
Abstract
Spontaneous flexor tendon rupture is a rare condition and the aetiology is not clear. We report 12 elderly Korean farmers with spontaneous flexor tendon ruptures. We found the rupture in the dominant hand in ten patients. A rupture in the little finger was found in all 12 patients (seven with both flexor tendons ruptured and five with only the profundus ruptured), in the ring finger in four patients (the profundus ruptured in all and both flexor tendons in two patients), and in the middle finger a partial rupture of the profundus in one patient. The tendons were ruptured close to the hook of the hamate. Repetitive friction between the flexor tendons and the hamate hook may cause the ruptures. The hamate hook was excised and the ruptured profundus tendons were reconstructed with tendon transfers with quite favourable functional recovery at follow-up of 1 to 2 years. The ruptured superficialis tendons were not reconstructed.
Level of Evidence IV
Introduction
Spontaneous tendon rupture has been defined as intratendinous rupture not due to any known pathologic condition (Boyes et al., 1960). Such ruptures are a result of intratendinous disruption and occur most frequently in the little finger (Naam, 1995). In the hand, a relationship between minor repetitive trauma and flexor tendon rupture has been proposed (Takami et al., 1993). Patients with physically demanding occupations, such as those requiring either repetitive heavy lifting or repetitive use of power grip, may be more susceptible to spontaneous tendon rupture over time. Rupture of the flexor tendon is usually sustained in the dominant hand and predominantly occurs in men over the age of 40 years (Bois et al., 2007; Naam, 1995).
We report the results of 12 elderly Korean farmers of spontaneous ulnar side flexor tendon ruptures.
Patients and methods
This study was approved by our institutional review board, and all patients provided informed consent. From March 2006 to December 2012, 18 patients with closed flexor tendon ruptures were treated surgically at one hand institute and one affiliated hospital, and were reviewed retrospectively. Data were obtained from the medical records. Standard posteroanterior and lateral radiographs of the wrist and carpal tunnel were taken to assess bony abnormalities such as previous fracture of the distal radius or carpal bones. Ultrasonography was also performed to confirm the tendon rupture and the location of the proximal and distal stumps (Lee et al., 2000). We enrolled the patients with a diagnosis of closed flexor tendon rupture. We excluded: (1) patients who could not be followed up for more than 12 months; (2) patients who had associated disease that could cause tendon rupture; and (3) patients who did not agree to enrol in this study. Two patients were excluded because they were followed up for less than 12 months, and one patient who had undergone surgery for a distal radius fracture. In addition, one patient had rheumatoid arthritis, one patient was diagnosed with Kienbock’s disease, and one did not agree to enrol in this study. Finally, 12 patients were enrolled in this study.
The patients were assessed at a mean of 17.7 months (range 12–24). The active ranges of motion of affected fingers were measured by two of authors (GJL and HJL) with a goniometer and the DASH scores were assessed by physician assistants.
Surgical treatment
All patients were treated surgically after the clinical diagnosis was established. Under general or brachial plexus regional anaesthesia with pneumatic tourniquet, the flexor tendons were explored through a zigzag incision over the involved fingers. The incision was initiated at the ruptured site, which was identified by preoperative ultrasonography, and was extended to the proximal and distal tendon stumps. Proximally, we incised the transverse carpal ligament and exposed the median nerve and the flexor tendons. At exploration, all flexor tendon ruptures were found in Zone III (Figure 1(A)). In all cases there was a lack of soft tissue coverage over the hamate bone, leaving a portion of this bone exposed and roughened (Figures 1(B), 2(A), and (B)). In some cases, the hook of the hamate was deformed with a bony spur (Figure 2(C) and (D)). We excised the hook of the hamate at the base and the exposed hamate bone was covered with soft tissue from around the hamate including part of the transverse carpal ligament to protect the repaired tendons (Figure 1(C)).
