
Abstract
Patients awaiting surgery for Dupuytren’s contractures listed the problems from their Dupuytren’s disease that had led them to request surgery and their relative priorities of the results of surgery. The listed problems were compared with the nine items comprising the Unité Rhumatologique des Affections de la Main (URAM) Dupuytren’s disease-specific outcome measure. One hundred and ten patients reported 278 problems. Ninety-four different combinations of problems were provided by patients, and over half (55%) of the problems were not captured by items in the URAM scale. The long-term outcome from surgery was relatively more important to patients than speed of recovery. The URAM tool may not be relevant to patients in the UK, and further assessment of its face validity is required before it is used.
Level of evidence: III
Introduction
The use of patient-reported outcome measures (PROMs) in healthcare has been stimulated by recent UK Department of Health publications (Darzi, 2008; Department of Health, 2010). Interest in their development and use across Europe and North America is evident from groups such as the COSMIN collaboration (Mokkink et al., 2010). PROMs may be of particular use in hand surgery, as patients’ functional requirements vary, and so do their expectations of treatment and definition of a satisfactory outcome. PROMs used in hand surgery are classified into generic tools that assess global well-being (e.g., EuroQol 5D), domain-specific tools that assess a particular region (e.g., Disabilities of the Arm, Shoulder and Hand [DASH] tool [Hudak et al., 1996] or Patient Evaluation Measure [PEM] [Macey et al., 1995]), and disease-specific tools (Szabo, 2001). Whilst generic and domain-specific tools can be used to assess outcome for upper limb conditions, they have low sensitivity and specificity, and may not detect changes in symptoms or hand function that are relevant to patients. They can also be subject to ceiling or floor effects, which occur when many individuals’ scores are close to the upper (ceiling) or lower (floor) limit of the scale (Szabo, 2001). This limits the ability of the scale to detect further improvement or deterioration, respectively.
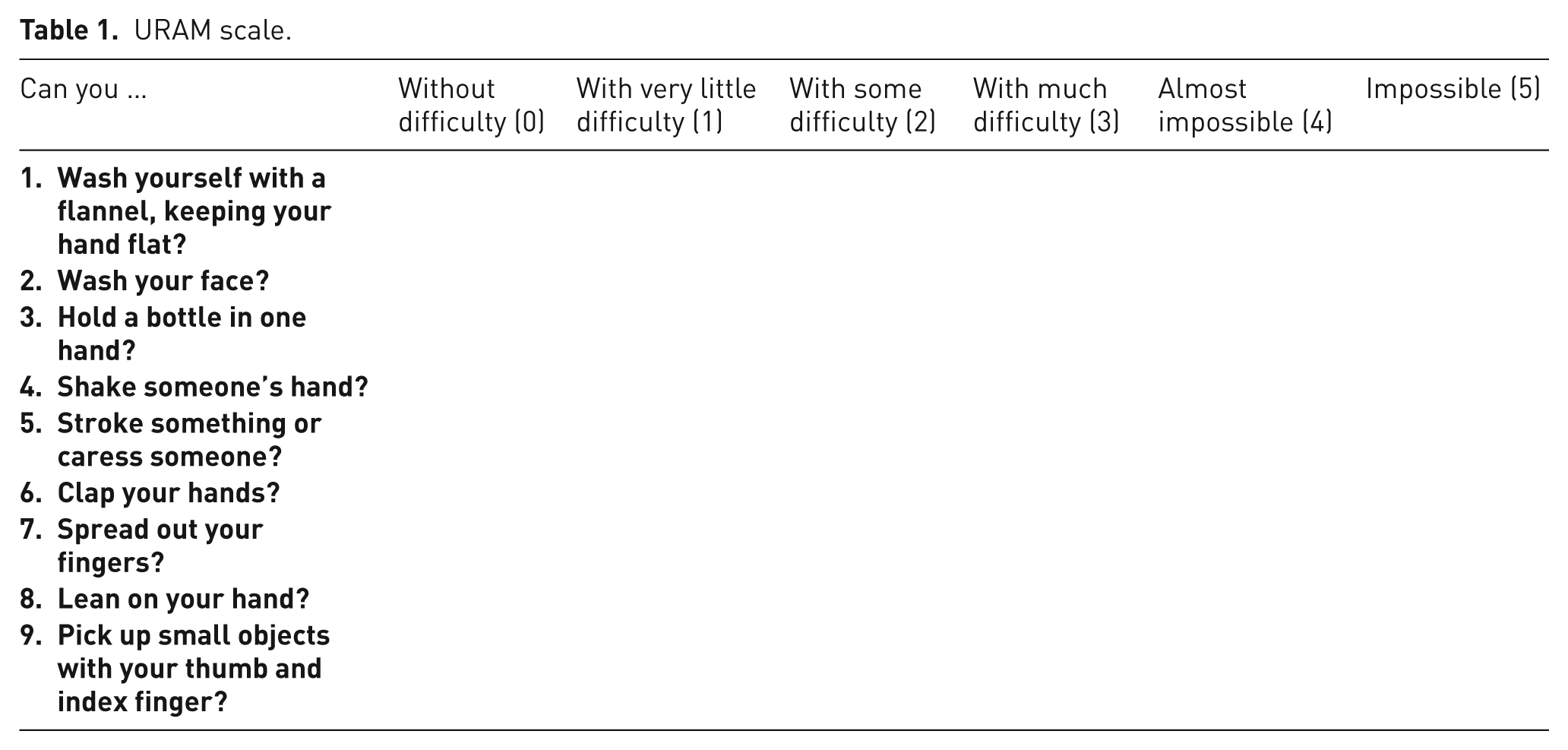
Recently, a Dupuytren’s disease-specific tool was developed in France (Beaudreuil et al., 2011). This Unité Rhumatologique des Affections de la Main, or URAM, scale comprises nine items, which are each scored between 0 and 5 depending on the difficulty in performing that particular function (Table 1). Nine patients and seven healthcare professionals generated an initial battery of items that were then reduced to the nine items comprising the final scale, via a process involving a further 85 patients. However, all were recruited at a single hand surgery centre in Paris.
URAM scale.
