
Abstract

Dear Sir,
A 46-year-old right-handed man presented with a 2-year history of unilateral Dupuytren’s disease in the right hand, with a contracture of the ring and little fingers that had progressed over a period of 1 year. He worked as a carer for autistic adults and his duties involved regular shaving of those in his care. On questioning, no localized infections or episodes of inflammation had been noted in the palm. Pre-operative examination revealed Tubiana stage II disease on the right ring and stage III disease in the right little finger. One palmar pit was observed with no evidence of inflammation.
A fasciectomy was carried out on the right palm, right ring and little fingers under general anaesthetic as a day case. It was noted that several hairs were emanating from the palmar pit (Figure 1). It was noted that the complex resembled a pilonidal sinus and a specimen was sent for histopathological examination. Full release of the contracture was obtained and the post-operative course was uneventful. Histology confirmed the presence of fibrous connective tissue within which there was a sinus tract, lined in part by squamous epithelium and in part by inflamed granulation tissue with a foreign body giant cell reaction to polarizable hair (Figure 2). These features were in keeping with a pilonidal sinus. A 2-year follow-up revealed no recurrence of the pilonidal sinus or Dupuytren’s disease.
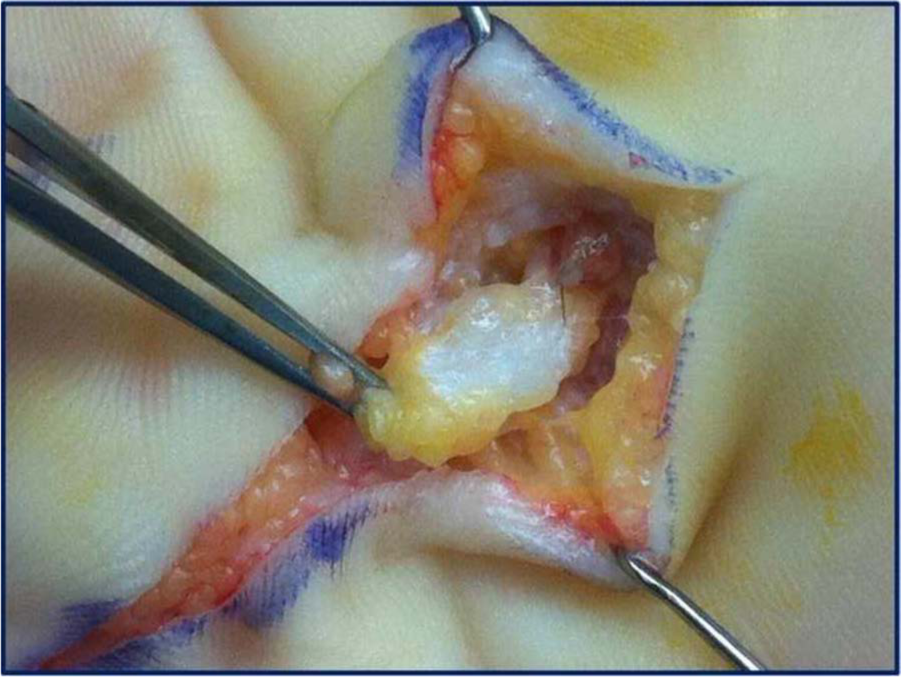
Hairs noted at the base of the Dupuytren’s pit.
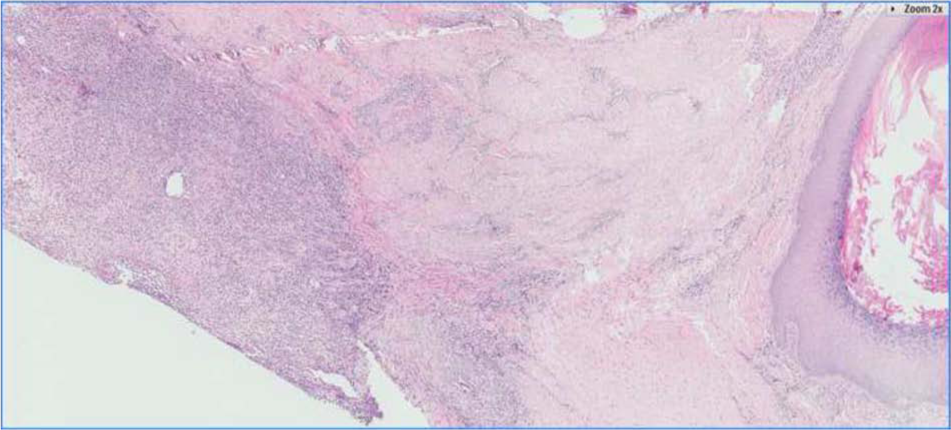
Histological section showing both pilonidal sinus and Dupuytren’s pathology.
Pilonidal sinus disease of the hand has been described in barbers, dog groomers and those who shear sheep (Mohanna et al., 2001). In contrast with pilonidal disease elsewhere in the body, the sinus does not contain the hair of the individual, but hair from another. Most sinuses affect the interdigital space, but there have been case reports of sinuses in the subungual and pulp spaces, and one episode of associated osteomyelitis of the underlying distal phalanx (Mohanna et al., 2001). There is no consensus about appropriate management. Opinion is divided between excision and primary closure, allowing to heal by secondary intention, negative pressure treatments and the interposition of vascularized tissue (Aydin and Mengi, 2010). The injection of dye to outline the tract has been found to be useful in aiding complete excision (Uysal et al., 2003). The two markers of successful treatment are the absence of recurrence and avoidance of web space contractures (Aydin and Mengi, 2010; Eryilmaz et al., 2012).
Although palmar pits are a common feature of Dupuytren’s disease, we have not found a previous report of a pilonidal sinus being found within the pit itself. The case appeared to be typical Dupuytren’s disease, but we must accept that the foreign body reaction to the hair may have been a possible cause of the fibromatosis, given there was no evidence of fibromatosis in the contralateral hand and no family history of Dupuytren’s disease.
Footnotes
Conflict of interests
None declared.