
Abstract
In 1910, Georg Preiser (1876–1913) described five cases of rarifying osteitis. Based on his imaging studies, he diagnosed post-traumatic avascular necrosis (AVN) of the scaphoid without any sign of primary fracture. This was followed by an article in 1911 in which Preiser related his findings to Kienböck’s disease and Köhler’s disease of the tarsal navicular. Upon searching the literature, we found descriptions and discussions of Preiser’s imaging; however, the original images have never been published. We reproduce Preiser’s original imaging in this current review. All of these appear to show a fracture and no signs of AVN, suggesting that Georg Preiser misinterpreted his findings. There is no apparent uniformity in the literature regarding the definition, description, or aetiology of Preiser’s disease, and it is for this reason that we find the use of eponyms to be confusing.
Keywords
Introduction
More than a hundred years ago, Georg Preiser (1876–1913) proved to be far ahead of his time by visualising the vascular supply of the scaphoid bone using vascular injection and radiographic imaging. He reported post-traumatic avascular necrosis (AVN) of the scaphoid without primary fracture (Preiser 1910). Preiser’s disease has been studied and discussed ever since. We found his 1910 article and believe it to be the first time—after Preiser published them himself—that these original images have been published. Upon analysing these images, we found pathology suggesting primary fracture, and for this reason, propose that Georg Preiser misinterpreted his findings.
History and imaging
Georg Karl Felix Preiser was an orthopaedic surgeon from Hamburg. In 1910 he published the article, “Eine typische posttraumatische und zur Spontanfraktur fuhrende ostitis des naviculare carpi”, in the German journal Fortschritte auf dem Gebiete der Röntgenstrahlen. Preiser described 24 cases of fracture of the scaphoid; however, in five of his patients Preiser found the radiographs to be significantly different. He suggested post-traumatic AVN of the scaphoid without any sign of primary fracture. Preiser described his theory of ligament rupture, followed by blood vessel rupture, bone weakening, osteoporosis, sclerosis, and ultimately, fracture (Preiser 1910; 1911).
Preiser was interested in the anatomy and vascularisation of bone in general, and of the scaphoid in particular, and used injection techniques and radiographs to visualise its blood supply for the first time. However, Preiser was dissatisfied with his imaging and asked his friend, the more experienced surgeon Erich Lexer (1867–1937), to help him inject cadavers and create images of the scaphoid bone. Together they managed to visualise the vascularisation of the scaphoid and its apparent pathology. Preiser stated that the pathology seen in these particular cases was necrosis of the scaphoid bone. He said, “Grade dieser Fall ist absolut beweisend, dass sich die Ostitis auch ohne primäre Fraktur, bezw. Infraktion ei nstellt.” (“Especially this case proves absolutely that ostitis occurs without primary fracture or (alternatively) infraction”) (Preiser 1910).
