
Abstract
The aim of this study was to evaluate the accuracy of magnetic resonance imaging in the detection of triangular fibrocartilage complex injury through a meta-analysis. A comprehensive literature search was conducted before 1 April 2014. All studies comparing magnetic resonance imaging results with arthroscopy or open surgery findings were reviewed, and 25 studies that satisfied the eligibility criteria were included. Data were pooled to yield pooled sensitivity and specificity, which were respectively 0.83 and 0.82. In detection of central and peripheral tears, magnetic resonance imaging had respectively a pooled sensitivity of 0.90 and 0.88 and a pooled specificity of 0.97 and 0.97. Six high-quality studies using Ringler’s recommended magnetic resonance imaging parameters were selected for analysis to determine whether optimal imaging protocols yielded better results. The pooled sensitivity and specificity of these six studies were 0.92 and 0.82, respectively. The overall accuracy of magnetic resonance imaging was acceptable. For peripheral tears, the pooled data showed a relatively high accuracy. Magnetic resonance imaging with appropriate parameters are an ideal method for diagnosing different types of triangular fibrocartilage complex tears.
Level of Evidence: Diagnostic Level III
Introduction
Traumatic and degenerative injuries of triangular fibrocartilage complex (TFCC) are a common source of ulnar-sided wrist pain (Hermansdorfer and Kleinman, 1991). However, the diagnosis of TFCC lesions has been difficult and controversial. Physical examination may not be accurate because of a variety of lesions on the ulnar side of the wrist (Ruston et al., 2013). Therefore, effective imaging tests are useful.
Magnetic resonance imaging (MRI) has been shown to be efficacious, with its ability for high contrast resolution in soft tissues (Yoshioka and Burns, 2012). As a non-invasive, more timesaving and cost-effective method than magnetic resonance arthrography (MRA), MRI is favoured by many radiologists and hand surgeons. However, there is no consensus on the accuracy of MRI for TFCC tears. Previous studies comparing MRI and arthroscopic findings have shown varying results. For instance, Morley et al. (2001) compared MRI and arthroscopy in 54 wrists and found an overall sensitivity of 44%, specificity of 87% and accuracy of 56%, whereas in a study reported by Potter et al. (1997), MRI had a sensitivity of 100%, specificity of 90% and accuracy of 97%. There may be several reasons for these differences. The interpretation of peripheral attachment tears with MRI, for example, is much more difficult than central tears (Haims et al., 2002), but some studies did not report the accuracy of MRI in the detection of the different components of the TFCC. Furthermore, various MRI protocols used in previous studies may have a strong influence on the performance of MRI (Ringler, 2013). Hobby et al. (2001) and Smith et al. (2012a) calculated the overall accuracy of MRI for TFCC tears by meta-analysis, but neither of them took the imaging protocols and the correlation of the injured location with the MRI findings into account. In addition, they failed to include all eligible studies, which may lead to publication and selection bias.
Our meta-analysis not only combined data from all included studies, but also calculated the pooled sensitivity and specificity of MRI for both ‘central tears’ and ‘peripheral tears’ of the TFCC. Moreover, we selected high-quality studies using recommended MRI parameters to determine whether an optimal imaging protocol would lead to a better diagnostic performance.
Materials and methods
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009). A total of 26 items of the PRISMA checklist and one flow diagram was included in this article. However, we did not prospectively register our meta-analysis online as the PRISMA indicates. The data were extracted and calculated to yield the overall accuracy of MRI in the detection of TFCC injuries. To reduce the bias resulted from the heterogeneity of included studies, we created three subgroups to illustrate the accuracy of MRI in the detection of central and peripheral tears and to determine whether optimal MRI protocols yielded better results.
Literature search strategy
We conducted a comprehensive literature search of MEDLINE, Embase, the Cochrane Library, OVID, CNKI, open SIGLE, WHO ICTRP, NTIS of published and grey articles up to 1 April 2014, using the search terms ‘TFCC/TFC/triangular fibrocartilage’, ‘MRI/MR/magnetic resonance imaging’, ‘wrist’ and ‘ulnocarpal complex’. We scrutinized the references of all relevant articles for possible inclusion. Two authors conducted the literature search independently, and disagreements were resolved through discussion between the authors.
Inclusion criteria
Studies included in our meta-analysis had to meet the following criteria: (1) the results of MRI of TFCC tears were compared with either arthroscopic or open surgical findings; (2) data were published in the four-fold (2×2) tables (true positives (TP), true negatives (TN), false positives (FP) and false negatives (FN)), or the four-fold tables could be constructed based on the information from the studies. Studies in any designs or languages were eligible. We excluded studies with incomplete data (the four-fold tables could not be constructed) or which used healthy volunteers, cadavers, animals or children as research subjects.
