
Abstract
The value of post-operative radiographs following stabilization of Arbeitsgemeinschaft für Osteosynthesefragen (AO) type A distal radius fractures with volar locking plates is unclear. We examined the value of post-operative radiographs of type A fractures treated with volar locking plates. A retrospective review was performed on all AO type A distal radius fractures treated with volar locking plates between 2007 and 2010 at two institutions. A total of 158 patients receiving 446 sets of post-operative radiographs were included. Reviewing all clinic, emergency, and operative notes, we found that 94% of radiographs were performed as routine follow-up, with no set of post-operative radiographs demonstrating findings of hardware/fracture site complications. All cases requiring further workup or interventions were heralded by patient complaints. Routine post-operative radiographs following volar locking plates for extra-articular distal radius fractures did not demonstrably alter clinical decision making; this is an area where a reduction in resource utilization would not seem to alter clinical quality care, but further studies with larger populations are needed to establish the incidence of radiographic problems prior to symptom occurrence.
Introduction
Internal fixation of distal radius fractures with volar locking plates (VLP) is increasingly common; arguments in favour of this technique include the stability of the fracture/implant construct, earlier return of function, and low complication rates (Capo et al., 2009; Dahl et al., 2012; Dillingham et al., 2011; Rozental and Blazar, 2006). In particular, nonunion rates for distal radius fractures are exceedingly low; risk factors include the severity of injury, loss of metaphyseal bone, and comorbidities such as tobacco use and alcohol abuse (Capo et al., 2009; Dahl et al., 2012; DeBaere et al., 2007; Khamaisy et al., 2011; Rozental and Blazar, 2006). The published stability of VLP constructs for even comminuted fractures makes failures of fixation uncommon (DeBaere et al., 2007; Mignemi et al., 2013; Segalman and Clark, 1998).
Reducing the cost of medical management, while maintaining quality of care, has become a guiding principle in health care reform (Brody, 2010). In a field that is highly reliant on medical imaging, orthopaedic surgeons can reduce costs by identifying imaging practices that add limited clinical value. The cost-effectiveness and clinical relevance of related radiographic practice, however, remains an open question. Radiographs are taken at most clinic visits following surgical fixation of fractures to evaluate healing and determine loss of alignment or hardware complications.
The aim of this study was to assess the value of routine post-operative radiographs for patients following VLP for type A distal radius fractures.
Methods
AO type A distal radius fractures treated with VLP between 2007 and 2010 at two level-one trauma institutions were retrospectively reviewed under an Institutional Review Board (IRB) approved protocol. The study was limited to AO type A distal radius fractures due to their stability following VLP and low fracture site or hardware complication rate (Capo et al., 2009; Chung and Spilson, 2001; Dahl et al., 2012; Dillingham et al., 2011; Rozental and Blazar, 2006). Billing databases were reviewed for cases using Current Procedural terminology (CPT) code 25607 (‘Open treatment of distal radial extra-articular fracture or epiphyseal separation, with internal fixation’). We excluded 54 patients that had additional indications for serial radiographic evaluation, e.g. open fracture (18), distal both-bones forearm fracture (associated distal ulna fracture without ulnar styloid fracture) (25), skeletal immaturity (9), and polytrauma (2). A total of 21 patients who failed to follow up were also excluded, for a total of 75 excluded patients. A total of 158 patients were included in the final data set, receiving 446 sets of post-operative radiographs over 534 clinic or emergency department visits (Table 1). Surgical fixations were performed by 14 different surgeons with either Synthes (Paoli, Pennsylvania, USA) 2.4 mm Variable Angle LCP Two-Column Volar Distal Radius Plates or DePuy (Warsaw Indiana, USA) DVR Anatomic Plates. Intra-operative digital images of the final fixation were saved electronically. Patients were followed at intervals and radiographs obtained according to the individual surgeon’s practice.