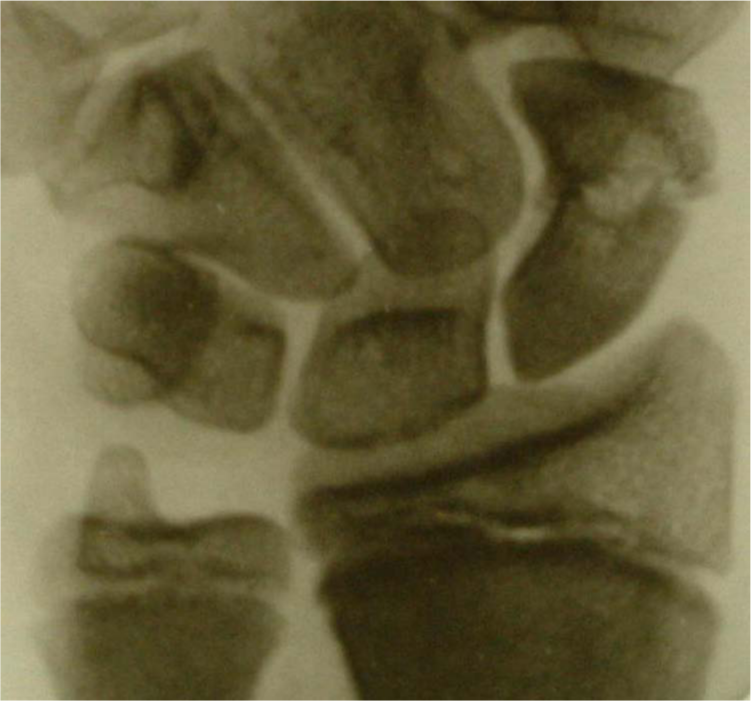
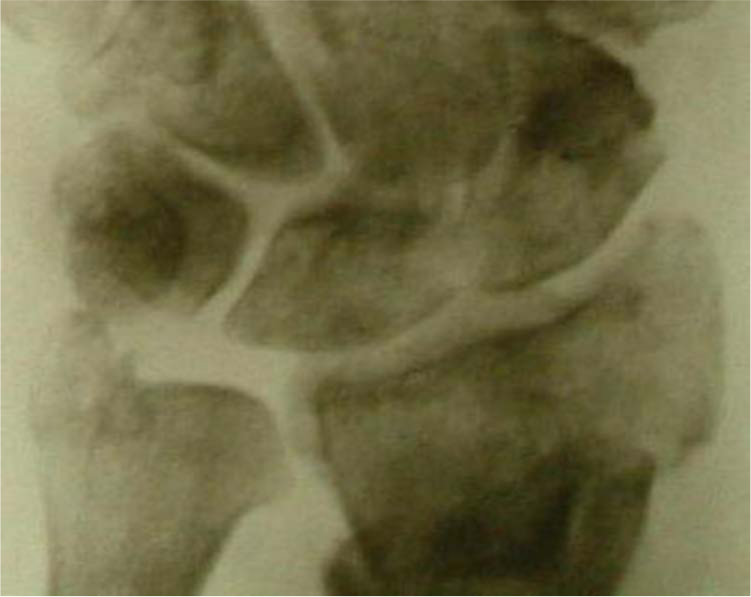
Based on the findings of his radiographic imaging with intravascular contrast, Preiser explained the vascularisation of the scaphoid in great detail. He found that the radial artery entered the bone through its dorsal surface and provided most of the blood supply to the scaphoid. He also described other small branches that arose from an anastomosis between the radial and interosseous arteries, and joined the main supply in the dorsum of the scaphoid. The original radiographs published by Preiser show a few small branches entering the tuberosity as well as a main central vessel at the waist of the scaphoid (Figures 1a,b) (Preiser 1910).
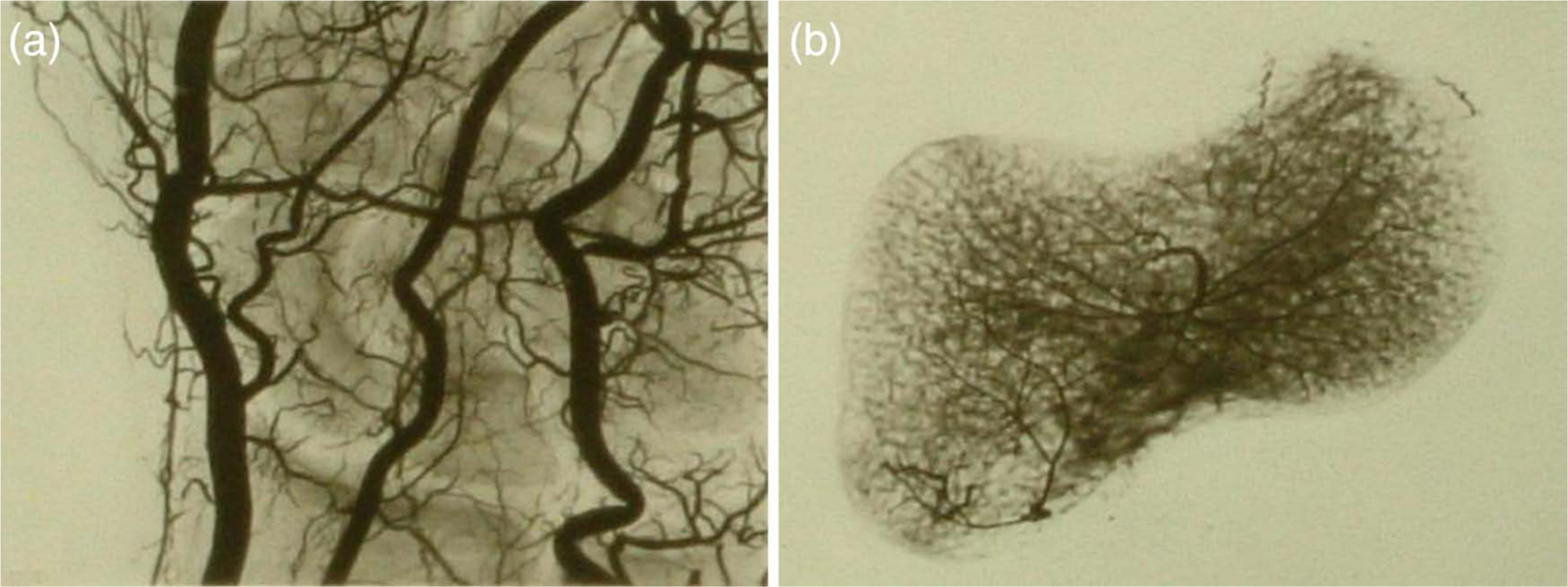
(a) Vascularisation of the wrist and (b) vascularisation of the scaphoid.
In his second article published in 1911, “Zur Frage der typischen traumatischen Ernährungsstörungen der kurzen Hand- und Fusswurzelknochen”, Preiser argued with a Dr. Haenish, who concluded that a fracture line was present in the images of the scaphoid. However, Preiser was certain this was not the case. He stated, “die Hauptsache müsse eine Gefäss- bezw. Ernährungsstörung sein!.” (“the main issue had to be a vascular problem or (alternatively) or a problem of supply (nourishment)!”) (Preiser, 1911).
