
Abstract
The need for surgical correction in patients with malunion with mild dorsal angulation after a distal radius fracture is controversial. We specifically investigated in vivo changes in the lengths of carpal ligaments in a group of patients with mild-degree dorsal angulation following a distal radial fracture. We obtained computed tomography scans of both wrists in eight patients, whose distal radius on one side had united with dorsal angulation from 10° to 20°. The three-dimensional images of the carpus were reconstructed and the lengths of wrist ligaments were measured based on known anatomical landmarks. Compared with the contralateral uninjured side, the dorsal radiocarpal ligament and ulnotriquetral ligament were substantially lengthened (p < 0.05) and the long radiolunate ligament was substantially shortened (p < 0.05) at most wrist positions except extension. However, five other ligaments that we measured did not show significant differences in length compared with those of the uninjured side (p > 0.05). The lengths of some ligaments are substantially altered even by mild dorsal angulation of the distal radius, while the lengths of most other ligaments are not substantially affected.
Keywords
Introduction
Malunion of the distal radius is the most commonly reported complication of distal radius fractures (Cooney et al., 1980; Haase and Chung, 2012; McQueen and Caspers, 1988). Dorsal angulation of the radius is the most common type of malunion. Malunion with dorsal angulated position can lead to loss of wrist flexion, limited or painful forearm rotation, arthritis of the distal radioulnar joint, late median neuropathy, loss of extensor tendon efficiency, and carpal instability.
Length changes of carpal ligaments have been studied in cadavers (Berger, 2001; Nagao et al., 2005; Savelberg et al., 1993; Viegas et al., 1999), in normal wrists in vivo (Moritomo et al., 2008; Tang et al., 2011; Xu and Tang, 2009a), and in patients with distal radius fractures (Viegas et al., 1999). We are unaware of any previously published studies that sought to determine the length changes of carpal ligaments in dorsal angulated malunited distal radius fractures.
The purpose of the present study was to determine the length changes of carpal ligaments in vivo in distal radius fractures with mild malunion.
Materials and methods
For this investigation, we recruited eight patients (one man and seven women) who had suffered malunion following a distal radius fracture. Their average age was 60 years (range 53–75). The inclusion criteria for the present study were: malunion of an isolated distal radius fractures with dorsal angulation from the horizontal between 10° and 20°; ulnar variance < 3 mm (Figure 1); over 6 months from injury to testing; the absence of any disease that might affect wrist structure or function; and the absence of severe medical illness or cognitive disorder precluding participation in the follow-up examination.

The anterior-posterior view (A) and lateral view (B) of the X-ray films of a malunited distal radius. (A) In all wrists, the ulnar plus variation (H) was 0–3 mm. (B) The dorsal angulation (∠α) was between 10° and 20°.
Assessments
Bilateral posteroanterior and lateral radiographs were taken to confirm the absence of bone and joint abnormalities in the normal wrist and forearm. The average dorsal angulation for the injured side was 15° (4.1) and the palmar tilt for the uninjured side was 14° (3.8) (p < 0.01). The average time from injury to testing was 20 months (range 7–44). The average radial angulation was 20° (4.4) for the injuried side and 25.4° (2.3) for the uninjured (p < 0.05).
In the computed tomography scanner, the volunteers held their arms out straight in the ‘superman’ position. The positions of their wrists were controlled, held in custom-designed jigs equipped with protractors to assist in wrist positioning. The neutral position of the wrist was targeted by visually aligning the third metacarpal with the long axis of the forearm. Computed tomography images were collected at five wrist positions: the neutral position of the carpus; 20° of ulnar deviation; 20° of flexion; 20° of extension; and 40° of extension. Both wrists of each subject were imaged simultaneously with a high-speed, 16-slice, spiral computed tomography scanner (Somatom Sensation 16; Siemens Medical Solutions, Forchheim, Germany) to obtain images at a maximum of 120 kVp and 80 mA. Contiguous 0.75-mm slice images were acquired from the distal parts of the radius and ulna to the heads of the metacarpals at each designated wrist position.