To clarify the accuracy of MRI for tears to different components of the TFCC, we divided the data into ‘central tears’ (subgroup 1) and ‘peripheral tears’ (subgroup 2). ‘Peripheral tears’ included ulnar tears, radial avulsion, distal avulsion and tears of the volar or dorsal radioulnar ligaments (Palmer, 1989). In addition, benefiting from advances in MRI equipment and techniques, MRI has achieved a better performance in the visualization of the tiny structures of the wrist. It has been generally accepted that appropriate parameter settings of MRI are important for high accuracy (Lenk et al., 2004; Ringler, 2013; Yoshioka and Burns, 2012). Ringler (2013) proposed an MRI strategy for the wrist ligaments to increase accuracy. Based on Ringler’s strategy, we established the following criteria.
The study provided detailed information of MRI examination and surgery.
The MRI was read by at least two reviewers who were blinded to the arthroscopic findings.
Magnetic strength was ≥ 1.5 T.
Dedicated wrist coils were adopted.
Field of view (FOV) ≤ 10 cm.
Slice thickness ≤ 2 mm.
Matrix ≥ 384 × 256.
MRI sequences included T1, fat-saturated PD or T2-weight fast-spin-echo (FSE).
The included studies satisfying any five or more of above criteria were selected into subgroup 3 to combine the data of high-quality studies using recommended MRI parameters.
Data extraction
The titles and abstracts of relevant studies were reviewed by two authors independently. The same two authors then reviewed the full texts of all potentially eligible studies for final inclusion in the study. Data from the included studies were subsequently extracted using a standardized form. The following characteristics and data were collected: first author, country, year of publication, language, average age of the subjects, MRI parameters, sample size, TP, TN, FP and FN.
Quality assessment
The quality of the included studies was assessed by two authors independently according to the Quality Assessment Tool of Diagnostic Accuracy Studies (QUADAS) (Whiting et al., 2006). Any disagreements were resolved through discussion.
Statistical analysis
We calculated the sensitivity and specificity along with their 95% confidence intervals (CI) based on the 2-by-2 tables derived from each study. A bivariate mixed model was adopted to construct a summary receiver operating characteristic curve (SROC) and to obtain the corresponding area under the curve (AUC). Heterogeneity was assessed using the Cochran Q statistic and I2 test. A p value <0.05 or a I2 ≥50% indicated significant heterogeneity, and the random effects model was then conducted for the meta-analysis. Funnel plots and Egger’s linear regression test were used to assess publication bias. A symmetric distribution on the funnel plots or a P value >0.05 indicated no significant publication bias.
Results
Characteristics of included studies
The search results are presented in the PRISMA flow diagram (Figure-1). Two studies (Anderson et al., 2008; Haims et al., 2002) were excluded because they provided insufficient data. Finally, 25 studies with 1298 wrists were included in our meta-analysis, of which 23 articles were in English, one in German and one in Chinese (The characteristics of included studies are presented in the Appendix). A total of 22 included studies used arthroscopy and one took open surgery as reference standard, and two had both arthroscopic and open procedures. The diagnostic criterion used by authors to confirm MRI diagnosis of full-thickness tears of TFCC are consistent, described as ‘absence of the TFC or focal full-thickness defect’ or ‘discontinuity or fragmentation of the low-signal-intensity band of the TFCC’. We did not exclude studies on the basis of quality assessment.