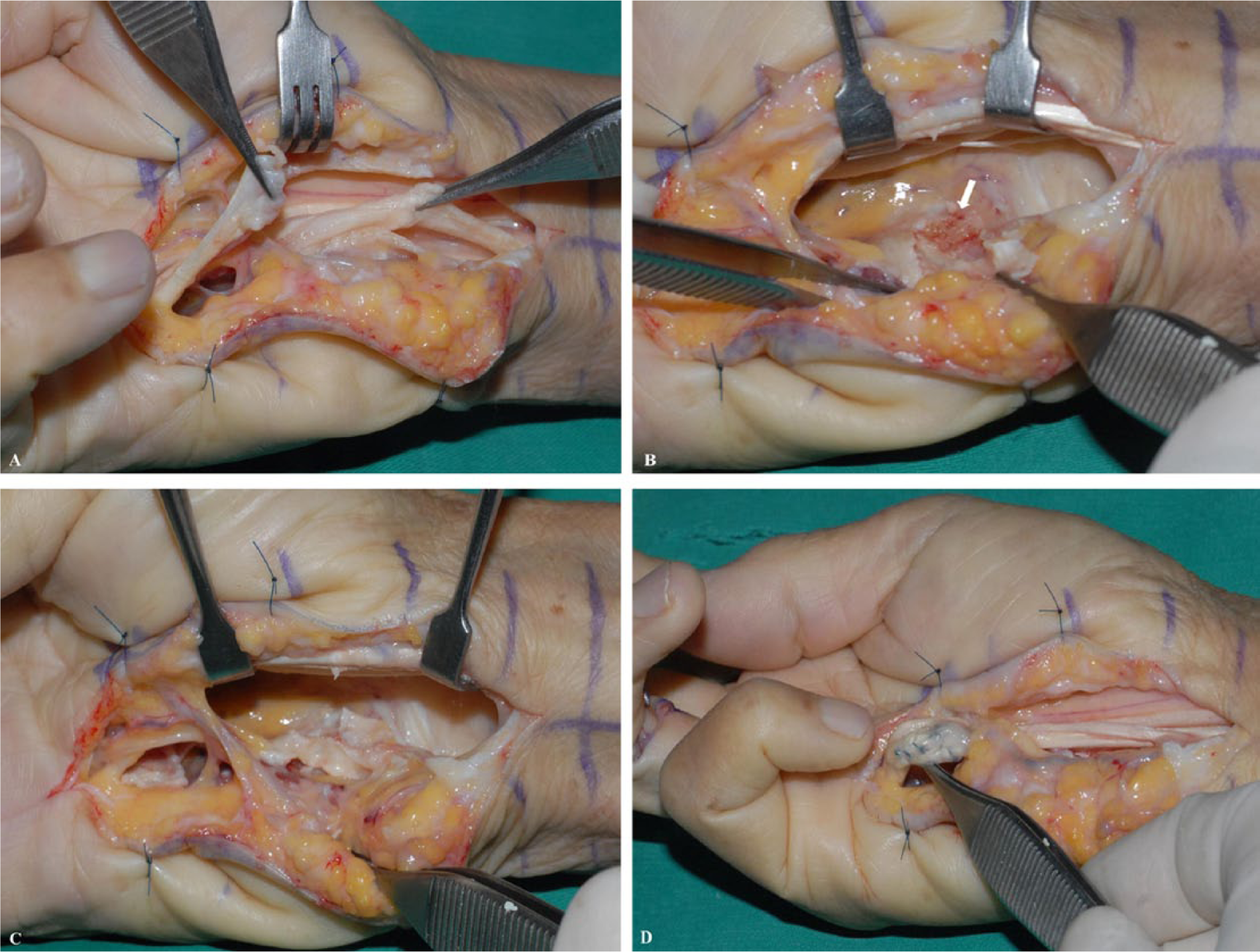
A 75-year-old, right-handed woman was assessed in our clinic 7 days after she felt a ‘pop’ in her right hand and she could not flex her fifth finger. (A) Proximal and distal tendon stump of the FDP tendon to fifth finger in Zone III. (B) Exploration of the floor of the carpal tunnel revealed there was a lack of fascial coverage over the hamate bone that was exposed and appeared roughened (white arrow). (C) The exposed hamate bone was covered with soft tissue from the transverse carpal ligament. (D) A FDS to fourth finger transfer to the FDP tendon to fifth finger was performed.
