
Abstract
We investigated whether there is an optimal grip span for determining the maximum handgrip strength in preschool children and if it is influenced by gender, age, or hand size. A total of 292 preschool children (3–5 years; 59.2% boys) carried out the handgrip strength test with different grip spans (4.0, 4.5, 5.0, 5.5, and 6.0 cm). The hand size was also measured. We also determined the reliability of the optimal grip span in another group of children (n = 56, 57% boys) who did the test twice, with a 3-hour difference between tests. The results showed that 4.0 cm is the optimal grip span to determine the maximum handgrip strength in preschool children. This result applied to both genders, all age groups, and hand sizes. Paired t-tests showed no significant differences between test and retest. These findings may guide clinicians and researchers in selecting the optimal grip span when measuring handgrip strength in preschool children.
Level IV
Introduction
There is increasing evidence that muscular strength is a marker of health in childhood and adolescence (Ortega et al., 2008; Ruiz et al., 2009; Smith et al., 2014). A prospective study with one million participants showed that muscular strength in adolescence is associated with lower risk of all-cause premature mortality, as well as with premature mortality due to cardiovascular disease and suicide (Ortega et al., 2012). In the last decade, assessment of muscular strength has become popular, and it has been included in several fitness-test batteries in children and adolescents (Artero et al., 2011a; Castro-Pinero et al., 2010; Ortega et al., 2012; Vicente-Rodriguez et al., 2008). Less is known however about whether muscular strength is a marker of health in younger populations and whether its assessment is feasible in children as young as 3-5 years old (hereafter called preschool children) (Ortega et al., 2015).
The handgrip strength test is a relatively simple test that has been widely used in experimental and epidemiological studies in youth (Ardoy et al., 2011; Artero et al., 2011b; Castro-Pinero et al., 2010; Moliner-Urdiales et al., 2010; Ortega et al., 2012; Ruiz et al., 2006a; Ruiz et al., 2011). It is considered as a good indicator of overall strength in young people (Artero et al., 2012) and it seems to be valid and reliable (Artero et al., 2011a; Castro-Pinero et al., 2010; Ruiz et al., 2009). However this test can be affected by factors, such as joint angles (Ahrens et al., 2006; Artero et al., 2012; Hilgenkamp et al., 2010; Ruiz et al., 2006b), posture (Ahrens et al., 2006; Espana-Romero et al., 2010; Ruiz et al., 2006b), grip span (Ahrens et al., 2006; Espana-Romero et al., 2008; Firrell and Crain, 1996; Mathiowetz et al., 1985; Richards et al., 1996; Ruiz et al., 2006b; Ruiz-Ruiz et al., 2002; Su et al., 1994; Watanabe et al., 2005), and individuals’ hand sizes (Espana-Romero et al., 2008; Ruiz et al., 2006b; Ruiz-Ruiz et al., 2002; Trampisch et al., 2012). We showed that there is an optimal grip span to which the dynamometer should be adjusted when measuring handgrip strength in adults (Ruiz-Ruiz et al., 2002), adolescents (Ruiz et al., 2006b), and children aged 6 years and older (Espana-Romero et al., 2008). Moreover, we showed that the optimal grip span was influenced by hand size in both genders of any age, except in adult men (Ruiz-Ruiz et al., 2002). It is expected that preschool children may need a different optimal grip span when measuring handgrip strength compared with older populations (Bear-Lehman et al., 2002).
Studies examining which position on the grip dynamometer will result in maximum handgrip strength in preschool children are needed to inform population-based studies as well as intervention studies on how to appropriately assess this test. Therefore, the aim of this study was to investigate whether there is an optimal grip span for determining the maximum handgrip strength in preschool children and if that grip span is influenced by gender, age, or children’s hand size.
Materials and methods
Participants
A total of 292 preschool children aged 3–5 years (59.2% boys; n = 83, 101 and 108 for 3, 4, and 5 years old, respectively) participated in the study. Children were recruited from three public schools located in Southern Spain. Children were healthy and free of any injury or impairments in the upper limbs. A comprehensive description of the purpose of the study was given to both their parents or legal guardians and teachers. One parent or legal guardian provided written informed consent. The study protocol was performed in accordance with the ethical standards (Declaration of Helsinki, revised in 2013) and was approved by the local Review Committee for Research Involving Human Subjects.