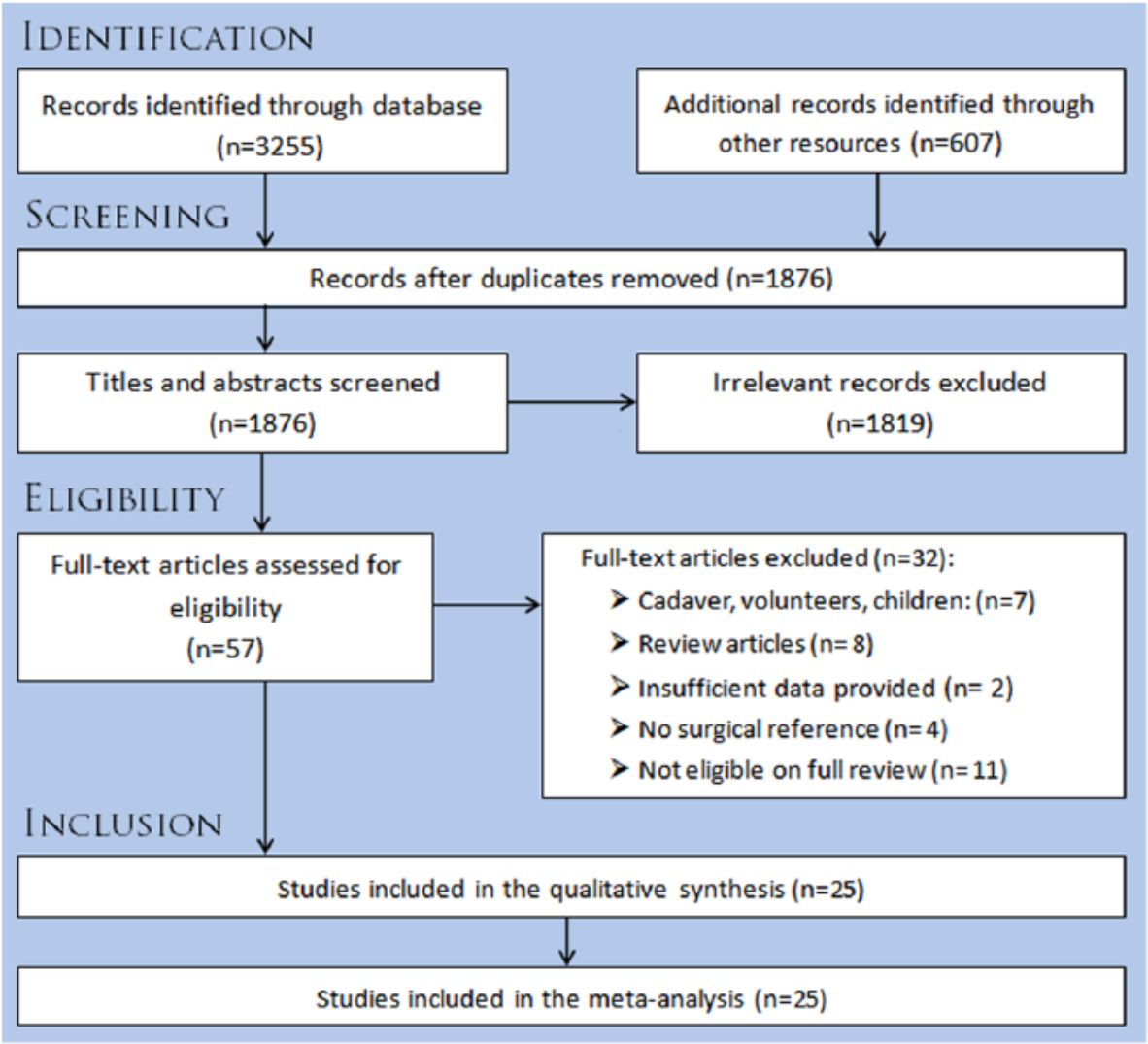
PRISMA flow diagram. Database: MEDLINE, Embase, the Cochrane Library, OVID, CNKI; other resources: open SIGLE, WHO ICTRP, NTIS.
We divided the included studies into several groups. One article (Lee et al., 2013) only provided data on each component of the TFCC, and we failed to obtain an overall accuracy on the basis of the details in the study. Therefore, this study was included in subgroup 1 and subgroup 2, but excluded from the meta-analysis on the overall accuracy of MRI. Eight studies reported the MRI results of different parts of the TFCC: two of these provided data only on central tears (one study) and peripheral tears (one study). Finally, 24 studies were included in the meta-analysis on the overall accuracy, seven were included in subgroup 1 (central tears) (Table 1) and seven were included in subgroup 2 (peripheral tears) (Table 2). A total of six studies met the inclusion criteria of subgroup 3 (high-quality diagnostic studies using recommended MRI parameters) (Table 3).
The data extraction of the studies in subgroup 1 for central tears.