It is unclear whether the URAM is broadly applicable and culturally generalizable, and therefore it is unclear whether it is valid for use elsewhere. This prospective study aimed to identify patients’ indications for Dupuytren’s disease surgery at a hand surgery centre in the UK and compare them with the URAM scale items.
Methods
Data collection involved the baseline time point of a service evaluation and took place between September 2011 and April 2013. The inclusion criteria were:
Patients awaiting fasciectomy or dermofasciectomy at the hand surgery centre.
Primary or recurrent Dupuytren’s disease.
Available for a pre-operative assessment at a time when the primary author (JR) was available.
Exclusion criteria were:
Cognitive impairment preventing informed consent.
Refusal of invitation to participate.
Eligible patients were issued with a letter, which explained the project and invited them to participate on a voluntary basis. A single surgeon (JR) assessed all patients who consented to participate. Details of patient demographics and planned procedure were recorded.
Patients were asked to specify up to three functional problems they were experiencing and wished their proposed surgery to resolve. Free text answers were recorded, so that participants were not restricted to grading their ability to specify tasks or the severity of particular symptoms. They were not asked to rank these indications. Indications were specified before the patients completed any established PROMs as part of their service evaluation to avoid them being influenced by the items in existing PROMs.
One author (JR) then grouped the free text indications, so that different descriptions of the same task were consolidated into “types” of problem. For example, “difficulty washing my face” and “I catch my eye or nose with my finger when washing my face” were grouped together as “wash self”.
The consolidated types of patient problem were mapped against the nine items that comprise the URAM scale. When a problem would have been captured on the URAM scale, a positive result was recorded (+). When a problem was not captured, a negative result was recorded (–). When a problem was interpreted as having some overlap with a URAM item, this was recorded as unclear (+/–).
As well as listing the types of indication for surgery, a question was posed to establish the relative importance that patients assigned to issues such as speed of recovery or better long-term outcome of treatment. The question asked them to rank the following characteristics of their ideal treatment:
Early recovery from surgery.
Better long-term outcome.
Surgeon’s recommended treatment.
The third of these options was provided to gauge whether patients deferred to the surgeon’s opinion or felt unable to prioritize speed of recovery against long-term outcome.