A few months previous to the 1911 article, the Viennese radiologist Robert Kienböck had published an article describing the process of lunatomalacia, supported by evidence of radiological changes and clinical symptoms (Peltier, 1980). Preiser related his own findings to Kienböck’s lunatomalacia, and also to the comparable Köhler’s disease of the tarsal navicular. Furthermore, he pointed out that Kienböck had accepted his (Preiser’s) theory about ligament rupture ultimately leading to fracture. He suggested this type of disease should be called Traumatische Ernährungsstörungen der kurzen Hand- und Fusswurzelknochen (Traumatic supply problems of the short carpal and tarsal bones) (Preiser, 1911).
Preiser’s cases
Here we summarise the key descriptions from Preiser’s data on history, physical examination, and his imaging, followed by our interpretations of these radiographic images.
Case 1
A 30-year-old male who had fallen on his right wrist 6 months earlier was complaining of wrist pain during heavy work. Physical examination showed a slight increase in wrist diameter and slightly diminished range of motion. The first radiograph was taken 7 months after the injury (Figure 2a). Preiser interpreted the central hypodense area in the scaphoid as necrosis without fracture. The second radiograph (Figure 2b) was taken 15 months after trauma and shows a waist fracture of the scaphoid, which Preiser believed was secondary to necrosis. We believe both radiographs (Figures 2a,b) show a central waist fracture with signs of cyst formation.