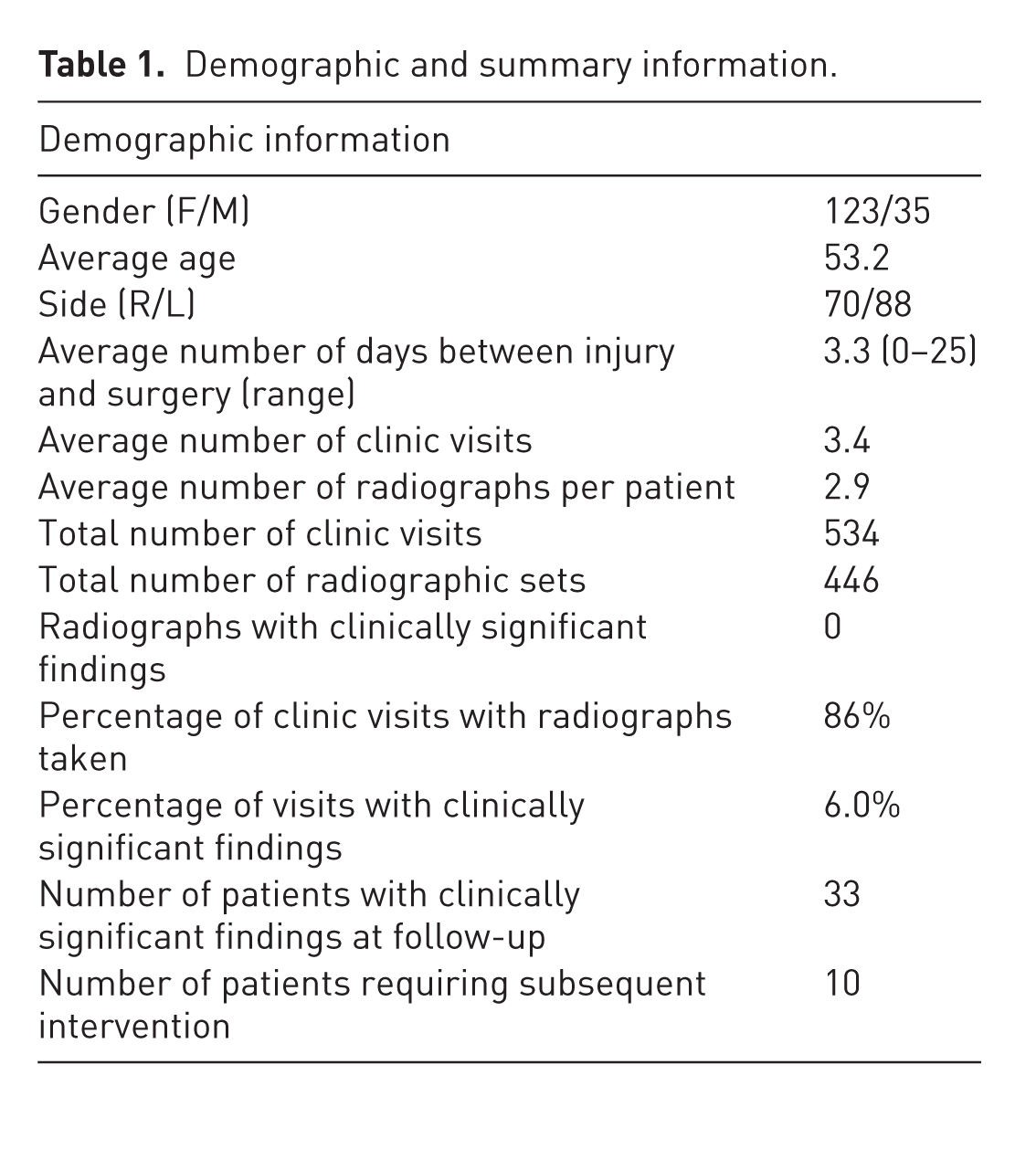
Demographic and summary information.
