
Abstract

Dear Sir,
A 49-year-old Caucasian male industrial worker presented with a 3-year history of a progressive painless swelling on the dorsum of the right hand. He described an industrial accident that had caused a laceration of the dorsum of the hand with penetration of foreign particles into the soft tissue 16 years previously. He had no significant past medical history.
Physical examination revealed an 8 × 3 cm soft, non-tender mass on the dorsum of the wrist. The range of wrist motion was 80° flexion to 60° extension. The range of metacarpophalangeal motion was within normal limits. Haematological investigations were normal. A lateral radiograph of the right wrist was insignificant other than the soft tissue swelling in the region of the carpal bones. Magnetic resonance imaging showed proliferating synovium composed of villous frond-like projections that had the signal intensity of subcutaneous fat, predominantly in the second and third, and partially in the fourth extensor tendon compartments (Figure 1).
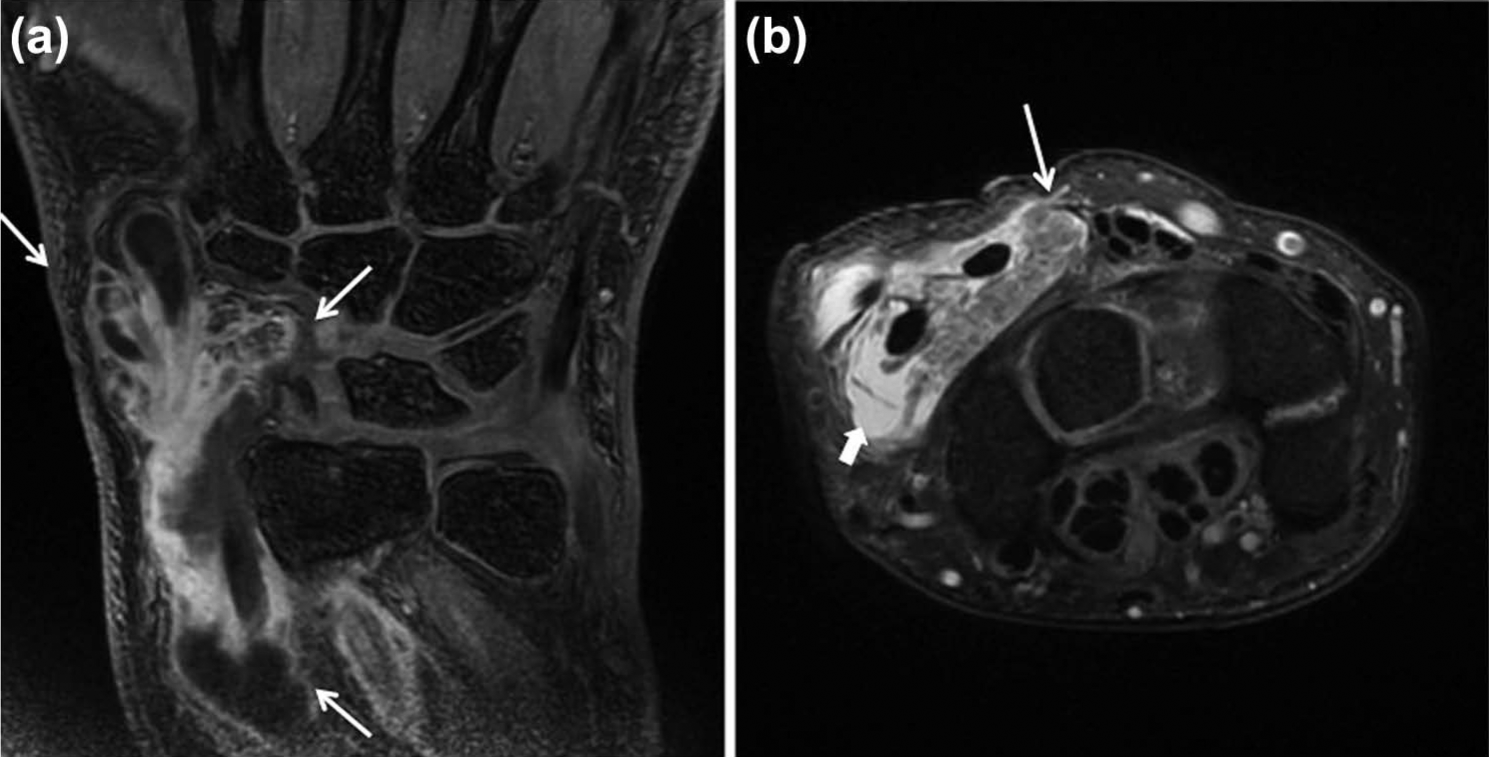
Lipoma arborescens of the extensor tendon sheath of the wrist. (a) Coronal three-dimensional T1-weighted fat-saturated magnetic resonance image shows that the lesion extends from the distal one-third of the radius to the base of the index metacarpal. (b) Axial post-contrast fat-saturated image at the level of the first carpal row demonstrates frond-like tissue extending from the synovium with signal characteristics consistent with fat (arrows) in association with fluid (solid arrow).