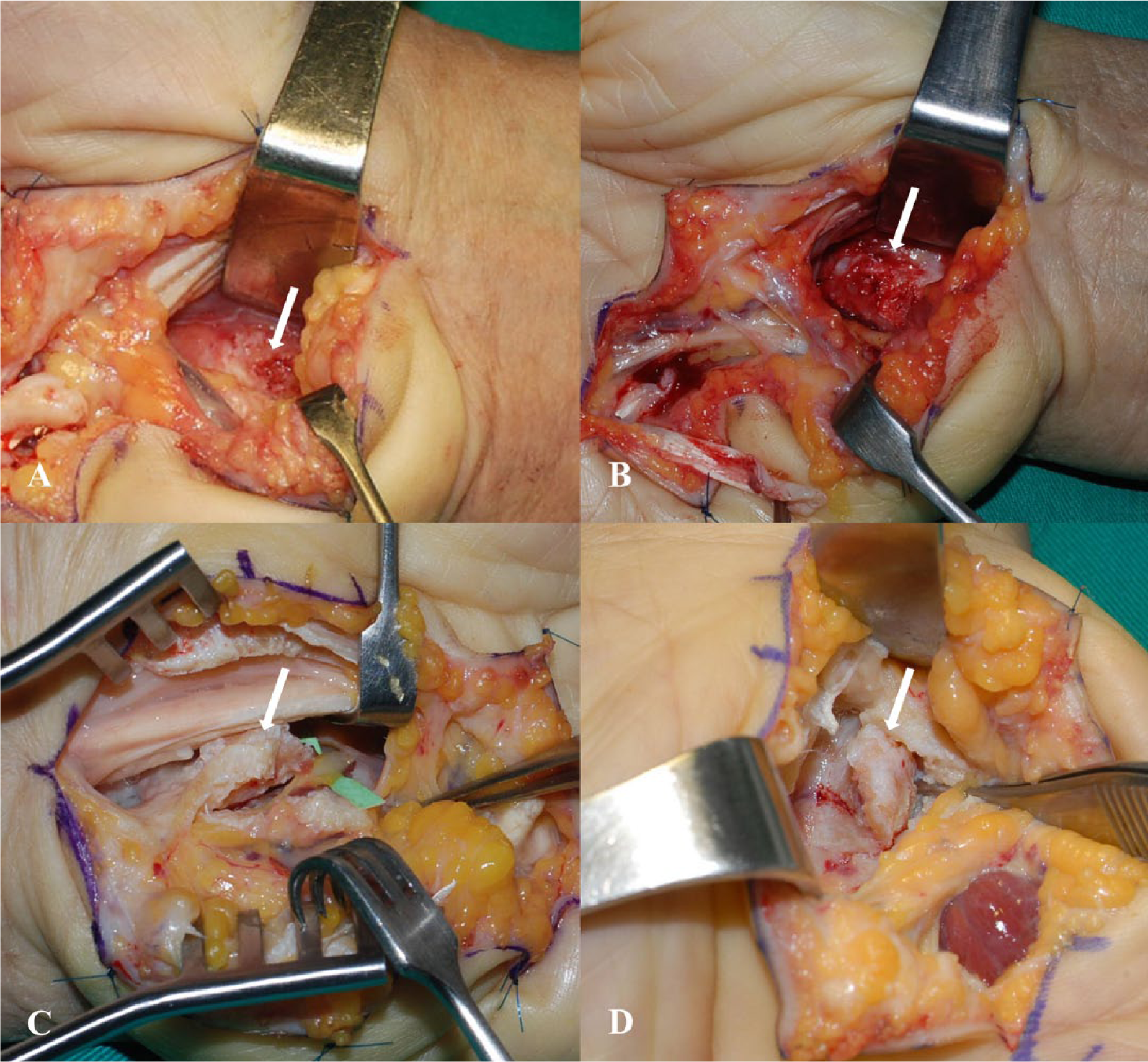
Various surgical findings. (A) and (B) There was a lack of soft tissue coverage over the hamate bone and the hamate bone was exposed. (C) and (D) The hook of hamate was deformed with a bony spur.