All post-operative clinic or emergency department notes were reviewed. We included all patient complaints and exam findings as ‘positive’ irrespective of whether the reviewer felt that these findings raised a significant concern of a complication. For example, clinic notes describing ‘persistent ulnar sided wrist pain’ or ‘crepitation of the tendons over the plate’ were denoted as having ‘positive clinical findings’. In other words, any complaint by the patient or any exam findings from erythema to mild tenderness on palpation that the clinician felt was outside of the expected post-operative course was considered ‘a clinical finding’. The radiographs ranged from one to three views of the operative extremity. All post-operative radiographs were reviewed by two independent observers blinded to both the patients’ clinical presentation and the radiology report. Images that demonstrated hardware or fracture site complications were denoted as having ‘positive radiographic findings’. Patients were considered to have a clinically associated intervention if they incurred a new diagnosis in the operative extremity (e.g. carpal tunnel syndrome) or required nonstandard follow-up or any procedural intervention (e.g. removal of hardware).
Statistical analysis
P-values were calculated using the chi-square test in Statistical Package for the Social Sciences (SPSS) and were considered significant if the two-tailed value was less than 0.05. If contingency tables had less than five expected values in one category, then Fisher exact testing was applied. Based on a reported radiographic complication rate of 10% in a cohort of dorsally displaced, unstable distal radius fractures, and a much lower expected rate of complications in our population (1%), we performed a power analysis determining that 158 patients was a sufficiently large sample size to correctly reject the null hypothesis value with a significance level of 0.05 and a power of 0.8.
The study was approved by the hospital IRB.
Results
A total of 158 patients with 446 post-operative radiographs were identified and followed-up for a mean of 4.2 months (range 6 weeks to 4 years). Radiographs were obtained at 86% of clinic visits (Table 1). None of the 446 post-operative radiographs demonstrated evidence of hardware or fracture site complications, as evaluated by either independent reviewer or the radiology report (Table 1) (95% CI 0–0.0082). There was no loss of reduction, delayed union, or nonunion in any patients. Both observers independently agreed that all patients came to radiographic union, and no set of radiographs demonstrated loss of fixation or change in post-operative alignment.