The three-dimensional structures of the entire carpus, including the distal part of the radius and ulna and the metacarpal bones, were reconstructed for each patient, with use of an established method of three-dimensional bony reconstruction (Crisco et al., 1999; Marai et al., 2004; Tang et al., 2011). The three-dimensional images of these wrists were reconstructed with use of an analytic software program (Mimics 10.01; Materalise, Leuven, Belgium).
Measurements
The lengths of carpal ligaments
Eight ligaments were measured based on anatomical insertions obtained from anatomical studies of Viegas et al. (1999), Nagao et al. (2005), and Berger (2001). These ligaments are the radioscaphocapitate (RSC), long radiolunate (LRL), ulnolunate (UL), ulnocapitate (UC), ulnotriquetral (UT), dorsal radiocarpal (DRC), and dorsal intercarpal (DIC) ligaments each with two bony insertions (Figure 2). We marked the origins and insertions of these ligaments on the computer created bony surface.
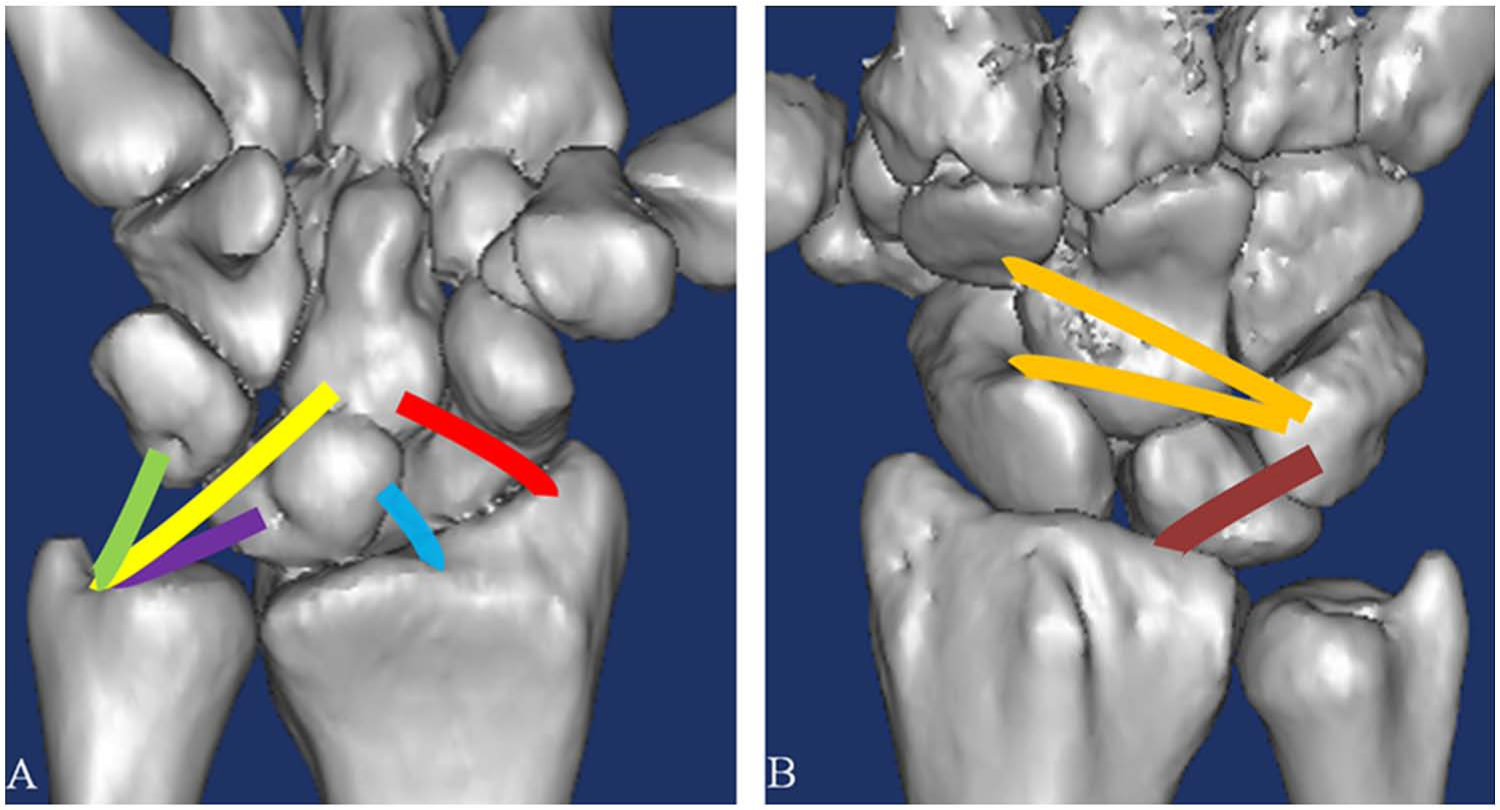
The insertions and paths of eight studied carpal ligaments. The measurements of the lengths of these ligaments were taken at the middle portion of the attachment. (A) Palmar ligaments: RSC (red), LRL (light blue), UC (yellow), UL (purple), and UT (green). (B) Dorsal ligaments: DIC in two portions (both in yellow) and DRC (purple).