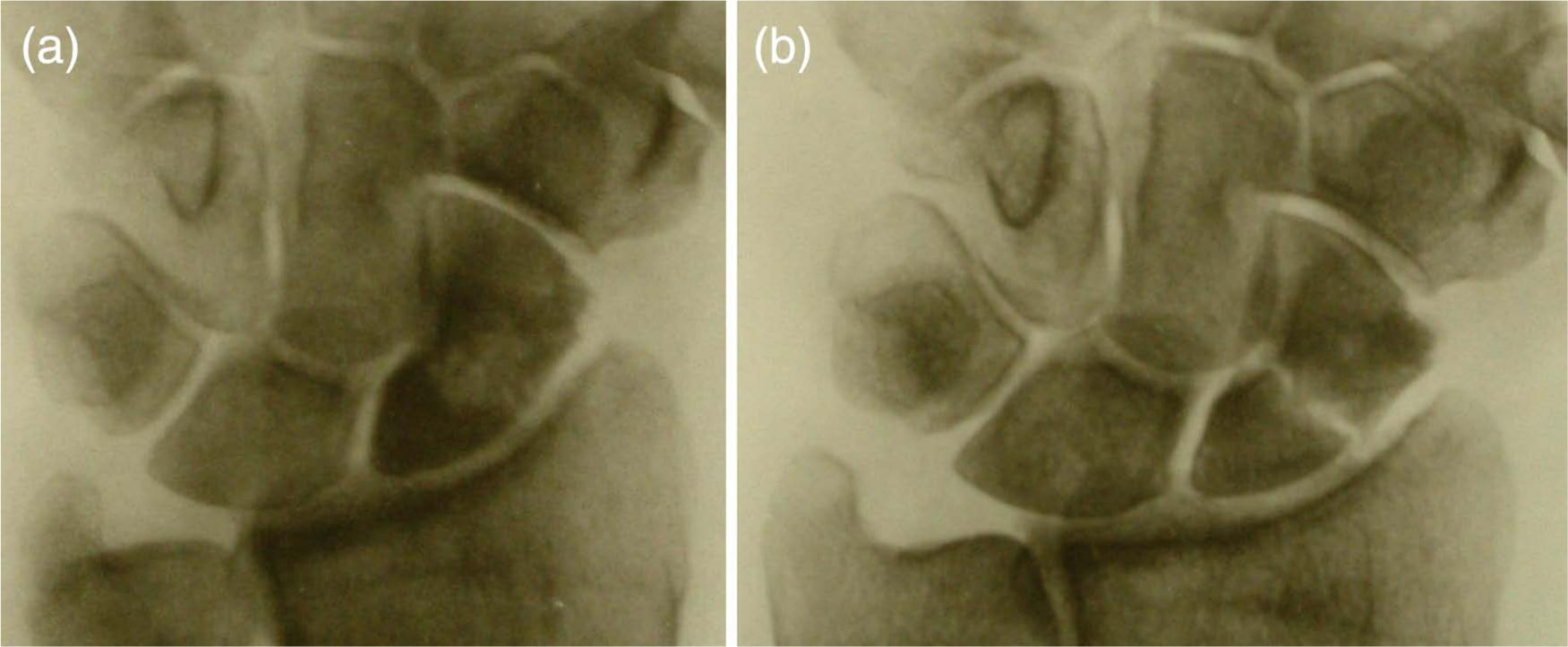
(a) First radiograph taken, seven months after trauma and (b) second radiograph taken, fifteen months after trauma.
Case 2
A 32-year-old male fell on his left hand 3 months prior to presentation. On physical examination he complained of pain on motion. Extension, ulnar, and radial deviation. The first radiograph, taken 3 months post-trauma, was felt to show an avulsion fracture of the radial side of the scaphoid (Figure 3a). He suggested this was the result of a fall on the hand in ulnar flexion and tension on the collateral radial ligament. He describes a central hypodensity—in his opinion, secondary to necrosis. On the second radiograph taken 8 months after trauma he described a secondary oblique fracture through the waist of the scaphoid (Figure 3b).