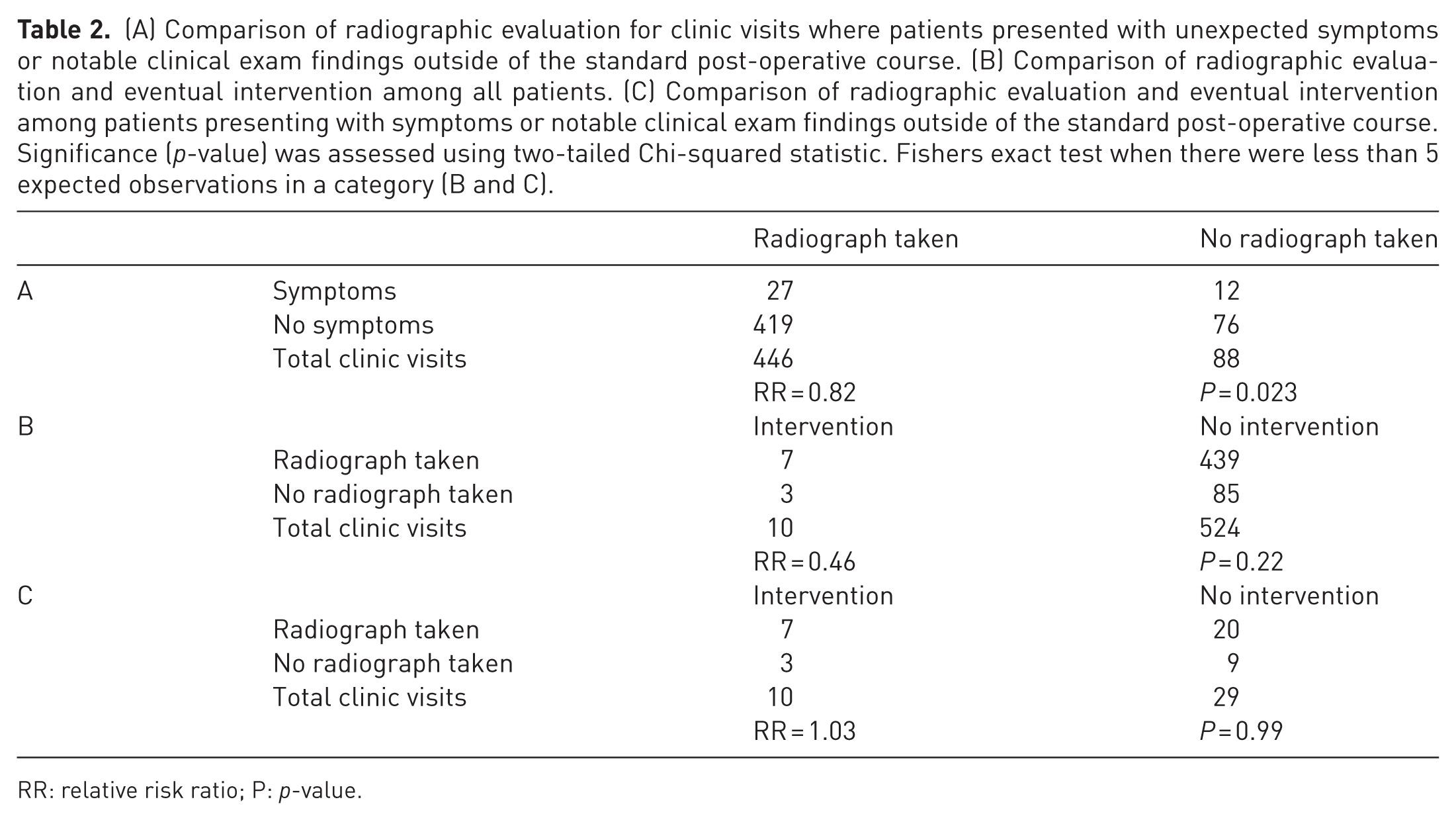
All patients had at least one set of post-operative radiographs obtained with a mean of 2.9 sets (range 1–6) of radiographic per patient (Table 1). There was no association between radiographic evaluation and the need for further intervention (Table 2, p = 0.22). Patients with positive clinical findings or complaints were significantly less likely to have radiographs than those without (85% versus 69%, p = 0.023). In other words, 94% of post-operative radiographs were obtained independent of positive clinical findings or patient complaints and led to no change in medical decision making.
(A) Comparison of radiographic evaluation for clinic visits where patients presented with unexpected symptoms or notable clinical exam findings outside of the standard post-operative course. (B) Comparison of radiographic evaluation and eventual intervention among all patients. (C) Comparison of radiographic evaluation and eventual intervention among patients presenting with symptoms or notable clinical exam findings outside of the standard post-operative course. Significance (p-value) was assessed using two-tailed Chi-squared statistic. Fishers exact test when there were less than 5 expected observations in a category (B and C).
RR: relative risk ratio; P: p-value.
A total of 33 patients (21%) presented to clinic or the emergency department with symptoms that merited further clinical work-up; 24 of these had radiographs taken of their operative forearm or wrist at the time. Ten patients had clinical examination findings or symptoms that justified intervention (Table 3), eight of which required additional surgery: four carpal tunnel releases, three operations to remove painful plates and screws, one cortisone injection for de Quervain’s syndrome, and one incision and drainage of an infected post-operative hematoma. There was also one extensor pollicis longus (EPL) rupture managed nonoperatively based on patient preference.
Summary data of cases requiring intervention. Post-operative day corresponds to the number of days after surgery that the patient presented to clinic or the emergency room with the noted complaint.
