
Abstract

Dear Sir,
Classical descriptions of the functional anatomy of the muscle belly of the flexor digitorum profundus (FDP III) muscle, i.e. to the middle finger, attributes its innervation to the median nerve (Oh et al., 2009). Thus, motion of the middle finger would depend exclusively on the median nerve as it also innervates the flexor digitorum superficialis (FDS) muscle. However, recent anatomical studies have questioned this common belief in favour of a dual innervation of the FDP III by both the median and ulnar nerves (Oh et al, 2009; Wong et al, 2010).
We analysed whether the ulnar nerve participates in the innervation of the FDP III. This was done thorough functional and neurophysiological studies in two groups of patients. FDP III and FDS III muscle strengths were graded using the MRCscale.
The first group included nine patients affected with total high median nerve palsies (eight male and one female) who were assessed between May 2010 and May 2013. All patients had some flexion of their middle fingers Grade M4 (Figure 1(A)). Flexion was attributed to FDP III since FDS testing revealed no active movement. The second group included 12 patients with a C5–C6 SD C7 brachial plexus, scheduled for an Oberlin’s transfer to restore elbow flexion between January and May 2013. They underwent selective median and ulnar nerve stimulation intra-operatively. In all patients ulnar nerve stimulation provoked flexion of the middle Grade M4 owing to FDP but not FDS contraction. In contrast, median nerve stimulation gave the middle finger flexion Grade M4 owing to contraction of both FDP III and the FDS III muscles (Figure 1(B)).
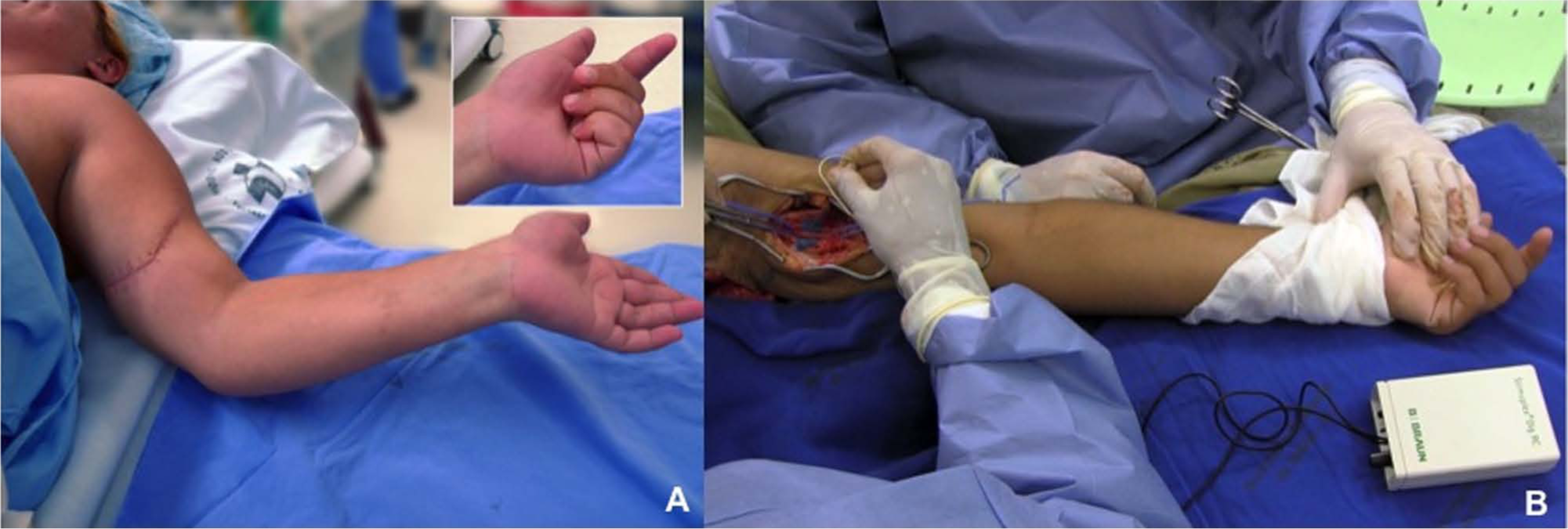
(A) 22-year-old patient with a complete median nerve palsy showing active middle finger flexion. (B) An intra-operative photo showing middle finger flexion after ulnar nerve stimulation in a 25-year-old patient before performing an Oberlin transfer for a C5–C7 brachial plexus palsy.
According to classical teaching, patients with high median nerve palsies should hold their radial two fingers in extension while the ulnar two fingers would sit with normal flexion (ulnar innervated FDP) (Oh et al., 2009; Wong et al., 2010). Our clinical findings in high median nerve lesions did not reproduce this classical description. None of our patients showed a complete palsy of the middle finger, but rather, had some preservation of FDP III muscle function.
In line with recent anatomical studies, our study supports the finding that the muscle belly of the FDP III is innervated by both the median and ulnar nerves. Ulnar nerve mediated flexion of the middle finger may result from some intertendineous connections, from variation in the innervation patterns, or both (Oh et al., 2009; Wong et al., 2010; Schreuders, 2012). In 92% of anatomical specimens the ulnar nerve participates in the innervation of the FDP III (Oh et al., 2009), and in 92.8% intramuscular communicating branches between the ulnar and median nerve are found within this muscle belly (Wong et al., 2010). These cadaveric studies could identify ulnar nerve branches entering the FDP III muscle, but could not confirm their motor function. Our clinical and neurophysiologic observations confirm that the ulnar nerve regularly contributes to flexion of the middle finger.
Footnotes
Conflict of interests
None declared.
Ethical approval
The local ethics committee approved the protocol of the study. Patients provided written informed consent before participation, in accordance with the Declaration of Helsinki guiding biomedical research involving human subjects.