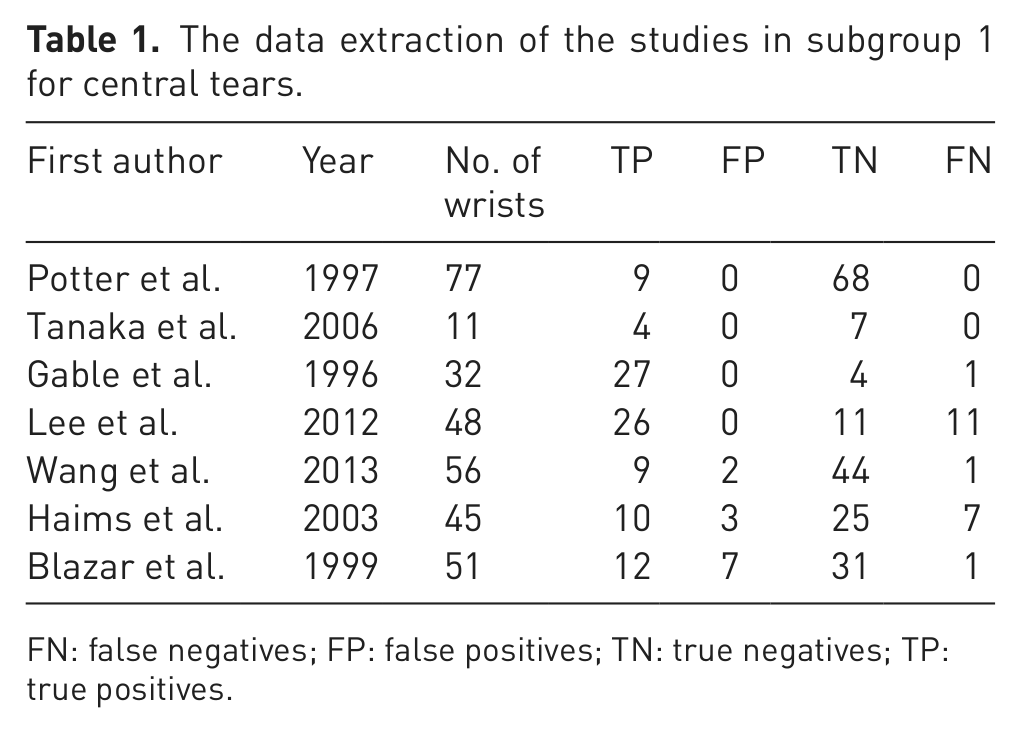
FN: false negatives; FP: false positives; TN: true negatives; TP: true positives.
The data extraction of the studies in subgroup 2 for peripheral tears.
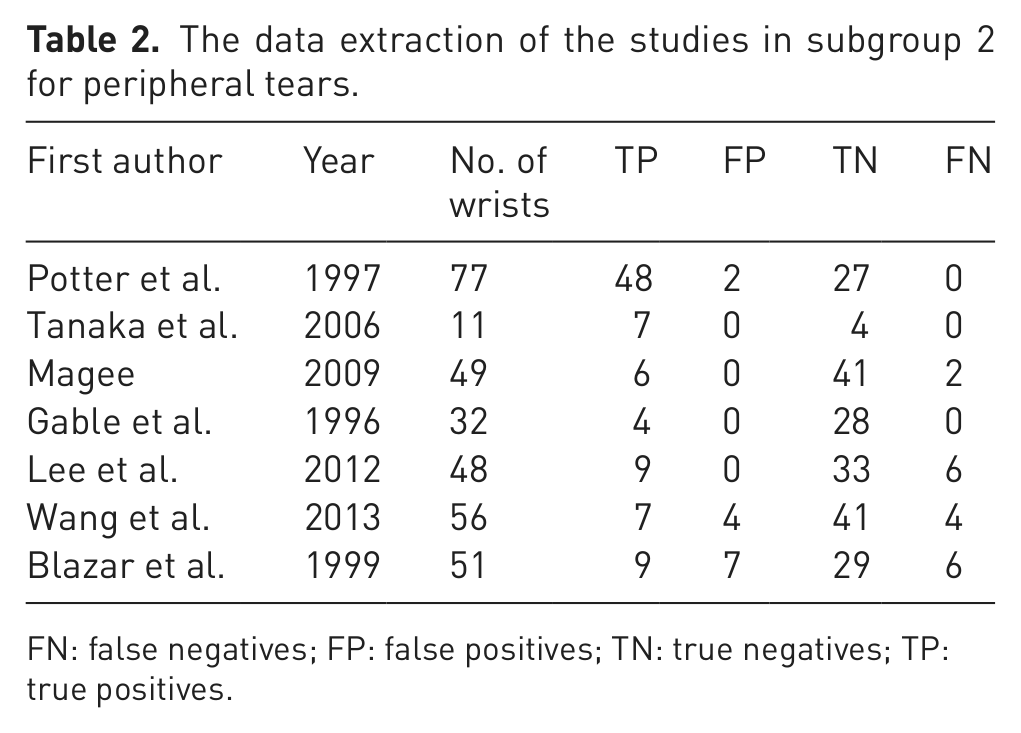
FN: false negatives; FP: false positives; TN: true negatives; TP: true positives.
The MRI parameters used by the high quality studies in subgroup 3.
