
Abstract

Dear Sir,
Intra-articular injections are routinely performed for therapeutic effect in painful joints of the hand and wrist in a wide range of clinical settings, commonly without image guidance. The difficulty in accurate intra-articular needle placement when using clinical assessment alone, even for the larger joints of the body, has long been appreciated (Smith et al., 2011). In a meta-analysis of comparative studies, ultrasound-guided injections to the wrist resulted in greater reductions in pain and a greater likelihood of achieving a clinically significant improvement in symptoms, compared with clinical assessment alone, at 1 to 6 weeks follow-up (Dubreuil et al., 2013). The complication rate (skin hypopigmentation, fat atrophy and crystal deposition) doubles with peri-articular injection (Lopes et al., 2008). Accurate placement of the needle in the joint contributes in achieving the desired therapeutic benefit and reduces the incidence of complications.
Fluoroscopic guidance is frequently used by hand surgeons performing joint injections. The aim of the study was to determine the accuracy of clinical assessment alone in achieving intra-articular positioning for a wide range of hand and wrist joint injections and compare this with the accuracy achieved using fluoroscopic guidance.
Data was collected prospectively over 12 months. All injections were undertaken in the operating theatre under aseptic technique in conscious patients and were performed by two Consultant Hand Surgeons, three senior Registrars and one Core Surgical Trainee. The injection technique was standardized. The needle was placed into the position clinically assessed to be intra-articular using anatomical landmarks. The needle was advanced until there was a perceived puncture of the joint space. The accuracy of needle placement was then assessed with fluoroscopy using orthogonal views. If an intra-articular position had not been achieved using clinical assessment alone then fluoroscopy was used to achieve this. The joint was then injected with a prepared mixture of local anaesthetic and corticosteroid. Our standardized technique for each joint is described in detail in Appendix 1 (available online). The data were collected and entered onto Excel (Microsoft, Seattle, WA, USA) and analysed. Fischer’s exact test was used in the statistical analysis.
A total of 50 joint injections were performed in 37 patients (26 women and 11 men) with a mean age of 59 years. The aetiology was primary osteoarthritis (40 injections), post-traumatic osteoarthritis (four) and post-traumatic pain (six). The mean patient follow-up time was 6.5 months (range 2 to 11). Four joints had further injections (two thumb carpometacarpal (CMC) joints, two interphalangeal joints); seven joints underwent operative management (four trapeziectomies, one fusion of the little finger CMC joint and two distal interphalangeal joint fusions). One case of hypopigmentation of the skin occurred as a delayed complication on routine review of all patients in the outpatient clinic at 6 weeks post-injection.
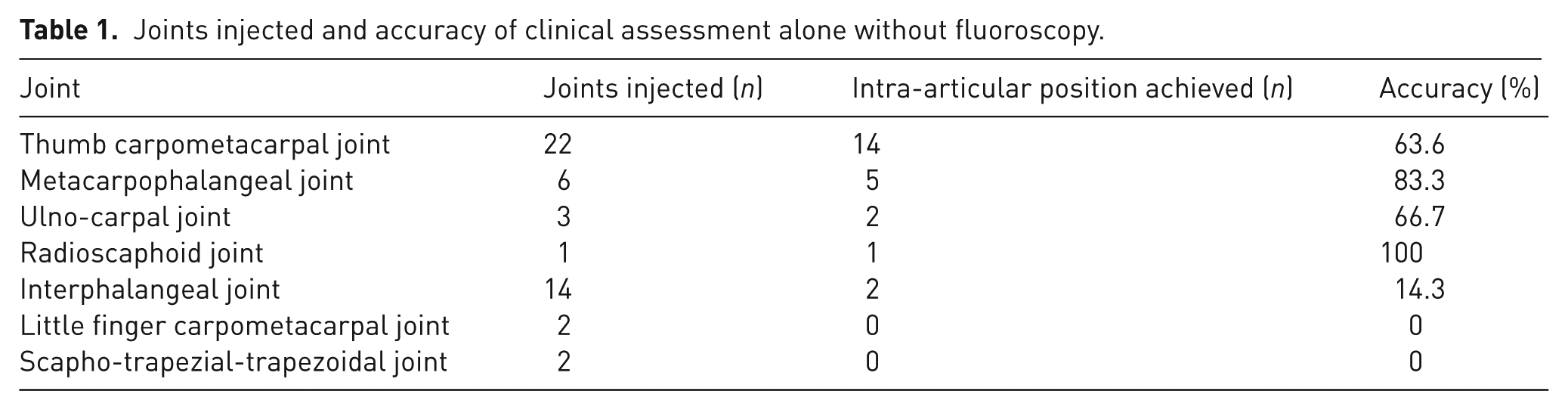
The distribution and accuracy of the intra-articular injections is shown in Table 1. The overall accuracy using clinical assessment alone was 48%. When intra-articular positioning using clinical assessment failed, subsequent positioning using fluoroscopy was always successful. Accurate localization using clinical assessment alone was significantly lower than that achieved when using fluoroscopy (p < 0.0001). The use of clinical assessment alone for the small joints of the hand (interphalangeal joint, scapho-trapezial-trapezoidal joint and little finger CMC joint) was significantly less accurate (p < 0.0001) when compared with the larger joints (thumb CMC joint, metacarpophalangeal, radiocarpal and ulnocarpal joints). The accuracy varied with the grade of surgeon, with 4/10 (40%) for Core Trainees, 16/35 (45.7%) for Specialist Registrars and 4/5 (80%) for Consultants. These differences were not statistically significant when comparing between grades (e.g. Non-Consultant versus Consultant p = 0.18); this may simply be because it was a small study.
Joints injected and accuracy of clinical assessment alone without fluoroscopy.
The overall accuracy of injections using clinical assessment alone for a wide range of joints in the hand and wrist was limited. This brings into question whether these injections should be performed on a routine basis without the aid of fluoroscopy, or some other form of image guidance. We chose to study a wide range of hand and wrist joints in order to represent the variety treated in a hand surgeon’s daily practice, and chose fluoroscopy as the imaging technique as this is readily available in hand surgery practice.
In this study, the accuracy achieved for injections of the thumb CMC joint was comparable with previously published studies (Helm et al., 2003), indicating our technique was comparable. Our population of predominantly osteoarthritic joints may reflect more accurately the patients seen in hand surgery outpatient clinics, as compared with the rheumatoid populations in other studies (Lopes et al., 2008). A limitation was the number of different surgeons and grades injecting, though this pragmatic study design may reflect the variety of surgeon seniority regularly undertaking these injections. The moderate number of injections included is comparable with other studies investigating other anatomical sites, however, the results should be viewed with caution, particularly those relating to the small joints with lower numbers injected. Furthermore, this study is not able to comment on the risk of complications from peri-articular injections, nor their relation to therapeutic effect.
This report serves as a reminder for surgeons and other practitioners in the outpatient setting to consider using image guidance when performing intra-articular injections into the hand and wrist, especially the smaller joints.
Footnotes
Acknowledgements
Many thanks to S Sharma and T Sinnett for their recruitment of patients to the study.
Conflict of interests
None declared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.