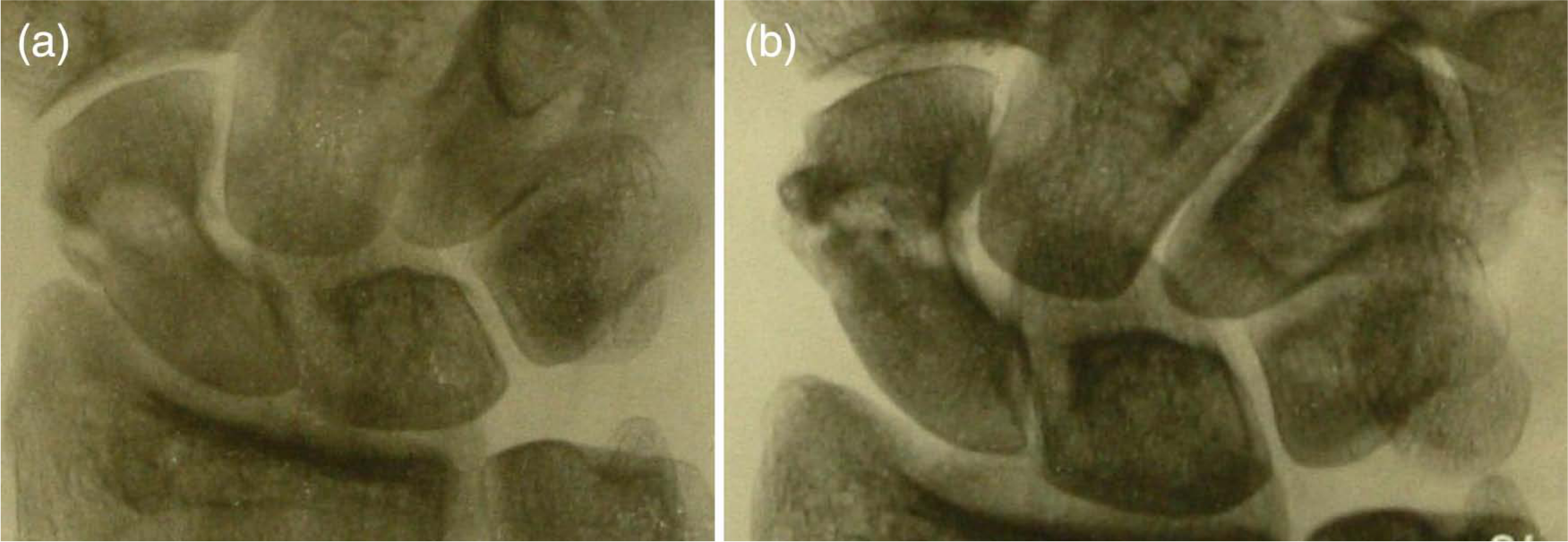
(a) First radiograph taken, three months after injury and (b) second radiograph taken, eight months after injury.
Our interpretation of the first radiograph pls change all of these to radiographs is not of an avulsion, but more likely a loose fragment from the scaphoid waist fracture (Figure 3a). In the second radiograph the fracture is clearly visible (Figure 3b). Both X-rays show obvious fractures and no sign of AVN.
Case 3
A 39-year-old male presented with pain in his wrist. He had fallen on his right hand 3 months earlier. Preiser reported the radiographs as showing mid-waist necrosis without any sign of fracture (Figure 4). No further radiographs were published. In our opinion, the pathology visible in the scaphoid could be a mid-waist fracture with possible cyst formation (Figure 4).
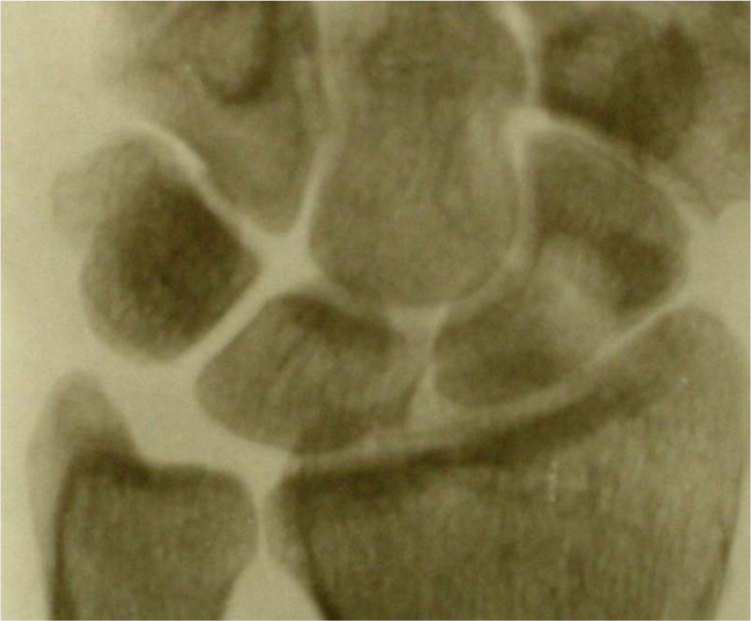
Radiograph taken three months after trauma.