The RSC ligament originates from the distal radius in the zone, from the tip of the radial styloid process to approximately the middle of the scaphoid fossa, and attaches to the volar aspect of the capitate to merge with the fibres of the UC ligament, which originates from the ulna fovea. The LRL ligament originates from the distal and palmar aspect of the radial styloid process and attaches to the lunate at the radial aspect of the palmar cortex. The UL originates from the palmar distal radioulnar ligament and attaches to the palmar aspect of the lunate. The UT originates from the palmar-radial aspect of the base of the ulnar styloid and attaches to the proximal and ulnar surfaces of the triquetrum (Marai et al., 2004; Xu and Tang., 2009a). The DRC originates from the ulnar and dorsal ridge of the distal end of the radius and attaches to the dorsal aspect of the triquetrum and, in some wrists, to the dorsal aspect of the lunate as well. In this study, we only measured the lengths of the fibres attaching to the dorsal cortices of the triquetrum. The DIC ligament originates from the dorsal tubercle of the triquetrum: the DIC-1 (inserting on the trapezoid) and DIC-2 (inserting on the dorsal cortices of the distal scaphoid). The lengths of these ligaments were investigated as in previous studies (Moritomo et al., 2008; Xu and Tang, 2009a).
The paths of the fibres of the eight ligaments were modelled according to the methods previously described (Chen and Tang, 2013; Crisco et al., 1999; Marai et al., 2004; Tang et al., 2011; Xu and Tang, 2009a, 2009b). This method takes into consideration the proper projection of the course of the ligaments by bony contour. When there was no intervening bone, the shortest paths were modelled and measured directly. When there was an intervening bony component, the ligament was projected around the bony contour and paths of the ligaments were then modelled. We measured the lengths of the ligaments using by the bone distance–field representation method and used them for statistical analysis.
Statistical methods
The data are expressed as means and standard deviations. The two-way repeated measure analysis of variance was used to determine the significant difference in the comparison in the multiple positions and between the diseased and contralateral uninjured sides. When significant difference was found among these data, a two tailed paired t-test was used to compare each pair of data of the lengths of the carpal ligaments in the uninjured and malunited forearms. The level of significance was set at p < 0.05.
The institutional review board approved this study.
Results
The lengths of the ligaments in the uninjured wrists
The lengths and percentage changes of the uninjured carpal ligaments are detailed in the 1 and Figure 3. Compared with the neutral position, the RSC ligament and LRL ligaments lengthened significantly as the wrists deviated 20° ulnarly (p < 0.001) or extended 20° or 40° (p < 0.05) while they shortened with the wrist flexed at 20° (p < 0.001). The UC ligament also lengthened as the wrists deviated 20° ulnarly or extended 40° (p < 0.05), but did not shorten significantly as the wrist flexed 20°. The UT ligament shortened as the wrist deviated 20° ulnarly (p < 0.001). The DRC ligament lengthened as the wrist flexed 20° (p < 0.001) and shortened at the other three positions (p < 0.05). The DIC1 and DIC2 ligaments showed no significant changes as the wrists changed position (Figure 3).