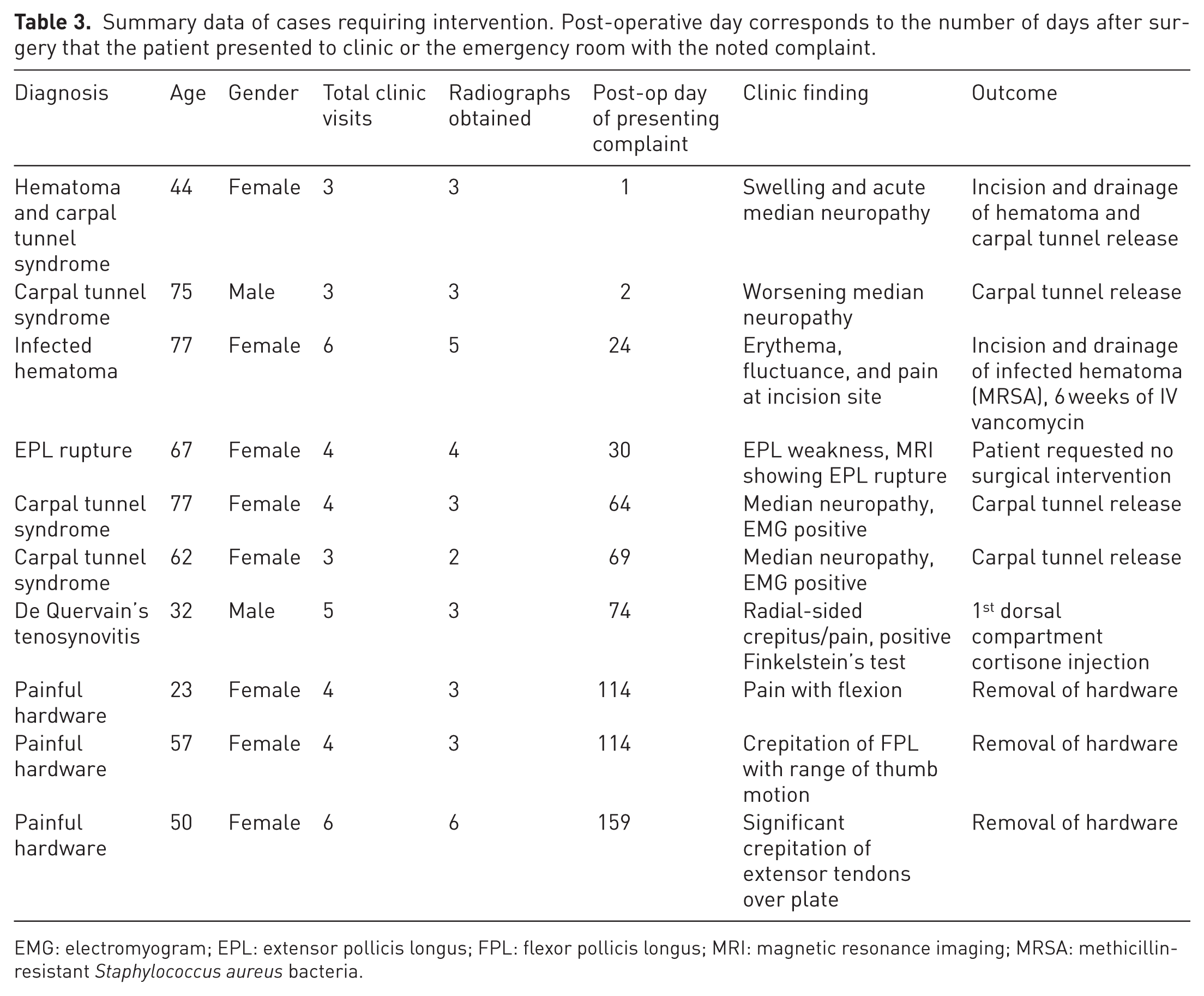
EMG: electromyogram; EPL: extensor pollicis longus; FPL: flexor pollicis longus; MRI: magnetic resonance imaging; MRSA: methicillin-resistant Staphylococcus aureus bacteria.