The lesion was excised via a 10 cm curved dorsal longitudinal incision and villous frond-like fatty tissue was identified involving the synovium. The specimen consisted of bright yellow soft tissue. Microscopically, samples displayed large groups of mature adipocytes infiltrating subsynovial areas, and a synovial inflammatory reaction consisting mainly of lymphocytes with focal fibrin deposition. These findings were interpreted as fibrinous synovitis and lipoma arborescens (LA). In addition to these findings, scattered granulomas with foreign body-type giant cells engulfing foreign bodies were noted (Figure 2).
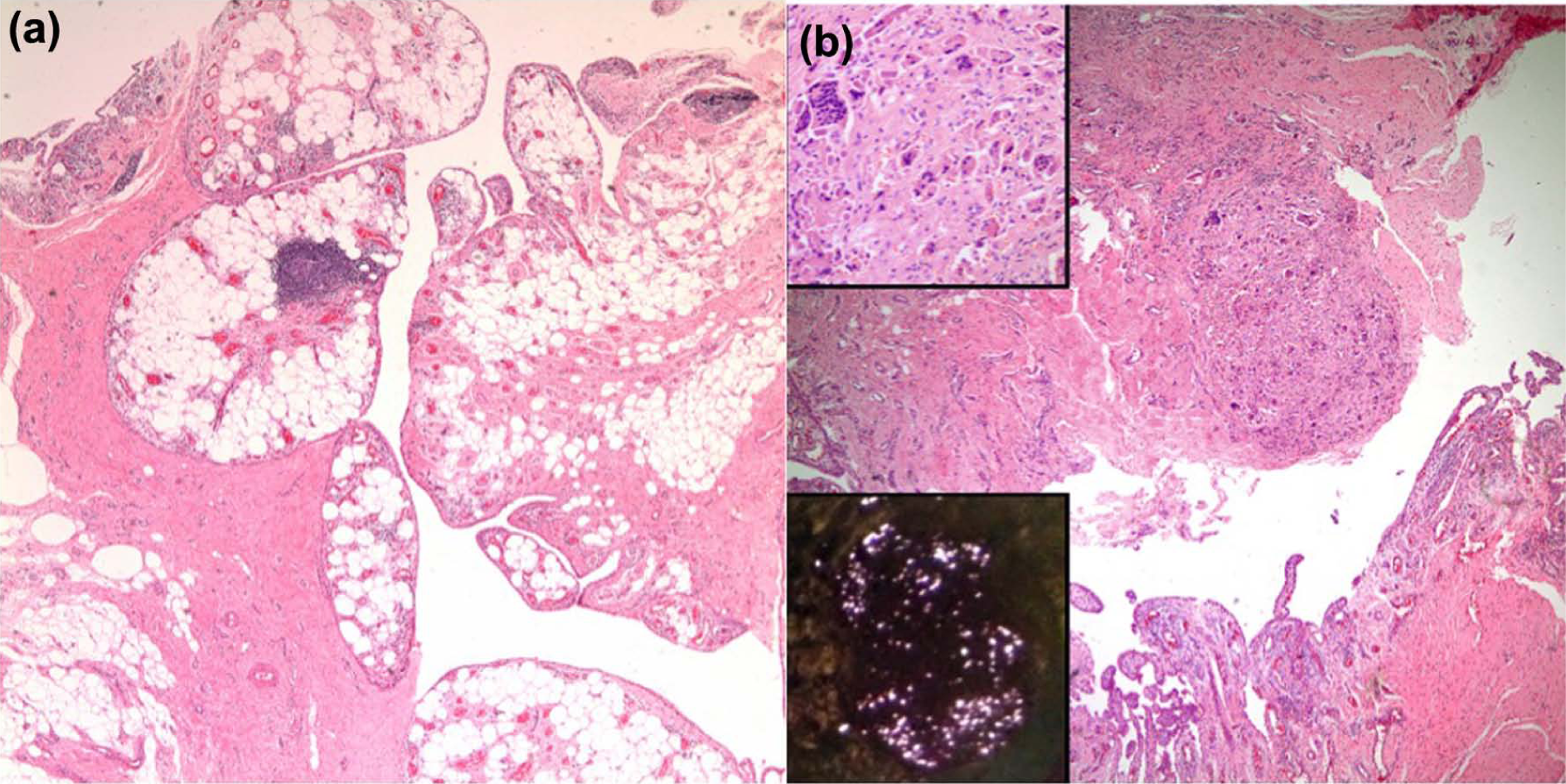
(a) Subsynovial groups of adipocytes forming vaguely papillary structures (haematoxylin and eosin stain, original magnification ×40). (b) Another part of the sample displaying a nodular aggregate of foreign-body type multinuclear giant cells At higher magnifications, these cells were seen to engulf brightly eosinophilic, rectangular acellular material (upper inset), which were birefringent under polarized light (lower inset).
LA is a benign intra-articular lesion characterized by the replacement of the sub-synovial tissue by mature fat cells giving rise to a villous proliferation. It is usually mono-articular, most frequently involving the knee, and rarely seen extra-articularly. Reported areas include the sub-deltoid bursa, elbow, hand, ankle, and peroneal