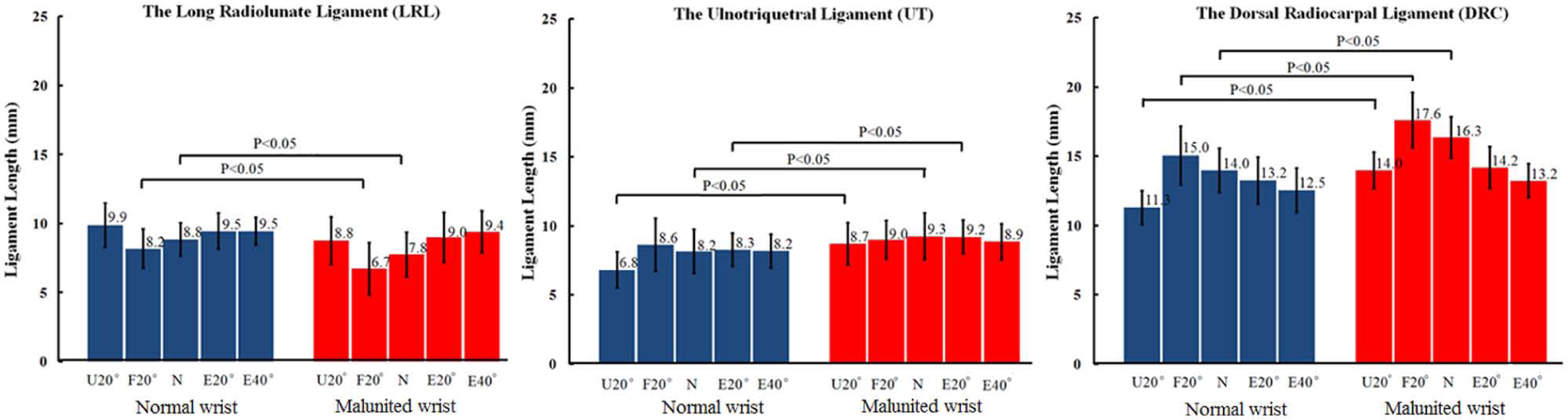
The lengths of LRL, UT, and DRC ligaments at 5 wrist positions. Compared with the same position of the normal wrist, the LRL ligament was shortened at neutral position, The UT ligament was lengthened when the wrist extended 20 degrees or ulnarly deviated 20 degrees, the DRC ligament was lengthened at the wrist ulnar deviation of 20 degrees or neutral position.
The lengths of ligaments of malunited wrist
As shown in Figure 3, the length of the LRL, UT, and DRC ligaments were also changed as the wrist position changed. However, the UT ligament lengthened at 20° of ulnar deviation in the malunited wrist as opposed to shortening in the normal wrist. The UT ligament lengthened at 20° of flexion and at neutral position of the wrist in the malunited wrist compared with the opposite. The DRC ligament also lengthened at 20° of ulnar deviation, 20° of flexion, and at neutral position of the wrist after malunion of the distal radius compared with the opposite.
The differences between the uninjured wrist and the malunited wrist
Table 1 details the comparisons of the lengths of these ligaments between uninjured and malunited wrists. Compared with the uninjured side, the DRC ligament showed the greatest length changes, and the DRC and UT ligaments were lengthened significantly at the neutral positions. The DRC ligament lengthened significantly compared with that of the uninjured wrist at neutral, 20° of ulnar deviation, and 20° of flexion (p < 0.05), but not at the other two tested positions. The UT ligament lengthened significantly compared with the uninjured wrist in neutral position, 20° of ulnar deviation, and 20° of extension (p < 0.05). The LRL ligament shortened significantly compared with that of the uninjured wrist at 20° of flexion and in neutral (p < 0.05) (Figures 4 and 5).
Lengths of the eight carpal ligaments at neutral position and length changes at selected carpal positions of both wrists.