Finally, 339 (76%) radiographs were taken within the first 90 post-operative days, with 135 (30%) obtained within the first 2 weeks (Figure 1). Although there was no standard protocol regarding timing of follow-up and radiographic evaluation, the most common radiographs were noted at 2 weeks and 6 weeks after surgery (Figure 1). Of the ten patients sustaining complications, seven of them presented with these symptoms prior to 90 days following their index surgery. The three patients with symptomatic hardware eventually requiring removal of hardware all presented with symptoms more than 110 days after their initial operation (Table 3).
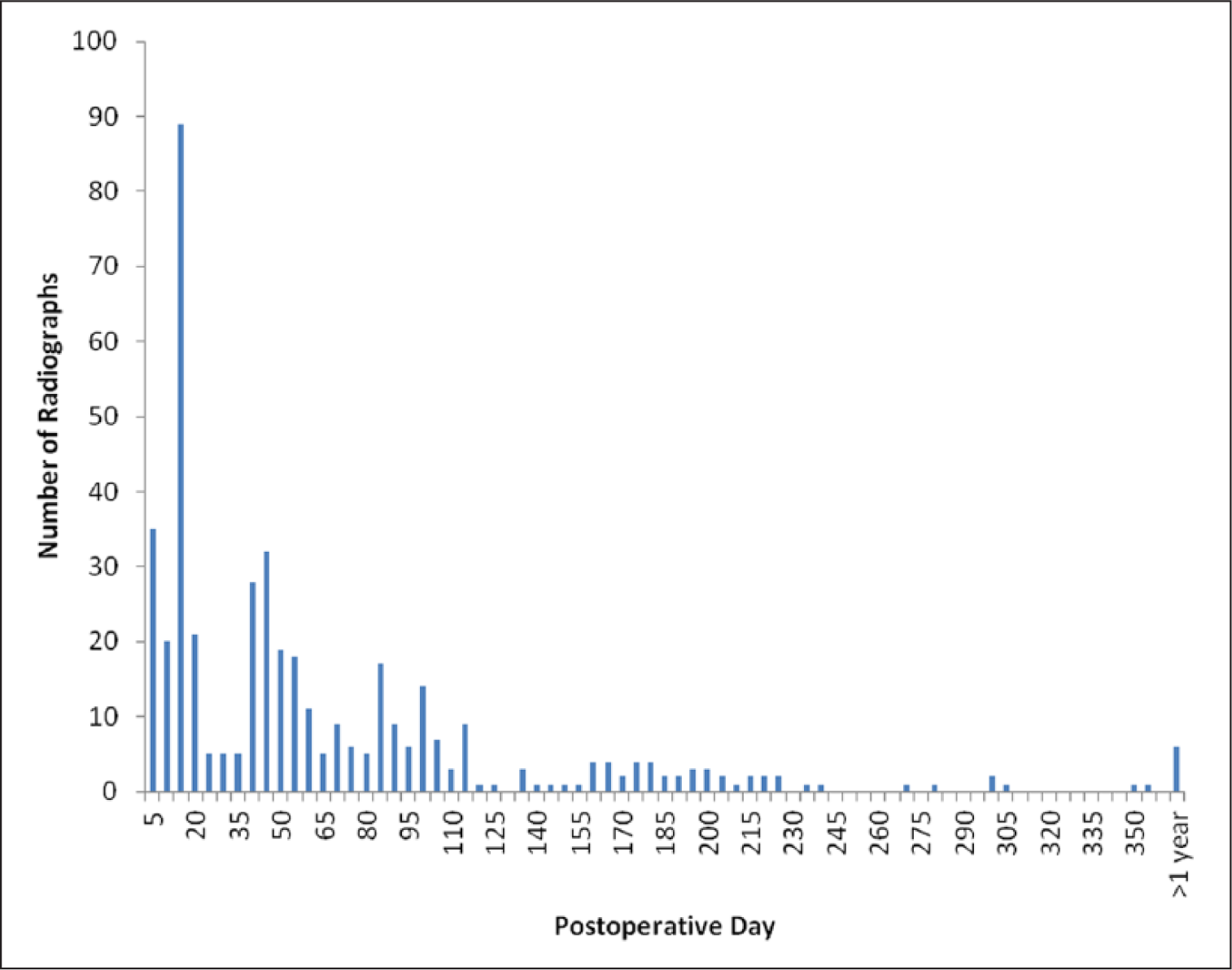
Histogram depicting total number of radiographs and the number of days following surgical fixation.