Results
There were 117 eligible patients. Six declined to participate and one was excluded due to Alzheimer’s disease that prevented her from being able to consent, leaving 110 patients. Eighty of the 110 patients were awaiting limited fasciectomy, 28 dermofasciectomy, and two needle aponeurotomy. Their mean age was 68 (range 34–90) years. Eighty-four (76%) were men, 69 (63%) were awaiting surgery to the right hand, and 67 (61%) were awaiting surgery to the dominant hand. The mean total passive extension deficit across the metacarpophalangeal and proximal interphalangeal joints of the fingers to undergo surgery was 68°.
In total, patients provided 278 problems, a mean of 2.5 per patient. Fifteen patients provided one problem, 22 gave two problems, and 73 specified three problems.
Once consolidated by the authors, there were 43 types of problem and 94 different combinations of these amongst the 110 patients. The most common problems, their frequencies, and capture by the URAM are shown in Table 2. Less common problems included five problems that were specified by four patients each: difficulty using computer keyboard (+/–), difficulty shaking hands (+), difficulty driving (–), difficulty clapping (+), and difficulty dressing oneself (–). Nine further indications were specified by three patients each: difficulty playing piano (+/–), difficulty using cutlery (–), difficulty using the computer other than the keyboard (e.g., the mouse) (–), difficulty with fine grip (+), difficulty writing (+/–), finger knocks things over (–), difficulty playing bowls (–), difficulty playing golf (–), and non-specific difficulty at work (–). Five more indications were common to two patients: difficulty playing snooker (+), difficulty applying cream to body (+), difficulty cutting fingernails (–), appearance of finger upsetting (–), and difficulty in stroking (+). There were also 13 indications specified by one patient each: paraesthesia (–), difficulty leaning on hand (+), difficulty placing hand into enclosed spaces e.g., washing cup (–), difficulty washing clothes (–), difficulty playing flute (–), difficulty using wheelchair (–), difficulty tying shoelaces (–), difficulty performing housework (–), unable to massage (+), difficulty cooking (–), concerned about finger swelling (–), dropping items (–), and difficulty sleeping (–).