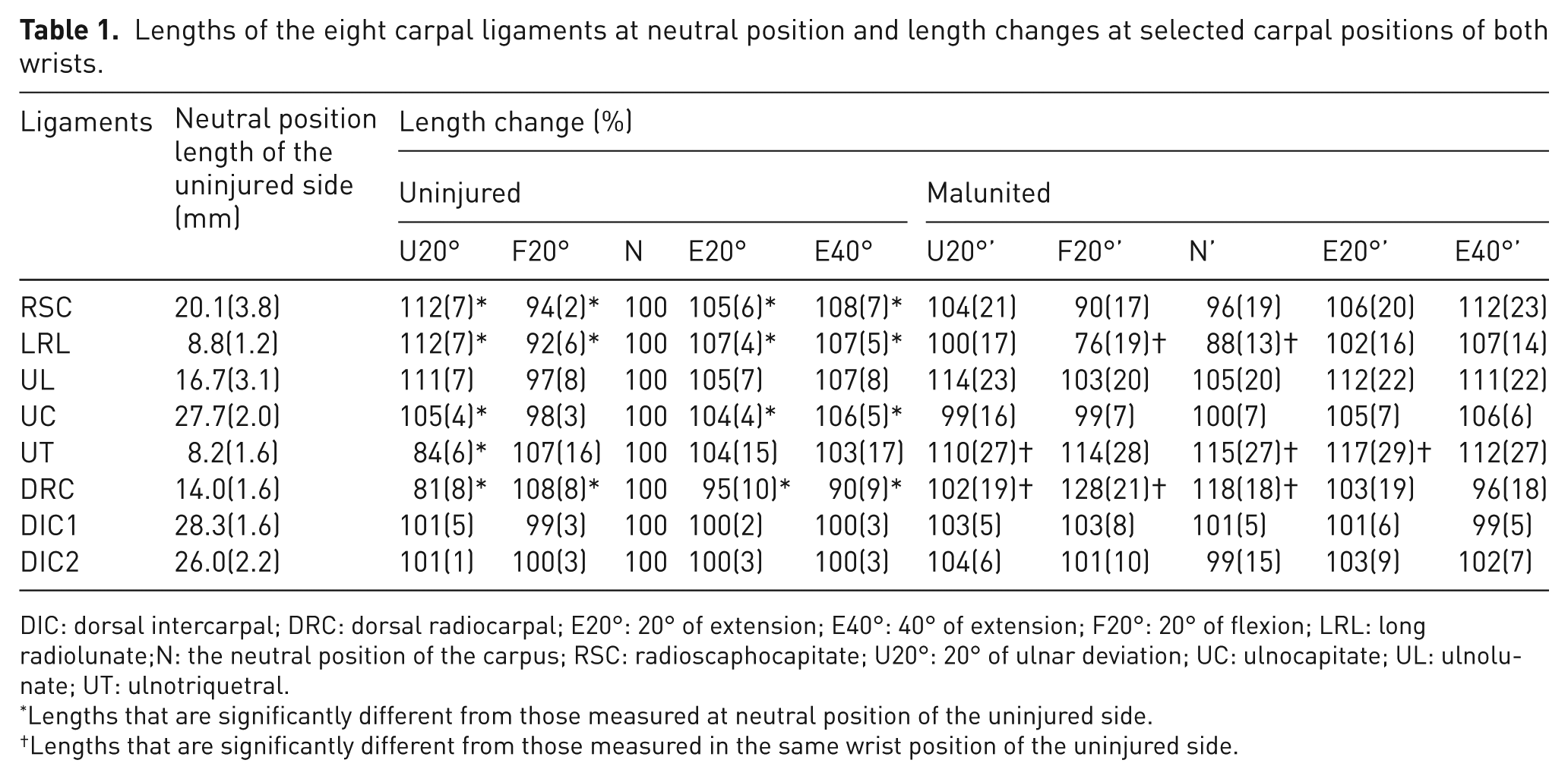
DIC: dorsal intercarpal; DRC: dorsal radiocarpal; E20°: 20° of extension; E40°: 40° of extension; F20°: 20° of flexion; LRL: long radiolunate;N: the neutral position of the carpus; RSC: radioscaphocapitate; U20°: 20° of ulnar deviation; UC: ulnocapitate; UL: ulnolunate; UT: ulnotriquetral.
Lengths that are significantly different from those measured at neutral position of the uninjured side.
Lengths that are significantly different from those measured in the same wrist position of the uninjured side.
