
Abstract
The purpose of this study was to report our experience of partial capitate shortening in seven patients with a median 38 months follow-up. Staging was made by the Lichtman classification system and stage II and III-A patients were included in the study. The mean age was 34 years (range 22–52). Patients were assessed for pain, range of motion, grip and pinch strength, and satisfaction was recorded using a scale between 0 and 4. All these parameters showed improvement after surgery. The Lichtman stage, lunate height index and carpal height index were determined radiographically. Magnetic resonance images of the wrist were studied for lunate revascularization at the final follow-up and occurred in all patients. According to our study, partial capitate shortening seems an effective treatment for Lichtman stage II and III-A patients.
Level IV case series study.
Introduction
The objective of operative treatment for Kienböck’s disease is to decrease the compressive loading on the lunate to allow revascularization (Allan et al., 2001; Cross and Matullo, 2014). Several surgical options, including joint levelling procedures (radial shortening or ulnar lengthening), partial carpal fusions, and total or partial capitate shortening (PCS) osteotomies have been advocated (Beredjiklian, 2009; Cross and Matullo, 2014; Lutsky and Beredjiklian, 2012; Matsuhashi et al., 2011; Viljakka et al., 2014; Werber et al., 2013). These procedures are used in Lichtman stages II and III-A, before significant fixed deformity has occurred. Although the efficacy of most of these procedures has been shown either by biomechanical or clinical studies, there have been only two case reports of PCS, which was found to be an effective procedure to unload the lunate (Moritomo et al., 2004; Wollstein et al., 2013). The purpose of this study was to assess the safety and efficacy of PCS in seven patients followed for a median 38 months.
Patients and methods
The series consisted of seven patients with a mean age of 34 years (range 22–52). There were four male and three female patients and the dominant hand was affected in five. The chief complaint of the patients was wrist pain during activity, at the time of admission. None of the patients had a history of trauma.
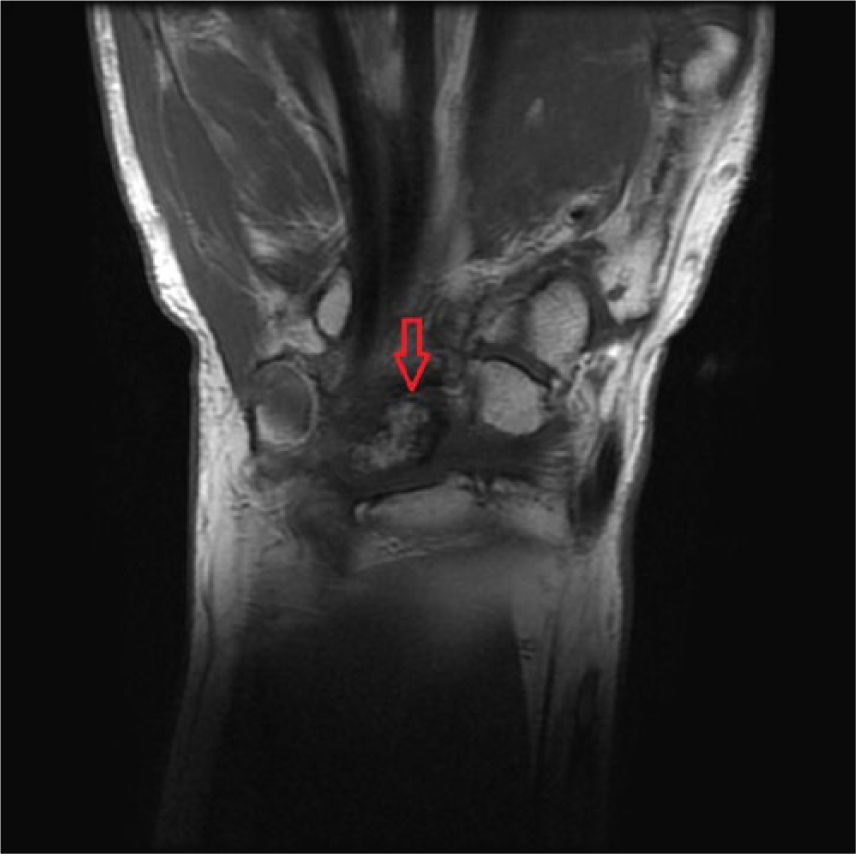
The diagnosis was made by plain radiography and confirmed by magnetic resonance imaging (MRI). Staging was made by the Lichtman classification system and stage II and III-A patients were included in the study. This means that there was lunate sclerosis (stage II) (Figure 1) or lunate collapse with normal carpal alignment and height (stage III-A) (Lichtman et al., 2010). MRI appearances confirmed Kienböck’s disease, with markedly decreased signal intensity on T1-weighted images (Figure 2).