tendon sheath. It has been concluded that irritation of the joint lining, either with a mechanical or inflammatory reaction, may result in this rare proliferative response (Coll et al., 2011). LA can be diagnosed using magnetic resonance imaging. The differential diagnosis includes synovial lipoma, synovial chondromatosis, pigmented villonodular synovitis, synovial haemangioma, and rheumatoid arthritis. Treatment of LA is by open or arthroscopic surgical excision, depending on the extent of involvement. Recurrence of the lesion might be seen due to the underlying persistent inflammatory condition (Sheldon et al., 2005).
There are a few reported cases of LA located around the wrist. Hill and Pyho (2011) reported a case of LA located on the dorsal aspect of the hand with an underlying non-displaced scaphoid fracture and degenerative radio-scaphoid arthritis. Stepan et al. (2013) reported a case of extra-articular LA with direct invasion of the fourth extensor compartment in a young patient presenting with a chronic mass on the dorsal aspect of the wrist of unknown aetiology. We have not found another case in which the condition was secondary to a reaction to a foreign body
Footnotes
Acknowledgements
The authors would like to thank Dr Gunes Guner and Dr Kemal Kosemehmetoglu and Hacettepe University Department of Pathology for their assistance in the preparation of the pathology slide images.
Conflict of interests
None declared. Informed consent was obtained from the patient.