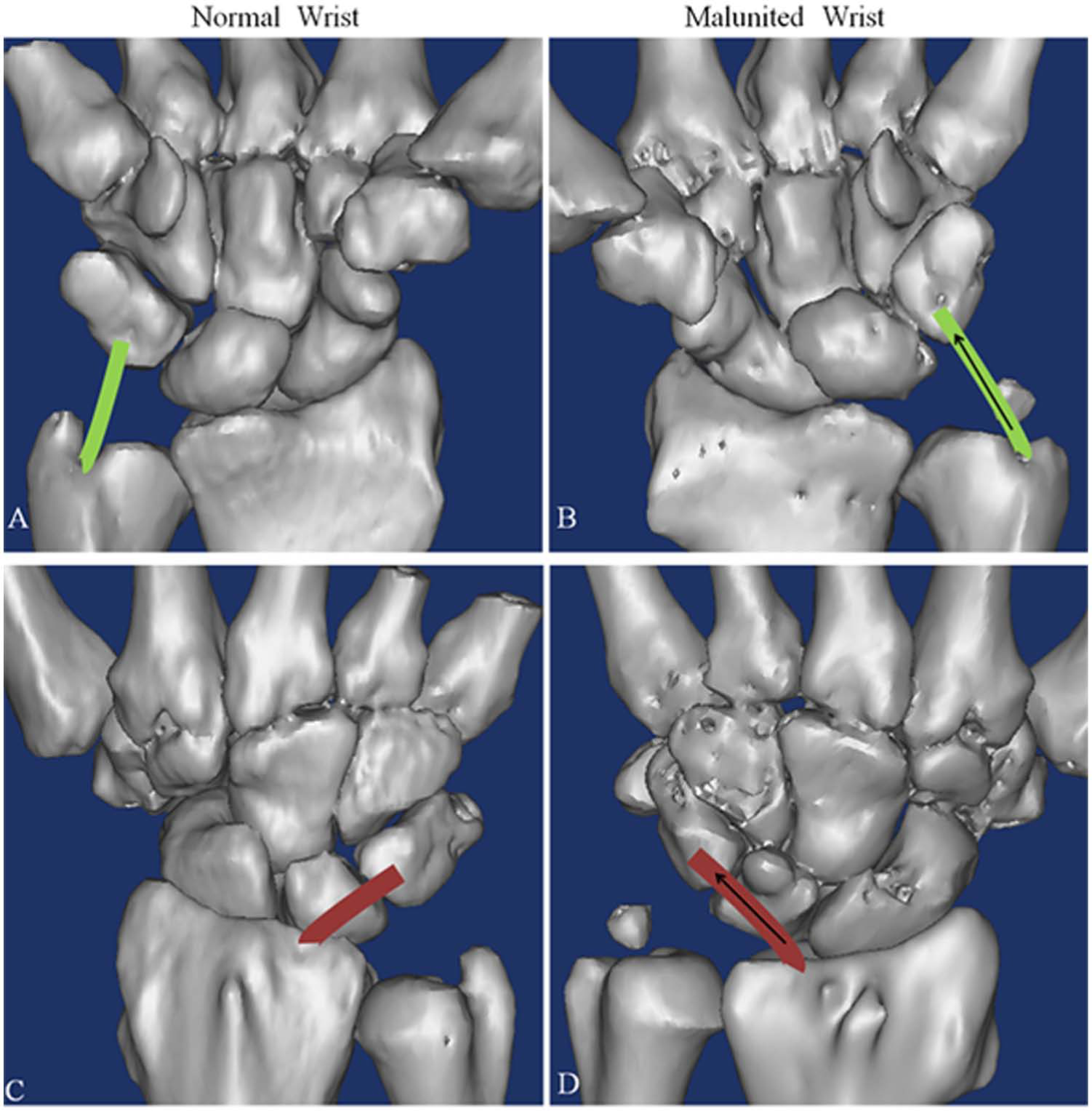
Length changes of the UT and DRC ligaments illustrated in the three-dimensional images of the volar and dorsal views obtained at neutral position. (A) and (B) are the palmar view. (C) and (D) are the dorsal view.