The choice of technique of tendon repair was based on the condition of the stumps of the ruptured tendons. In all cases, there appeared to be severe tenosynovitis around the proximal and distal stumps combined with tendon attrition. Thus, no tendon was repaired directly, and tendon transfer was used to reconstruct the ruptured flexor digitorum profundus (FDP) tendons. Ten patients had flexor digitorum superficialis (FDS) ruptures. The treatments included: one ring finger transfer to the FDP tendon of the little finger (Figure 1(D)); one interposition tendon graft using a segment of their palmaris longus tendon; one FDS tendon transfer from the middle finger to the ring finger FDP tendon; and one interposition tendon graft to the FDP tendon in the ring finger using the remnant of the FDS tendon of the middle finger. The transferred or grafted tendons were repaired with a Pulvertaft weave to allow early mobilization (Hashimoto et al., 2012). The A1 pulley was incised completely to prevent entrapment of flexor tendon.
Two surgeons, with an expertise in tendon surgery level III or IV (Tang, 2013), performed the tendon transfer procedures. After skin suture, the wound was dressed with loose-fitting gauze and a dorsal protective splint applied. At 3 days postoperatively, patients were started on a controlled passive motion method based on the Duran and Houser protocol (Duran et al., 1976). An active range of motion exercise was commenced 3 weeks postoperatively (Alam et al., 2014; Clancy and Mass, 2013; Tang et al., 2014). The dorsal protective splint was discontinued at 6 to 8 weeks postoperatively.
Results
There were two men and ten women with a mean age of 68 years (range 61–77) at the time of surgery (Table 1). The mean time from occurrence of the tendon rupture to surgery was 23 days (range 5–72); however, three patients could only provide an estimate of their time of injury, describing their symptoms as an insidious progression of decreased movement from the little to the ring finger. The mean follow-up time was 18 months (range 12–24). All patients lived in a rural area of South Korea and had worked for the majority of their lives in traditional farming. The rupture occurred in the dominant hand in ten patients. The flexor tendons to the little finger were involved in all 12 patients, the ring finger was involved in four patients, and the middle finger was partially involved in one patient. All ruptures occurred while patients were engaged in their usual farming activities, which demanded repetitive wrist motion combined with power grip. At the time of the tendon rupture, they were performing finger flexion against resistance. Seven patients recalled hearing or feeling a ‘snap’ or ‘pop’ in their finger. Three patients felt sudden sharp pain, and two patients did not know when the tendon rupture occurred.
Demographic data and surgical results.