Case 4
A 17-year-old male fell on his right hand 5 weeks earlier. He complained of pain and swelling around the scaphoid area. There was reduced extension and pain on palpation of the scaphoid and distal radius. On this radiograph, Preiser noted a fracture but stated that the primary problem was an interruption in blood supply (Figure 5). In our opinion, this radiograph shows cyst formation at the fracture line.
Radiograph taken five weeks after trauma.
Case 5
A 45-year-old male fell on his right wrist. He presented 1 week later. Preiser described a fractured distal radius and ulnar styloid as well as an area of density on the scaphoid, which he interpreted as AVN (Figure 6). We found this radiograph X-ray particularly hard to interpret. There are several fractures and the radiograph was taken in ulnar deviation. The distal pole of the scaphoid is dark, but so are the distal radius and part of the lunate. In our opinion, it is difficult to say whether or not there is a fracture of the scaphoid. We believe there is no sign of AVN of the scaphoid bone.
Radiograph taken one week after trauma.
Discussion
In his article Preiser described fives cases of rarefying osteitis. He diagnosed post-traumatic avascular necrosis of the scaphoid bone, without any sign of primary fracture (Preiser, 1910; 1911). He drew his conclusions from radiographs taken in one direction only and of poor quality. Even today, diagnosing AVN is not easy and it typically requires gadolinium enhance magnetic resonance imaing (Kalainov et al., 2003; Karantas et al., 2007).
Georg Preiser and Erich Lexer were far ahead of their time in using intravascular injections with contrast and radiographic imaging to visualise the vascular anatomy of bone, and in particular, the scaphoid (Lexer, 1908). Preiser discovered the largest blood supply of the scaphoid originated from the radial artery entering this bone through the dorsal surface, and — more than a hundred years ago — concluded that most of the proximal scaphoid bone was vascularised in a retrograde fashion. This has been confirmed in more recent studies (Botte et al., 2004; Fasol et al., 1978; Freedman et al., 2001; Gelberman et al.,1980; 1983; Handley et al., 1991; Lutzeler et al., 1932; Oehmke et al., 1987; Panagis et al., 1983; Taleisnik et al., 1966).
We believe very few people have seen Preiser’s original images. We found these original images in an archive with his first article. When searching the literature, we found two articles that describe and discuss the imaging of Preiser — Ferlic et al. (1989) and Taleisnik et al. (1966) — but were unable to find any documentation on the publishing of the original images. In this article we show these original radiographs, and on examining them we found pathology suggesting the presence of a primary fracture in all cases. With the knowledge we have today, we can state that Preiser misinterpreted his radiological findings, as in all five cases a primary fracture of the scaphoid was present and there was no proven avascular necrosis of this bone.
Over time, the eponym Preiser’s disease has come into being. In the literature Santozki and Kopelmann (1929) make the earliest references to Preiser’s disease. They use the term Preiser′s disease in their title: “Ein beitrag zur sogenannten malacia ossis lunatic et navicularis (Kienböck-Preiser’sche Krankheit)”. According to Ekerot et al. (1981), they subscribed to Preiser’s theory of progressive process of sclerosis, followed by necrosis, and ultimately fracture and collapse of the scaphoid (Ekerot et al., 1981). No other references to Santozki and Kopelmann were found. One other lead — McMaster et al. (1945) — was referred to by both Guelpa (1980) and Vidal et al. (1991). Unfortunately, even after a long search, the articles of Santozki and Kopelmann (1929) and McMaster et al. (1945) proved to be no longer available in any library in Europe, thus making it difficult to establish how the term spread. All other literature we found on Preiser’s disease dates from 1980 onwards.