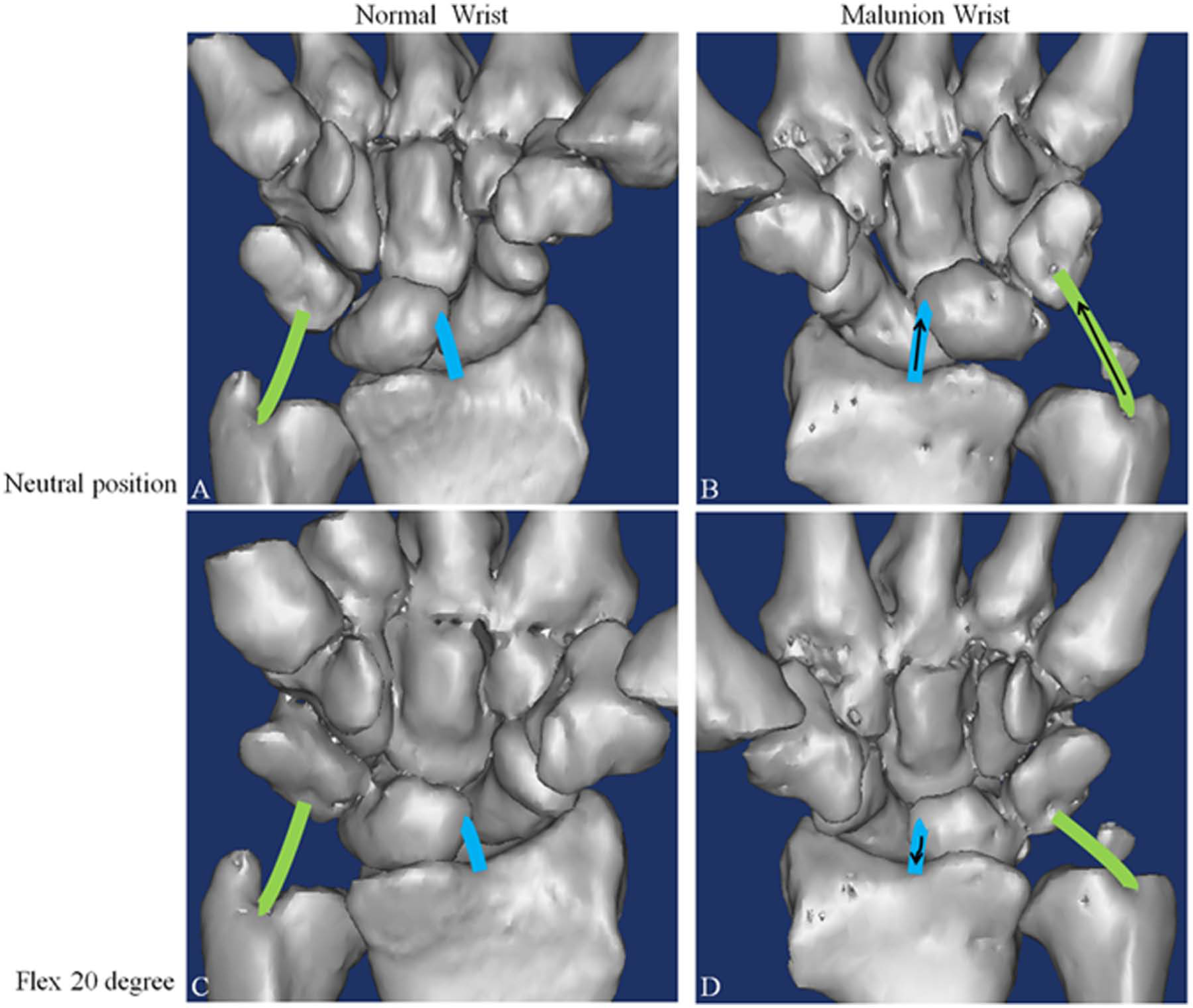
Length changes of the UT and LRL ligaments in the three-dimensional images obtained at neutral position or flexion of 20° of the wrist. All images shown are the volar view.
Discussion
Our study showed that following mild (between 10° to 20°) dorsal malunion and 5° loss of radial angulation of the distal radius, the ligaments of the wrist largely changed with movement as for the normal wrists. Compared with the uninjured wrist, the major differences in the changes of the lengths of the ligaments after mild malunion of the distal radius fracture are: (1) the lengths of the UT and DRC ligaments are substantially lengthened and those of the LRL ligament are substantially shortened in neutral; (2) the lengths of the UT ligaments are substantially lengthened during most wrist motion; and (3) the lengths of the DRC ligaments are substantially lengthened during ulnar deviation and flexion. The mild malunion does not affect the lengths of the other ligaments.