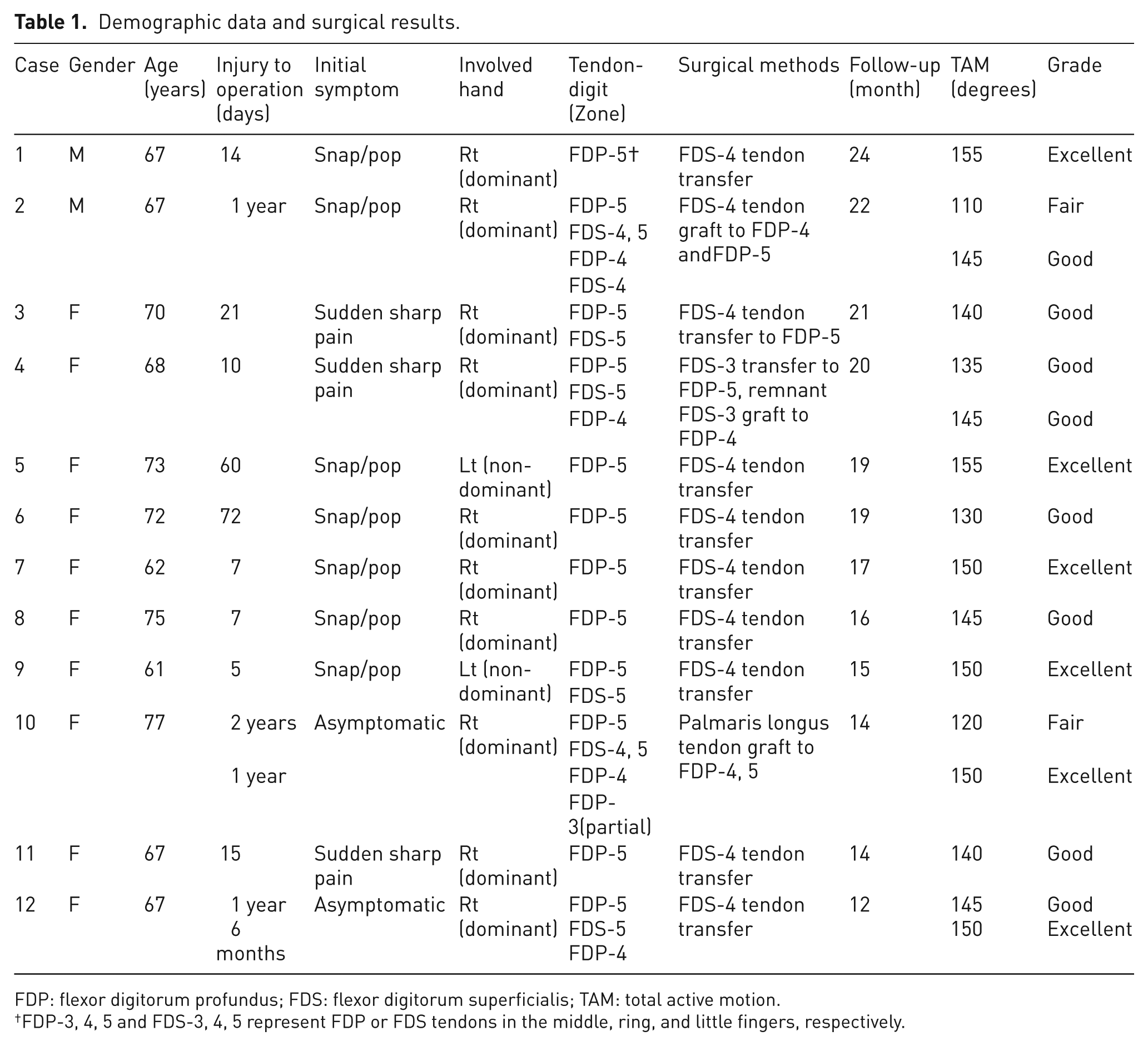
FDP: flexor digitorum profundus; FDS: flexor digitorum superficialis; TAM: total active motion.
FDP-3, 4, 5 and FDS-3, 4, 5 represent FDP or FDS tendons in the middle, ring, and little fingers, respectively.
By Strickland and Glogovac’s criteria (Strickland and Glogovac, 1980), six fingers in six patients were excellent, eight fingers in seven patients were good, and two fingers in two patients were fair. No finger in any patient was rated as poor. The DASH scores were 15.8 SD 9.7 points preoperatively to 6.3 SD 6.6 points at final follow-up. There was no complication of treatment.
Discussion
Spontaneous rupture of the digital flexor tendons is uncommon. Bois et al. (2007) reviewed the English literature over a 50-year period and reported a common pattern of injuries. The FDP tendon was involved in 82% of injuries, and the FDS tendon in 12%. The ulnar three digits were involved most commonly, with the little, ring, and middle fingers involved in 62%, 14%, and 10% of cases, respectively. A total of 80% of ruptures occurred in Zone III. The clinical history revealed that patients noted the sensation of a ‘snap’ or ‘pop’ in 68.4% of cases, a sudden sharp pain in 28.9% of cases, and no symptoms in 2.6% of cases. The ruptures occurred in the dominant hand in 65% of cases and 90% of cases are men. The mean age of the patients was 47 years. The choice of treatment was based on the length of time from injury and the location of the rupture. Most patients underwent direct tendon repair, some with an interposition tendon graft or a tendon transfer. Cavadas et al. (2015) have reported single stage vascularized FDS tendon grafting as an alternative treatment option.