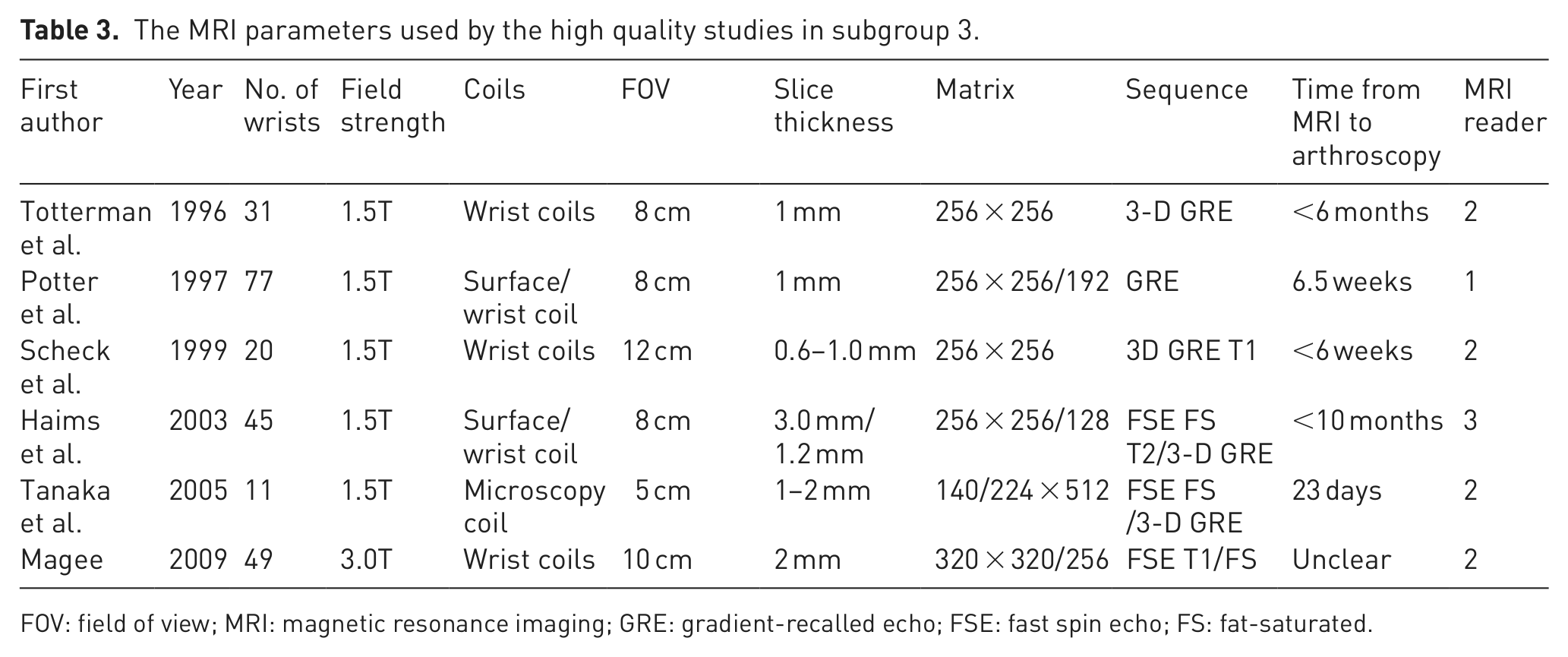
FOV: field of view; MRI: magnetic resonance imaging; GRE: gradient-recalled echo; FSE: fast spin echo; FS: fat-saturated.
Quality assessment
The results of the quality assessment showed that the spectrum of patients in all the included studies was representative of clinical practice. Some studies were poor at blinding procedures, describing the selection criteria and documenting the duration between the index test and the reference test. We regarded both open surgery and arthroscopy as equally efficient reference tests.
Meta-analysis
A forest plot of the meta-analysis on the overall accuracy of MRI for the diagnosis of TFCC injury is shown in Figure 2. The random effects model was adopted because of its significant heterogeneity (I2 >50%). The pooled sensitivity was 0.83 (95% CI: 0.75–0.89); the pooled specificity was 0.82 (95% CI: 0.71–0.89). Figure 3 displays the SROC with the AUC (AUC = 0.89 (95% CI: 0.86–0.92)) denoted. The funnel plots and Egger’s linear regression test (Figure 4) indicated no significant publication bias.