The mild malunion of the distal radius fracture appeared to have the greatest influence on the lengths of the DRC and UT ligaments. The increases in their lengths were mostly between 15% and 30% (Figures 4 and 5). This increase in ligament length is very high for a capsular ligament of the wrist such as DRC compared with other studies (Tang et al., 2011). Such ligament changes appear logical, as this is a dorsal ligament. The capitate and lunate tend to protrude against it in neutral or flexion because of the dorsal angulation malunion of the distal radius. The increase in length of the UT ligament in neutral, flexion, and ulnar deviation in malunite wrist is harder to explain. This change may relate to dorsal translation of the triquetrum, which lengthens the UT ligament in wrist flexion and ulnar deviation.
We generally recorded greater changes in ligament length in neutral, flexion, and ulnar deviation than in extension (Figures 4 and 5). This is understandable, as wrist extension effectively restores the ‘normal’ alignments of the carpal bones and distal radius (Wolfe et al., 2000), thus maintaining ligament lengths closer to those in the uninjured wrists.
The LRL is a volar ligament connecting the radius to the lunate (Berger, 2001). Our study showed that this ligament is substantially shortened in the neutral and in flexion in the malunited wrist. This change is also in agreement with deformity after mild malunion of the distal radial fracture. Palmar flexion of the lunate is exaggerated during flexion and in neutral after dorsal malunion of the distal radius. Therefore, the insertion point of the LRL in the lunate is brought closer to the insertion of this ligament in the palmar rim of the distal radius, resulting in shortening of the LRL ligaments.
Past studies have documented loss of function of the patients with malunion of the distal radius fracture when dorsal tilt exceeds 10° (Del Piñal et al., 2009; Henry, 2007; Wada et al., 2011). The role of corrective osteotomy is controversial (Hsieh et al., 2010; Lozano-Calderón et al., 2006; Malone et al., 2006; Ring et al., 2005; Ruch et al., 2010; Sato et al., 2009; Verhaegen et al., 2010; Wada et al., 2011). The mild-degree deformities after malunion of the distal radius fracture were found to be associated with higher arm-related disability after injury and limitation of wrist motion than normal wrists (Del Piñal et al., 2009; Henry, 2007). Wada et al. (2011) found that after corrective osteotomy for mild to severe malunited distal radius fractures, the patients’ ranges of flexion, extension, supination, ulnar deviation, and their grip strength improved significantly. Some surgeons have found that minimal deformities also benefit enormously from osteotomy (Del Piñal et al., 2009; Henry, 2007). Many other surgeons have recorded that dorsal angulation between 10° and 20° may not need correction, especially in elderly patients (Becker and Owers, 2012; Brogren et al., 2011; Chia et al., 2011).
It has been well documented that abnormal alignment and motion of the carpal bones leads to mechanical overload of the wrist (Anderson et al., 2005). This overload can cause ligament attenuation, synovitis, and progressive dynamic instability (Pogue et al., 1990). A number of previous mechanical studies have also revealed that this degree of mild dorsal angulation may cause only a small degree of mechanical disturbance (Park et al., 2002; Saito et al., 2013; Tang et al., 1999).
There were some limitations to our study: only eight carpal ligaments were compared; potential individual variations in ligamentous anatomy were not taken into account (Crisco et al., 2005; Moritomo et al., 2008); we assumed that the ligaments of the malunited wrists were intact; all the patients had ulnar variance of less than 3 mm, but there was significantly radial deviated on the malunited side, which could affect the result; and we obtained data from a limited number of wrist positions for each volunteer; we could only examine the carpal ligaments over a limited range of the wrist motion, because of stiffness in the malunited wrists.
In conclusion, malunion of the distal radius with a mean of 15° dorsal angulation and ulnar tilt decrease of 5° affects three ligaments’ lengths of the selected eight carpal ligaments. The DRC ligament and UT ligament were substantially lengthened and the LRL ligament was substantially shortened at most wrist positions except extension for the malunited side. Five other ligaments that we measured did not show significant differences in length compared with those of the uninjured side.
Footnotes
Conflict of interests
None declared.
Funding
Supported by the Health Bureau of Jiangsu Province, Natural Science Foundation, and Affiliated Hospital of Nantong University.