Posteroanterior radiograph of wrist with sclerosis of lunate.

T1-weighted magnetic resonance image showing Lichtman III-A Kienböck’s disease.
The operations were carried out by the same surgeon (M.S.) as described by Moritomo et al. (2004). Using regional or general anaesthesia and under tourniquet control, a 3-cm dorsal longitudinal incision was made over the capitate, the extensor tendons were retracted and capsule was incised longitudinally to expose the capitate. The osteotomy of the capitate was done in a ‘reverse L’ manner: the first osteotomy line lay longitudinally on the ridge and the second lay transversely, 2 to 3 mm distal to the edge of the articular surface of the lunate fossa of the capitate forming a 90° angle. A second transverse cut was made parallel and 2 mm distal to the first transverse cut (Figure 3(A)). The resulting mobile segment of the capitate was moved distally, and compressed against the distal segment using a headless cannulated compression screw (Figure 3(B)). The dorsal capsule was closed before skin closure.
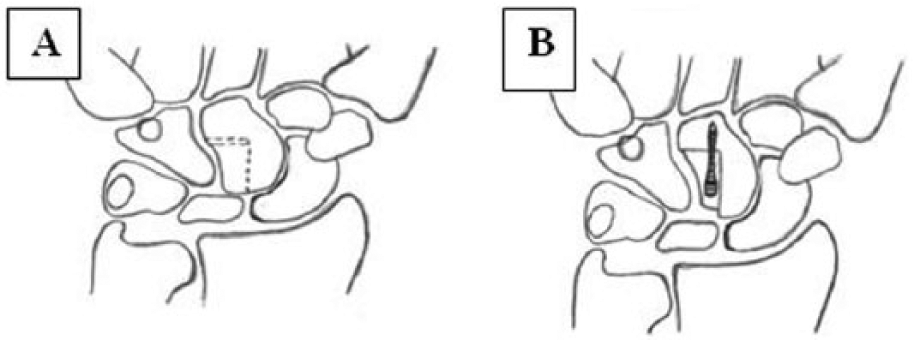
Diagram of the PCS osteotomy. (A) Osteotomy lines. (B) After shortening and fixation of the osteotomy with a screw.
A short-arm cast is applied for 4 weeks. Then light activities were allowed up to solid healing of the osteotomy site.
Clinically, patients were assessed for pain, range of motion, grip and pinch strength. Pain was evaluated by a visual analogue score between 0 and 10 (0, no pain; 10, the most severe pain). Range of motion was measured using a universal goniometer. Grip strength was measured by a Jamar dynamometer (Model SH 5001, Saehan Corporation, Masan, South Korea) and pinch strength was measured by a pinch meter (Model SH 5005, Saehan Corporation). Also, the patients’ satisfaction was recorded by a modified Gay scale (Gay et al., 2009) between 0 and 4. In this system 0 means ‘not satisfied’, 1 ‘no change’, 2 ‘slightly satisfied’, 3 ‘satisfied’ and 4 ‘very satisfied’.
The Lichtman stage, lunate height index according to Ståhl (1947) and carpal height index according to Youm et al. (1978) were established from radiographs.
Each patient underwent pre-operative and post-operative MRI. Magnetic resonance images of the wrist were assessed for lunate revascularization by an expert radiologist at the final follow-up. Standard sequences were obtained for all scans. Also, fast-spin echo (FSE) T1-weighted coronal, FSE T1-weighted FS coronal, axial and sagittal images were obtained after injection of gadolinium-diethylene triamine pentacetate. Positive revascularization of the lunate was defined as an increase in bone marrow signal intensity on MRI sequences. Additionally, the contrast enhancement within the lunate was similar to that of the other carpal bones in successful revascularization.
