this.
Footnotes
Conflict of interests
None declared.
Ethical approval
Our research protocol was approved by the local ethical committee of the Medical Spectrum Twente, the Netherlands.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.