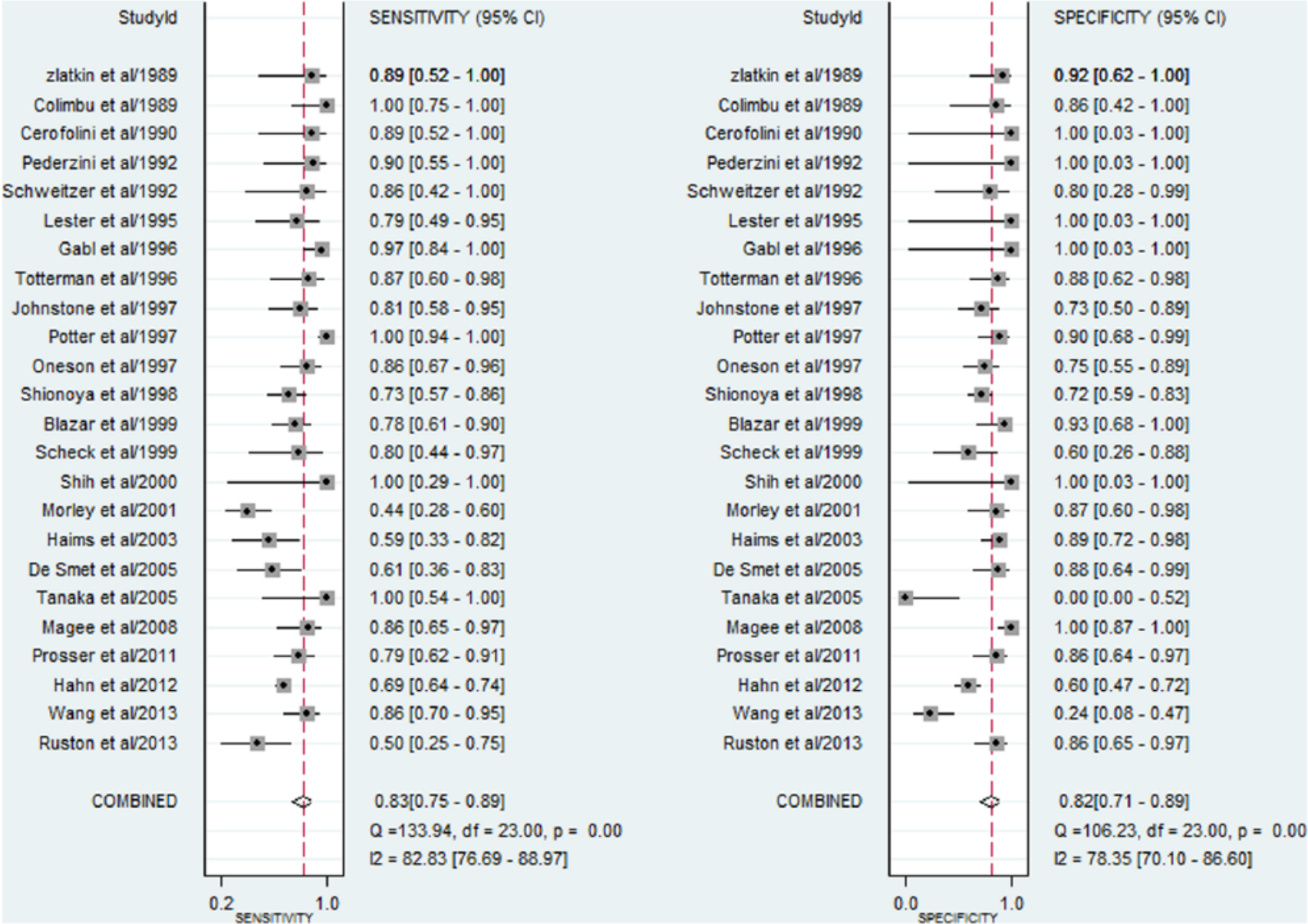
Forest plots for the sensitivity and specificity of MRI in the detection of TFCC tears.
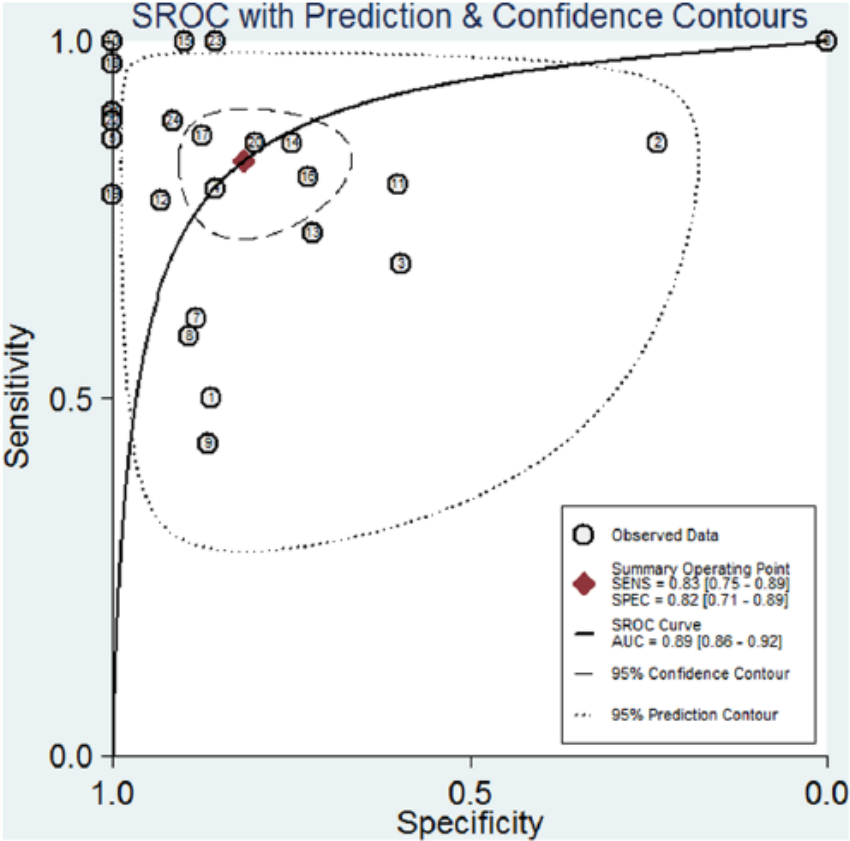
SROC for the overall diagnostic accuracy of MRI.