From the 1980s, the eponym Preiser’s disease has continued to be used and several new definitions introduced. Despite what Preiser had originally stated, the term became synonymous with AVN of the scaphoid without previous trauma (Aptekar et al., 1974; de Smet et al., 1992; 1993; Harper et al., 1984; Kawai et al., 1983; Lenoble et al., 1994; Milgram et al., 1976) or osteochondritis dissecans (Aghasi et al., 1981; Baumann et al., 1977; Cook et al., 1993; Guelpa et al., 1980). Only a few authors, such as Bray and McCarrol (1984), still continued to use Preiser’s original definition.
In the literature the anatomical descriptions of Peiser’s disease vary. Certain authors describe necrosis of the whole scaphoid bone (Buttermann et al., 2004; de Smet et al., 1999; 2000; Ekerot et al., 1981; Ferlic et al., 1989; Virik et al., 2001), whereas others maintain that Preiser’s disease should only describe necrosis of the proximal pole of the scaphoid (Herbert et al., 1994). Sherman et al. (1983) suggest it should only refer to necrosis of the distal fragment.
In parallel with these diverse definitions, a wide-ranging aetiology has been described. Preiser’s disease has been used synonymously for idiopathic avascular necrosis, meaning avascular necrosis without clear aetiology (Allen et al., 1983; Alnot et al., 1990; Dossing et al., 1994; Ekerot et al., 1981; Ferlic et al., 1989; Gupta et al.,1992; Herbert et al., 1994; Jensen et al., 1995; Lauder et al., 2006; Martini et al., 1995; Parkinson et al., 1991; Zadeh et al., 1996; Zeng et al., 2001). Several nontraumatic causes have been described including steroid use (Chang et al., 1993; Kawai et al., 1983; Virik et al., 2001), systemic disease (Aptekar et al., 1974; Tate et al., 2000), chemotherapy (Chang et al., 1993; Harper et al., 1984), and smoking (Chang et al., 1993). As a result, Preiser’s disease also came to mean nontraumatic avascular necrosis of the scaphoid. (Beckmann et al., 2005; Budoff et al., 2006; de Smet et al., 1992, Hirohata et al., 1992; Imam et al., 2009; Kawai et al., 1983)
Many authors have reviewed the literature on Preiser’s disease. They concentrate mainly on the differences in the definitions of this eponymous condition; some have even suggested a better way of defining and describing AVN of the scaphoid by means of a classification system (Herbert et al., 1994; Kalainov et al., 2003; Schmitt et al., 2007).
A few articles on eponyms can be found. Mc Dowell (1977) and Ravitch (1977) wrote: “It has been stated that of eponyms several things may be true: (1) the individual thus memorialized was not the first to describe the condition, structure, or operation named after him; or (2) he misunderstood or did not understand fully what he described; or (3) he has been misinterpreted or misquoted; or (4) that all these are true.” They specifically point out Poland’s syndrome as example: “It is not always easy to find the basis on which an eponym has appeared in literature” (McDowell, 1977; Ravitch, 1977).
These apply for Preiser’s disease. Unfortunately, we were unable to trace who first coined the eponymous term Preiser’s disease.
In our opinion, all Preiser’s original images show a primary fracture and no sign of AVN, suggesting Georg Preiser misinterpreted his findings. Over the past hundred years, the eponym Preiser’s disease has been defined in many ways, varying from post-traumatic AVN to nontraumatic or even idiopathic AVN of the scaphoid. We believe the use of eponyms to be confusing, and Preiser’s disease is a good example of this. In conclusion, there is no uniformity regarding the definition, description, or aetiology of Preiser’s disease.
Footnotes
Conflicts of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.