The study protocol was approved by the local ethical committee of Ataturk Training and Research Hospital.
Results
The patients were followed-up for a median of 38 months (range 15–46) after the operation. The Lichtman stage changed in one patient from III-A to III-B, and in another from II to III-A. The mean pre-operative visual analogue score was 8.2 (range 7–10) and the post-operative visual analogue score was 3.1 (range 1–5). The mean patient satisfaction score was 3.4 (range 3–4) over the 4-point Gay scale. The mean time to return to work was 5.5 months (range 1.5–12). The mean grip strength in the operated hands was 73% (range 26–100), palmar pinch was 83% (range 71–100), tip pinch was 88% (range 50–100) and key pinch was 91% (range 62–100)% when compared with the contralateral unaffected side. Inhomogeneous enhancement of the lunate was detected on the post-operative magnetic resonance images in all patients. Partial and patchy normalization of the signal intensity of the bone was detected on T1-weighted magnetic resonance images in all patients (Figure 4).
MRI showing revascularization.
Discussion
Operative treatment of Kienböck’s disease is designed to decrease the compressive loading on the lunate in order to prevent collapse and allow revascularization (Cross and Matullo, 2014; Günal et al., 2005; Moritomo et al., 2004). Although good or excellent results have been reported for joint levelling (Altay et al., 2008; Rodrigues-Pinto et al., 2012) and several types of partial fusions, capitohamate fusion seems to increase the loads borne by the lunate (Günal et al., 2005; Horii et al., 1990; Short et. al., 1992). It has been shown that if the loads used in experimental studies are increased to the level that occurs in forceful grasping, that is about 200 N (Cooney and Chao, 1977), then the joints between the carpal bones collapse and the loading pattern on the lunate after partial fusions is the same as in the normal wrist (Günal et al., 2005). Theoretically, this is not true for PCS because the ridge (Figure 3(B)) prevents collapse and no load is transmitted from the capitate to the lunate (Kataoka et al., 2012; Werner et al., 1992). So, PCS seems to be the only procedure that can unload the lunate independently from the loads applied to the wrist.
According to Horii et al. (1990), of the various surgical procedures including radial shortening, capitate shortening with capitohamate fusion results in the largest reduction of compressive forces on the lunate. However, this operation alters the congruency of the scaphocapitate joint and the scaphoid no longer rotates smoothly in the midcarpal joint (Moritomo et al., 2004). By contrast, PCS preserves both the scaphocapitate and scaphotrapeziotrapezoid joints, resulting in normal equilibrium and therefore better midcarpal motion (Moritomo et al., 2004). This point seems to be the advantage of PCS over all the other partial carpal fusions. However, with PCS an articular step-off is produced in the midcarpal joint. Although no problem has been reported either in experimental studies (Horii et al., 1992) or case reports of this procedure (Moritomo et al., 2004; Wollstein et al., 2013), long-term follow-up should focus on the possibility of degenerative arthritis.
Although our series was small, there have been only two previous case reports of PCS, with good results (Moritomo et al., 2004; Wollstein et al., 2013) and no previous case series.
Our results are comparable with all other series reporting other types of operative treatment (Afshar, 2010; Altay et al., 2008; Gay et al., 2009). All the patients returned to regular employment at a median of 6 months, with satisfactory range of motion, grip and pinch strengths. All were satisfied with the operation.
Despite good clinical results, in our opinion it is mandatory to confirm revascularization in cases of osteonecrosis, in order to demonstrate that the treatment is effective. Revascularization occurred in all cases in this series (Figure 4).
The major limitations of our study are the limited number of patients, the relatively short follow-up and the fact that our study was a case series. Larger prospective series with control groups and with longer follow-up are mandatory for reliable conclusions, but such studies are difficult to set up for Kienböck’s disease. Additionally, experimental and clinical studies should also take account the variations of the lunate and the step-off in the midcarpal joint. Nevertheless, our early results indicate that PCS seems to be an effective treatment for Lichtman stage II and III-A patients.
Footnotes
Acknowledgements
Thanks to Cihan Aslan for technical and scientific considerations.
Conflict of interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.