Discussion
Post-operative radiographs are nearly always obtained after fracture fixation. There are no published clinical guidelines regarding post-operative radiographs after distal radius fracture fixation. We investigated the value of post-operative radiographs in AO type A distal radius fractures treated with VLP as a model because of the very low probability of nonunion or hardware complications. AO B- and C-type injuries were excluded as being potentially less stable (Rozental and Blazar, 2006). The ten cases with complications in our series had no evidence of unexpected radiographic findings and the problems in all of these patients were heralded by patient-reported symptoms or examination findings. Thus none of the radiographs obtained during routine clinic visits indicated complications, and in the cases of patient complaints or positive physical exam findings, radiographs served primarily to rule out significant hardware or fracture-related diagnoses. We found that over 94% of the post-operative radiographs in our series were not associated with positive clinical findings and did not significantly contribute to clinical decision making.
These results suggest that practice can be changed to reduce cost, exposure to ionizing radiation, and length of follow-up visits (Figure 2). Our data indicate that a very small percentage (5.9% in our series) of post-operative radiographs produced findings that impacted decision-making. All of those radiographs contributed to clinical care by ruling out significant hardware or fracture complications, thereby serving as a reassurance that healing was following the expected course. Our data also demonstrate two periods of increased post-operative radiographs at or around 2 weeks and 6 weeks, corresponding to common intervals for post-operative follow-up. However, our complications were initially noted over a wide time period (range 1 to 159 days), therefore, the detection of complications following VLP of type A extra-articular distal radius fractures is reliant primarily on assessing patient complaints and physical examination and is unaided by the use of routine post-operative radiographs.
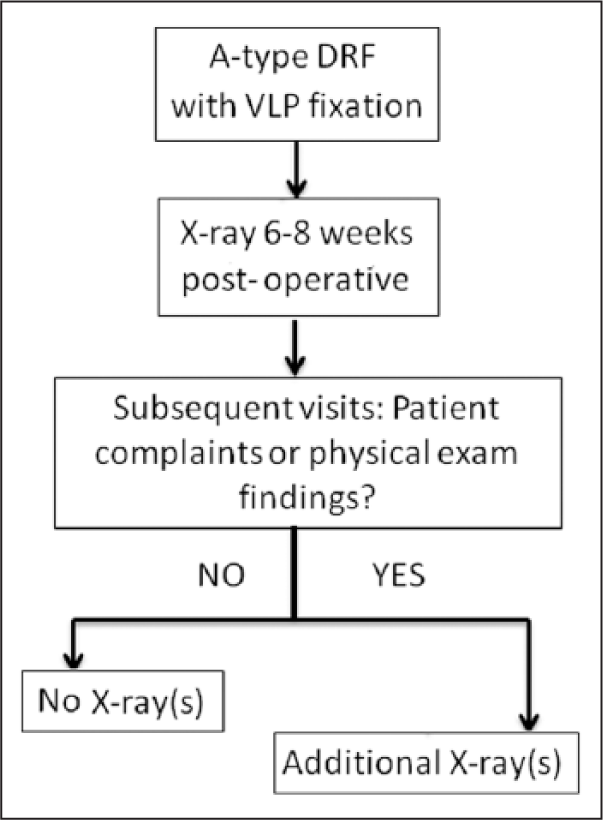
Proposed protocol for postoperative radiographs for A-type distal radius fractures treated with VLP.