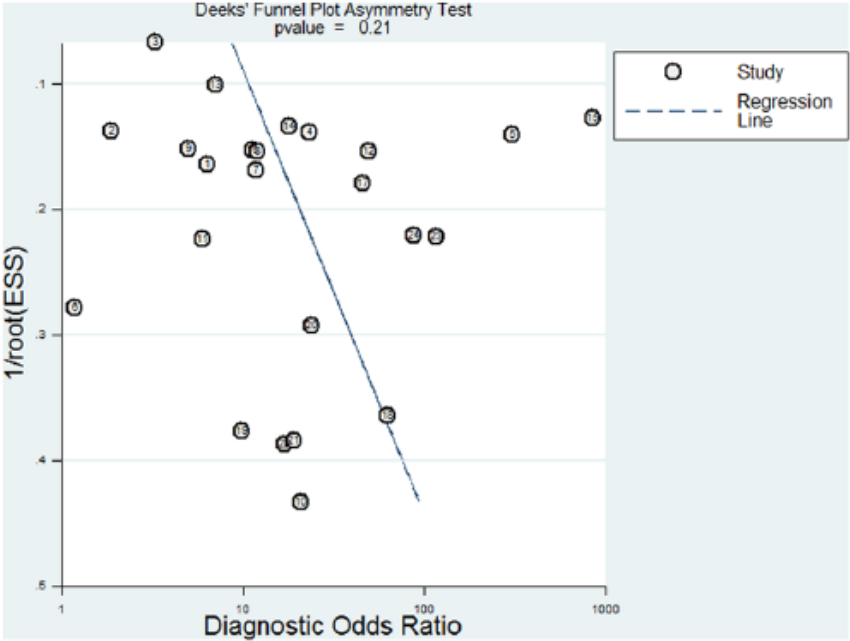
Deek’s funnel plot of publication bias on the pooled diagnostic odds ratio of MRI for the diagnosis of TFCC tears. No publication bias was detected in this meta-analysis.
Covariates
For central tears, the pooled sensitivity was 0.90 (95% CI: 0.70–0.97); the pooled specificity was 0.97 (95% CI: 0.85–0.99); and the area under the SROC (AUC) was 0.98 (95% CI: 0.97–0.99). For peripheral tears, the pooled sensitivity was 0.88 (95% CI: 0.59–0.98); the pooled specificity was 0.97 (95% CI: 0.86–1.00); and the area under the SROC (AUC) was 0.98 (95% CI: 0.97–0.99).
The diagnostic accuracy of subgroup 3 was superior to the overall results of the 24 studies. The pooled sensitivity was 0.92 (95% CI: 0.70–0.98); the pooled specificity was 0.82 (95% CI: 0.40–0.97); and the area under the SROC (AUC) was 0.95 (95% CI: 0.92–0.96).
Discussion
The meta-analysis on the overall diagnostic accuracy of MRI demonstrates an acceptable outcome in the detection of TFCC injury, whereas the meta-analysis of 17 studies conducted by Smith et al. (2012a) demonstrated a pooled sensitivity of 0.75 (95% CI: 0.70–0.79), and a specificity of 0.81 (95% CI: 0.76–0.86). The variances between these two meta-analyses derived from seven studies, which Smith et al. did not include, five of which were published after their literature search on1 August 2010.