In our study, 87.5% of fingers were rated as excellent and good in the Strickland–Glogovac criteria. Naam (1995) reported the surgical results of spontaneous flexor tendon ruptures in Zones II and III had good to excellent range of active motion of the digits. In cases of open injured flexor tendon in Zone III, Al-Qattan (2011) showed 90% of injured fingers had excellent or good outcomes using the Strickland–Glogovac criteria.
Though the FDP tendon is about 50% stronger than the FDS tendon, we found that all spontaneous flexor tendon ruptures involved the FDP tendon, most frequently the FDP tendon to the little finger. This is probably because the FDP tendons are deeper and run closer to any bone spikes. Imbriglia and Goldstein (1987) showed that the little finger transmits more of the force through the FDP tendon during flexion grip, which may cause it to be susceptible to degenerative changes over time. Imai et al. (2004), reporting on the histology of ruptured tendons, revealed an abundant regenerative fibrous tissue deeply infiltrating into the affected tendon suggesting a chronic attrition of the tendon fibres. Patients with physically demanding occupations may be more susceptible to spontaneous tendon ruptures over time. The majority of patients in previous studies were engaged in occupations that required repetitive heavy lifting or repetitive use of power grip (Bois et al., 2007; Imbriglia and Goldstein, 1987; Naam, 1995). Repeated minor trauma has also been shown to be associated with rupture of the FDP tendon (Takami et al., 1993).
All patients worked in dry-field or rice-field farming. In Korea, a large proportion of inhabitants in rural areas are elderly women. They frequently work in small-scale agriculture using hand hoes and small sickles rather than farming machinery. To use these tools, repetitive movements between full wrist flexion with ulnar deviation and full extension with radial deviation with power grip are required. In the position of full wrist flexion with ulnar deviation, the FDP tendons of the ulnar digits are deviated to an acute angle at the hamate in the carpal tunnel. Moreover, repetition of these movements can produce friction between the flexor tendon and the surface of the hamate leading to attrition of both the tendon and the surface of hamate.
During surgery, we found that the tendons were ruptured close to the hamate hook and the hamate was exposed and appeared roughened without a covering of soft tissue or a deformed hamate with bony spur in all cases. Bois et al. (2007) reported one case with similar findings in exploration of the floor of the carpal tunnel. Anatomically, when the wrist is fully flexed in combination with ulnar deviation and power grip, it is Zone III of the FDP tendon that rubs against the hamate. This may also explain why the site of rupture was located in Zone III in our patients. To reduce the risk of recurrence, we excised the hook of hamate in all our patients.
We found that all patients suffered their first tendon rupture in the little finger. The incidence of rupture of the flexor tendons in the ring finger is secondary to that in the ring finger. Because the FDP tendon of the little finger is intimately linked to the hamate, it is likely that the FDP tendon of the little finger will rupture first, followed in sequence by the FDS tendon of the little finger, and the FDP tendon of the ring finger.
Our study has several limitations. First, this study was retrospective, thus patients were reviewed by their medical records. Second, the limited number of patients in the case series meant that we could not confirm the aetiology. Third the follow-up was short.
In our case series, we noted spontaneous flexor tendon ruptures to be more common in older females than in younger males. We choose tendon transfer because of severe tenosynovitis with tendon attrition. Our follow-up data show that a good functional recovery can be expected when these patients are treated surgically.
Footnotes
Conflict of interests
None declared.
Ethical review committee statement
SNUB IRB protocol number: H-1304-067-482
All conditions of approval previously established by SNUH IRB for this research project continue to apply.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.