While our data suggest that the value of post-operative radiographs in screening for complications is low, we would not argue for the elimination of radiographs altogether. Unassessed by our design are the potential changes in post-operative management that a surgeon and/or a patient may delay until radiographic union. For example, a surgeon might not allow an injured worker to return to heavy manual labour or a physically demanding sport until radiographic union. As such, a single set of post-operative radiographs to document post-operative alignment and healing is reasonable, after which additional radiographs should be obtained based on the presence of symptoms or examination findings departing from the standard post-operative course. Negative radiographic findings are of diagnostic importance and particularly in the case of patient complaints or concerning exam findings, radiographs should frequently be considered as part of the clinical workup. In our series, this recommended protocol would have led to a reduction in the average number of radiographs for each patient by 2.3 fold (1.25 versus 2.84, p < 0.0001) and would correspond to 56% fewer sets of radiographs performed (252 fewer radiographic sets in our data set).
There are several limitations to this study. This is an observational and retrospective design with a limited sample size. In particular, there were only ten complications, all of which related to issues that are undetectable on radiograph (i.e. carpal tunnel syndrome, painful hardware, or acutely infected hematoma). The psychological benefits to the patient and reassurance for the surgeon of a radiograph documenting union and a lack of radiographic complications are not addressed by our study. Given that no radiographic complications (such as nonunions and malunions) were observed, a much larger sample would be required to establish an incidence of radiographic complications in this population. Another limitation is that the data assesses the association of clinical presentation and radiographs across the same 158 patients. Lastly, this study was limited to the results of 158 patients. It is possible that a very rare complication, on the order of 1 in 500 or 1000 patients, would need a much larger study group to identify. Therefore, readers should not interpret our study as ruling out the possibility of complications that are very infrequent.
Segalman and Clark reported 12 cases of nonunion after retrospective review of their institution’s operative records for a 25-year period (Segalman and Clark, 1998). Thus, while increasing the sample size, or even extending the length of study, would potentially lead to an increased chance of observing these radiographically evident complications, this remains an exceedingly rare event. Retrospective investigation into the clinical course and radiographic findings of patients with nonunion or subsequent malunion might serve to discern whether these events are indeed heralded by patient complaints before radiographic evidence. Of the few case reports describing the clinical presentation of patients with nonunion after distal radius fixation, each patient presented with pain at the operation sites and was subsequently evaluated radiographically (Cao and Ozer, 2010; DeBaere et al., 2007; Harper and Jones, 1990).
This study only included AO type A fractures. While this subset of distal radius fractures was intentionally selected as the most stable construct after VLP, our data does not allow extending these findings to more complicated fracture patterns. Recent outcomes studies have suggested similar functional and pain scores for patients with type-A distal radius fracture (DRF) as compared with those with simple intra-articular (AO B-type) DRF treated with VLP (Souer et al., 2011). Furthermore, Bolmers et al. have found that patients undergoing surgery for B- and C-type fractures have comparable functional outcomes in the long-term (Bolmers et al., 2013). These observations warrant a further study examining the value of post-operative radiographs in AO B-type and C-type fractures.
Since our data indicates that routine post-operative radiographs do not significantly affect clinical management of AO type-A DRFs treated with VLP, we find that routine post-operative radiographs for this fracture type are obtained more frequently than necessary. We suggest that obtaining one set of radiographs post-operatively would significantly limit exposure to ionizing radiation and clinical costs, with subsequent radiographs obtained only for complaints or examination findings outside the normal post-operative course.
Footnotes
Author note
Our study was performed under a protocol approved by the Partners Human Research Committee.
Conflict of interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.