The most common problems specified by patients.
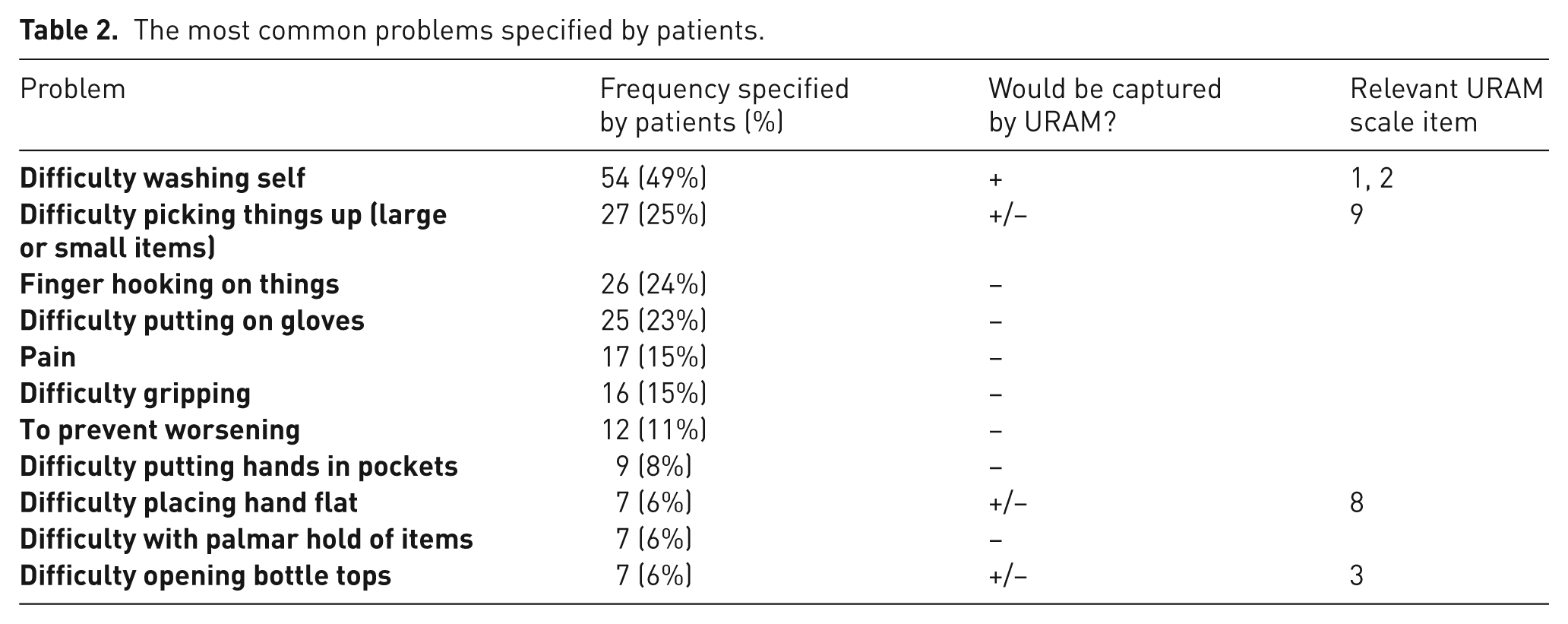
Seventeen patients (who had no comorbid painful condition) listed pain in the digit, despite pain not being considered a relevant symptom in Dupuytren’s disease by the team that designed the URAM. Two patients cited the unpleasant appearance of the digit as a problem, a symptom not assessed by the URAM or DASH, but which is captured by the PEM. Of the 15 patients who only cited one problem, the problem was difficulty washing oneself for five, concern about future deterioration for four, difficulty putting on gloves for two, and one each for difficulty gripping, difficulty holding items in the palm of the supinated hand (e.g., when given coins in a shop), difficulty dressing oneself, and difficulty writing.
URAM scale items would have directly assessed (+) nine of the 43 different types of problem obtained in this study. When frequencies of these nine indications were considered, URAM items would have captured 73 of the 278 problems specified by patients (26%). A further six of the 43 types of problem showed some overlap (+/–) with URAM items, accounting for a further 51 of the 278 (18%) problems. The remaining 28 indications showed no overlap with URAM items (–), and accounted for 154 of the 278 problems (55%).
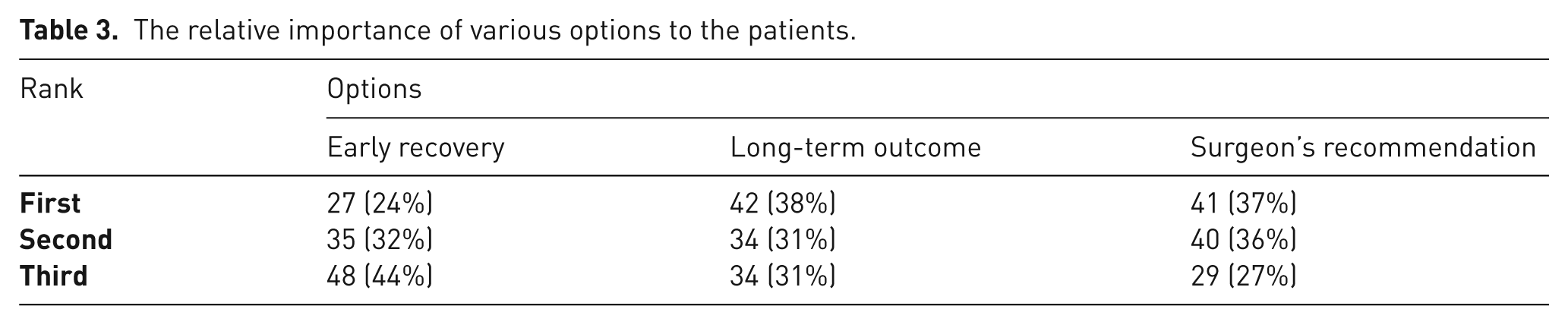
Long-term outcome was relatively important to patients, whereas achieving rapid early recovery was of less importance (Table 3).
The relative importance of various options to the patients.
Discussion
Understanding patients’ priorities is important when delivering patient-centred care, and our data describing priorities were intended to establish how patients view outcome of treatment, without being influenced by previous knowledge or opinions regarding specific treatment options. Our findings suggest that the long-term outcome of treatment may be more important than quick recovery to patients.
