
Abstract

Dear Sir,
Upper limb tourniquets are used widely and are typically very safe (Odinsson and Finsen, 2006; Drolet et al., 2014). For adults, the recommended maximal tourniquet time vary widely, with 1 hour 30 minutes–2 hours being the most widely accepted (Odinsson and Finsen, 2006; Drolet et al., 2014). Yet Flatt (1972) reported that it was safe to use an upper limb tourniquet for up to 2 hours 45 minutes. The guidance to surgeons may satisfy the precautionary principle, but not be evidence based. The aim of this study was to assess local symptoms and any complications of upper limb tourniquet use for over 2 hours in a cohort of elective hand surgical patients.
All patients were included who had a tourniquet applied for more than 2 hours over a 5-year period 1999–2004. The vast majority of the patients operated in this period had tourniquet times of <2 hours. Post-operatively, patients were assessed for pain at the tourniquet site, nerve palsy and compartment syndrome. They were assessed again on the first post-operative day and reviewed in clinic for at least 6 weeks. In addition, all patients were sent a simple follow-up postal questionnaire to validate the data collected; this enquired about both immediate and chronic local tourniquet site pain and distal paraesthesia and other complications of surgery.
An Anetic Aid tourniquet (Anetic Aid Ltd, West Yorkshire, UK) was used in all patients. It was 80 cm long and 8 cm wide. The upper limb was exsanguinated by elevation and manually squeezing the forearm muscles; the tourniquet cuff was inflated to 250 mmHg. The tourniquet times were recorded.
We identified 81 patients with a documented tourniquet time of 2 hours or more over a 5-year period. There were 54 women and 27 men, with a mean age of 53 years (range 18–83). A total of 70 patients (86%) had a primary diagnosis of rheumatoid arthritis. The other patients were treated for problems related to osteoarthritis or post-traumatic elective surgical reconstruction. Table 1 shows the number of patients per 15 min intervals of tourniquet time over 2 hours. The longest recorded duration was 3 hours 10 minutes.
Table showing the numbers of patients with short-term local pain and paraesthesia against tourniquet time.
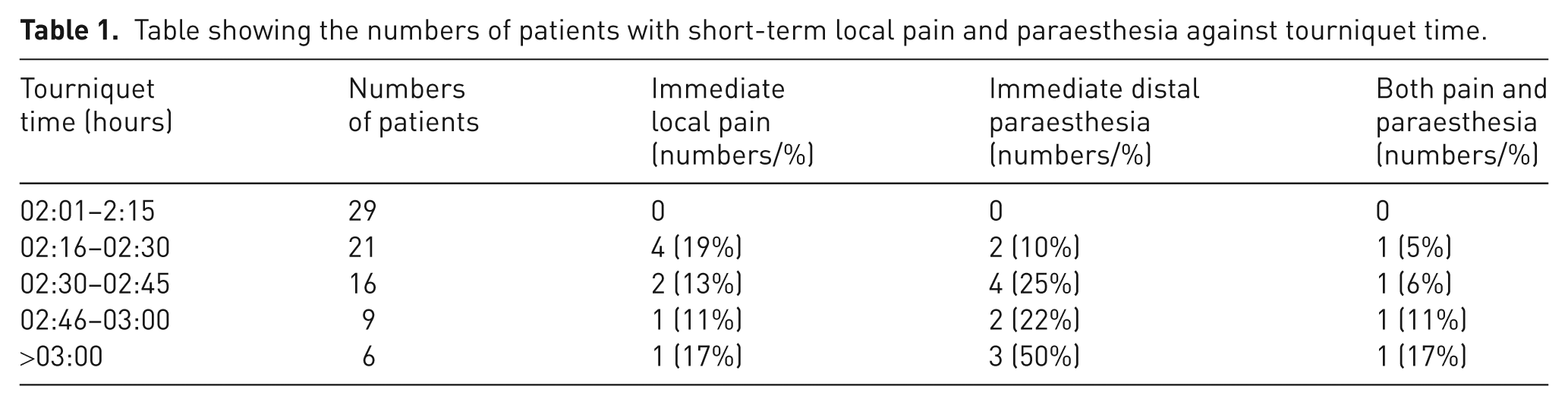
Short term, eight patients had local site pain at the site of the tourniquet: six resolved within 2 days; the other two resolved within 2 weeks. Eleven patients reported distal paraesthesia: eight resolved within 2 days, two resolved within 1 week and one patient experienced persistent paraesthesia. Clinically this was clearly not due to compartment syndrome. Of these patients, nine had received a regional nerve block.
Four patients reported both local site pain and distal paraesthesia. All symptoms resolved within 1 week. Their tourniquet times were between 2 hours 30 minutes and 3 hours 10 minutes. There is a trend to greater short-term adverse effects following longer operations. This may be due to prolonged tourniquet use or it may be due to greater post-operative swelling having had more extensive surgery (we did not measure post-operative swelling) or other factors.
Two patients developed chronic regional pain syndrome type 1 (CRPS 1). In one patient this was noticed 4 weeks following complex rheumatoid surgery. The tourniquet time was 2 hours 4 minutes and there was no immediate post-operative pain or distal paraesthesia. In the other patient, it was noticed after 8 weeks, again following multiple procedures for the rheumatoid hand. The tourniquet time was 3 hours 5 minutes; this patient reported initial distal paraesthesia that resolved within 24 hours.
Follow-up questionnaires were sent to 71 patients for whom addresses were known. One patient had died. A total of 61 patients responded (86%). The minimum post-operative time to questionnaire was 10 months. Four patients reported distal pain symptoms unconnected to the site of the tourniquet. Three patients reported distal paraesthesia: two of these had paraesthesia immediately post-operatively that had resolved completely; the third had persistent paraesthesia that seemed primarily related to their underlying rheumatoid arthritis (RA) rather than the tourniquet, but may have been due to the long tourniquet time (>2 hours 45 minutes). No patient reported any other complications not previously noted; none reported symptoms suggestive of compartment syndrome.
Tourniquet use is typically very safe (Odinsson and Finsen, 2006). Most tourniquet complications are associated with either the duration of ischaemia or the pressure generated beneath the cuff. Sometimes prolonged tourniquet use is needed to address a complication during surgery or to undertake multiple procedures. The absolute safe limit of tourniquet duration has not been established.
Overall our findings reflect those of Flatt (1972), who showed that 60 patients with a tourniquet duration of between 2 hours 45 minutes had no post-operative complications. This is important as many authorities quote time limits for upper limb tourniquet use of 1 hour 30 minutes or more reasonably 2 hours. This study and Flatt’s work appear to show that tourniquet use can be safely extended to well beyond 2 hours. The majority of our patients had tourniquet times between 2 hours 45 minutes, and even in these patients there was a trend to more short-term symptoms. These may simply reflect responses to more surgery but may also be due to swelling and soft tissue injury from longer tourniquet times. There were only 11 patients with tourniquet times >2 hours 45 minutes and these patients had an even stronger trend towards more short-term symptoms, and the only patient with possible long term symptoms from tourniquet use was in this group. The data more strongly support the use of an arm tourniquet up to, than beyond 2 hours 45 minutes. The ability to use a tourniquet for >2 hours gives greater flexibility to surgeons planning complex operations or addressing complications during operations by allowing longer tourniquet use. It should also help resist spurious medico-legal claims based solely on prolonged tourniquet times. Nonetheless we would strongly advocate minimizing tourniquet use as we do not know whether there may be subtle physiological changes that should be minimized for patient benefit.
Footnotes
Conflict of interest
None declared.