In addition, considering the anatomic complexity of the TFCC, the combination of all data from the included studies could not give an accurate picture. The small sizes and oblique orientations of the radioulnar ligaments, ulnar attachments, ulnar lunate and ulnar triquetral ligaments make visualization of the peripheral structures much more difficult than that of central disks. Therefore, to evaluate the accuracy of MRI comprehensively, it is necessary to correlate the MRI findings with the TFCC injury sites, which was not done by most researchers. We selected eight studies that reported the MRI results of different parts of the TFCC to evaluate the ability of MRI to differentiate the locations of tears. For central tears, our meta-analysis demonstrates a high pooled sensitivity of 0.90 and specificity of 0.97, which means that MRI is an accurate method of diagnosing central TFCC tears, whereas for peripheral tears the accuracy of MRI has always been questioned. Haims et al. (2002) reported only 17% sensitivity and 79% specificity of MRI in the detection of peripheral tears. This result has been cited by many authors as a limitation of MRI for peripheral tears (Magee, 2009; Ringler, 2013; Tanaka et al., 2006; Yoshioka and Burns, 2012). However, our meta-analysis on seven studies that reported the accuracy of MRI in detecting peripheral tears demonstrated a relatively high result, with a sensitivity of 0.88 and specificity of 0.97. Although the term ‘peripheral tears’ covers injury to all the structures of the TFCC except the central disks, and the positive standard of the index test was slightly different between studies, this unexpected high accuracy may change our traditional view. In addition, more high-quality studies with greater numbers of cases are required to illustrate the performance of MRI in detecting peripheral TFCC tears.
The quality assessment with QUADAS indicated that the MRI strategies used by the included studies were different. Considering the demanding equipment and the complicated parameter configuration of MRI, it is difficult for researchers to adopt a unified strategy. However, the diversity of MRI strategies increased the clinical heterogeneity between the included studies, which might lead to bias in the meta-analysis. Therefore, we created subgroup 3 to include the high-quality studies with recommended MRI parameters to determine whether a superior MRI strategy lead to a better accuracy. The inclusion criteria for subgroup 3 were derived from the MRI protocols recommended by Ringler in 2013 and QUADAS. The meta-analysis on six included studies of subgroup 3 demonstrated a sensitivity of 0.92, a specificity of 0.82 and an AUC of 0.95. Compared with the overall diagnostic accuracy of the 24 included studies, the better results of subgroup 3 indicated that proper parameters can considerably increase the diagnostic accuracy of MRI in detecting TFCC injury.
Although we have taken each component of TFCC and the MRI parameters into consideration, unavoidable bias resulted from other factors that cannot be ignored. For example, we excluded two studies for failing to provide sufficient data. In addition, we could not estimate the disease progression bias because 18 included studies did not document the duration between imaging and surgical confirmation. Blazar et al. (2001) showed that there are variations between MRI results reported by different reviewers, and indicated that an experienced radiologist would take a key role in the interpretation of MRI scans. However, the magnetic resonance images were interpreted by only one reviewer in some included studies, and some authors did not provide detailed information of the reviewers. Furthermore, 12 included studies did not blind the reviewers of the MRI scans to the arthroscopic findings, and only one conducted double-blind procedures. Previous studies did not find a difference between open and arthroscopic surgery for the detection of TFCC tears. Therefore, we used both open surgery and arthroscopy as reference standards in this meta-analysis. Although some studies mentioned partial tears, we extracted only the data on full-thickness tears for the lack of consensus about the imaging diagnosis of partial TFCC tears.
It is widely accepted that central degenerative changes to the TFCC have a greater prevalence in the elderly, and surgical repair for this condition is difficult, whereas peripheral tears are often symptomatic and treatable (Grechenig et al., 1998; Taleisnik, 1987). Therefore, an accurate preoperative diagnosis of tears localized to the peripheral structures of the TFCC is important for the treatment strategy. Our meta-analysis on subgroup 1 and subgroup 2 may help in this respect.
Previous studies have shown that the ability of conventional arthrography to detect intrinsic ligament tears in the wrist is limited compared with MRI (Smith et al., 2012b). Furthermore, MRI often helps to exclude potential diagnoses, thus narrowing the differential diagnosis and increasing certainty. Several studies demonstrated that depiction of intraarticular structures by magnetic resonance can be enhanced by the introduction of contrast material into the joint. Many authors have compared the accuracy of MRI with MRA, but there is no consensus (Braun et al., 2003; Haims et al., 2003; Magee, 2009). Although Smith’s meta-analysis demonstrated that MRA was superior to MRI, Smith et al. still considered that the improvement in the performance of MRA might not have been sufficient for some clinicians to use MRA instead of MRI (Smith et al., 2012a). Besides, MRI is non-invasive, more cost effective and less time-consuming than MRA.
In conclusion, the overall accuracy of MRI for diagnosis of TFCC injury is good. For central tears, MRI is an accurate method in detection of full-thickness injuries. For peripheral tears, the pooled data unexpectedly showed a relatively high accuracy. MRI with appropriate parameters can be an ideal method for diagnosing different types of TFCC tears.
Footnotes
Conflict of interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.