The URAM scale was designed specifically to assess Dupuytren’s disease, and its design methodology seems robust. However, our findings suggest that it fails to describe most of the problems that our patients experienced. This may be owing to the development of the URAM scale or to cultural differences between its developers’ patients and ours. The initial item-generation phase of the URAM involved input from only nine French patients, and thus may not have been generally representative of patients with Dupuytren’s contractures. Reduction of these items was then achieved by removing:
Items never performed by at least 5% of patients.
Items with a low spread of responses amongst pre-operative patients.
Items with low test–retest reliability.
Items with redundancy (defined as a high correlation coefficient with another item).
Items showing poor factor loading in an exploratory factor analysis.
Eliminating items never performed by 5% of the study population of patients might have removed problems that were very important to others. Additionally, removing items because of a small spread of responses obtained when administered to a small group of pre-operative patients may not be appropriate. Based on this methodology, a task that was commonly found to be severely limiting by all patients with the condition would be rejected.
Alternative PROMs to the URAM do exist and have been used to assess outcome of treatment for Dupuytren’s contracture (Ball et al., 2013). The most commonly used PROM has been the DASH. Like the URAM, it mainly assesses performance of specific, defined tasks, and so may also fail to capture the problems experienced by many patients.
The PEM outcome measure assesses symptoms and generalized, rather than specific, task performance (Macey et al., 1995). It also measures the psychological impact of the appearance of the hand. Therefore, the PEM might better capture the broad range of specific problems that patients experience.
An alternative solution would be to use individualized PROMs, which allow individual patients to specify tasks with which they have difficulty. Most of our patients had unique personal combinations of problems that caused them to seek treatment. A study from Sweden also reported a broad range of functional problems experienced by patients with Dupuytren’s contractures (Engstrand et al., 2009). Performance of these self-defined tasks improved significantly following surgery. This individualized approach to measuring outcome may represent a responsive, meaningful, patient-centred, and pragmatic endpoint.
Several other individualized tools exist, such as the Measure Your Medical Outcome Profile (MYMOP) (Paterson, 1996) and Canadian Occupational Performance Measure (COPM) (Law et al., 1990). These have been used in other clinical areas, but have not been validated for use in Dupuytren’s disease.
Measurements of finger joint angles (passive extension deficit, active extension deficit, and range of motion) have been used to measure outcome in many previous studies (Ball et al., 2013). However, angular measurements are not patient-centred outcomes. The data in this study suggest that some patients experience problems from their Dupuytren’s contractures that might not relate directly to loss of extension or reduced range of motion. For example, difficulty using computer keyboards and playing piano may relate to reduction of palmar span, and difficulty using cutlery and dropping items may relate to fine motor control rather than loss of extension.
There are limitations to our study. Our sample of patients included some who had already had treatment of Dupuytren’s disease in the past. The problems that they reported, and their expectations of treatment, might have been influenced by their previous experiences. However, as many patients with Dupuytren’s disease would be expected to undergo more than one procedure in their lifetime, this may increase the generalizability of our results. Another potential issue is that most of the patients studied were awaiting fasciectomy or dermofasciectomy, rather than needle aponeurotomy. Needle aponeurotomy has a quicker recovery time (van Rijssen et al., 2006), but is associated with more recurrence (van Rijssen et al., 2012). Patients who specifically sought quick recovery might have been referred elsewhere where this procedure was more likely to be offered. However, such a selection bias would not necessarily influence the symptoms reported by the patient.
It is thus clear that further work is required to optimize the assessment of patient-reported outcomes in hand surgery. Our data suggest that the face validity of the URAM needs to be reassessed and perhaps modified for general use. In this study, however, patients specified a broad range of problems that they experienced, which may prove hard to capture with any existing rigid scale based on task performance.
Footnotes
Acknowledgements
JN Rodrigues received educational support through a scholarship from the National Institute for Health and Care Excellence (NICE) during this project.
Conflicts of interests
None declared.
Ethical approval
This study was a minor element of a larger service evaluation project studying treatment outcome in Dupuytren’s disease. In keeping with UK National Research Ethics Service guidance, it is exempt from ethical approval. Nottingham University Hospitals NHS Trust guidance for the conduct of service evaluation projects was followed.
Funding
This work was supported by a BSSH Research Fellowship, Nottingham Hospitals Charity, and Nottingham Orthopaedic Walk.