Procedures
Measurement of handgrip strength
Maximal handgrip strength was tested using an analogue dynamometer (TKK model 5001, Grip-A, Takei, Tokyo, Japan; range 0–100 kg, precision 0.5 kg), and following the procedure described in the ALPHA-fitness test battery (www.thealphaproject.net) (Artero et al., 2011a; Castro-Pinero et al., 2010; Ruiz et al., 2009, 2011). We used an analogue dynamometer because, as it has been previously reported (Ploegmakers et al., 2013), and as we observed in an unpublished pilot study, there are preschool children with handgrip strength levels below 5 kg. The digital version of the TKK dynamometer (TKK 5401 Grip-D; Takey, Tokyo, Japan; range 5–100 kg, precision 0.1 kg) is not able to register strength levels below 5 kg.
To do the test, children stood on both feet with the arm of the tested side straight down, the shoulder slightly abducted (~10°, not touching the rest of the body), in full elbow extension (0° of flexion), the forearm in neutral position, and the wrist in 0° flexion. Each child did the test once (alternately with both hands) at different grip spans, starting from the lowest grip span possible. The spans were 4.0, 4.5, 5.0, 5.5, and 6.0 cm. For each measure, the side of the hand to be tested first, as well as the grip span, were chosen randomly. The mean of the handgrip strength obtained with each hand at each grip span was calculated and used in all the analyses. The children were encouraged to do their best when performing the tests.
Measurement of grip span
Grip span was measured from the external base of the grip to the mark placed in the central strip of the dynamometer with an accuracy of 0.1 cm (Espana-Romero et al., 2008).
Measurement of hand size
Hand size was measured in both hands with an accuracy of 0.1 cm, from the tip of the thumb to the tip of the small finger with the hand opened as wide as possible. The average of right- and left-hand size was calculated and used in all the analyses (Figure 1).

Measurement of hand size (0.1 cm precision).
Reliability
To confirm the reliability of the optimal grip span when measuring handgrip strength in preschool children, an additional group of 56 children (n = 32 boys) aged 3–5 years recruited from another public school (in Granada, Southern Spain) carried out the test at the obtained optimal grip span on two occasions with a 3 hour difference between the tests.
Statistical analysis
Age, hand size, and handgrip strength differences between boys and girls were determined with unpaired t-tests in all participants, and by age groups (3, 4, and 5 years). To determine the grip span at which the maximum handgrip strength was obtained, we conducted analysis of variance for repeated measures, where the handgrip strength obtained at each grip span (i.e. 4.0, 4.5, 5.0, 5.5, and 6.0 cm) was entered as a fixed factor. Post-hoc analyses with a Bonferroni adjustment were conducted to compare the handgrip strength obtained at each grip span. We conducted the analysis by gender, age (3, 4, and 5 years), and hand size groups (12, 13, 14, 15, and 16 cm), and also tested the interactions between grip span and gender, age groups, and hand size groups.
We also examined the association between hand size and handgrip strength obtained with the optimal grip span by one-way analysis of covariance, where hand size was entered as a fixed factor, handgrip strength obtained with the optimal grip span was entered as a dependent variable and age was entered as a covariate. The analysis was conducted in boys and girls separately.
For the reliability analysis of the optimal grip span, we conducted t-tests using zero as a reference to determine whether the mean difference (test minus retest) was significantly different from zero. The intra-class correlation coefficient was also calculated.
Results
Table 1 shows descriptive values for age, hand size, and handgrip strength levels of study participants by gender and age groups. Boys had a bigger hand size and higher levels of handgrip strength (all p < 0.05). When the analyses were conducted by age groups, we observed that the hand size as well as the handgrip strength levels were similar in boys and girls aged 3 and 4 years, whereas in children aged 5 years, both hand size and handgrip strength levels were higher in boys.
Mean age, hand size, and handgrip strength levels of study participants by gender and age groups.
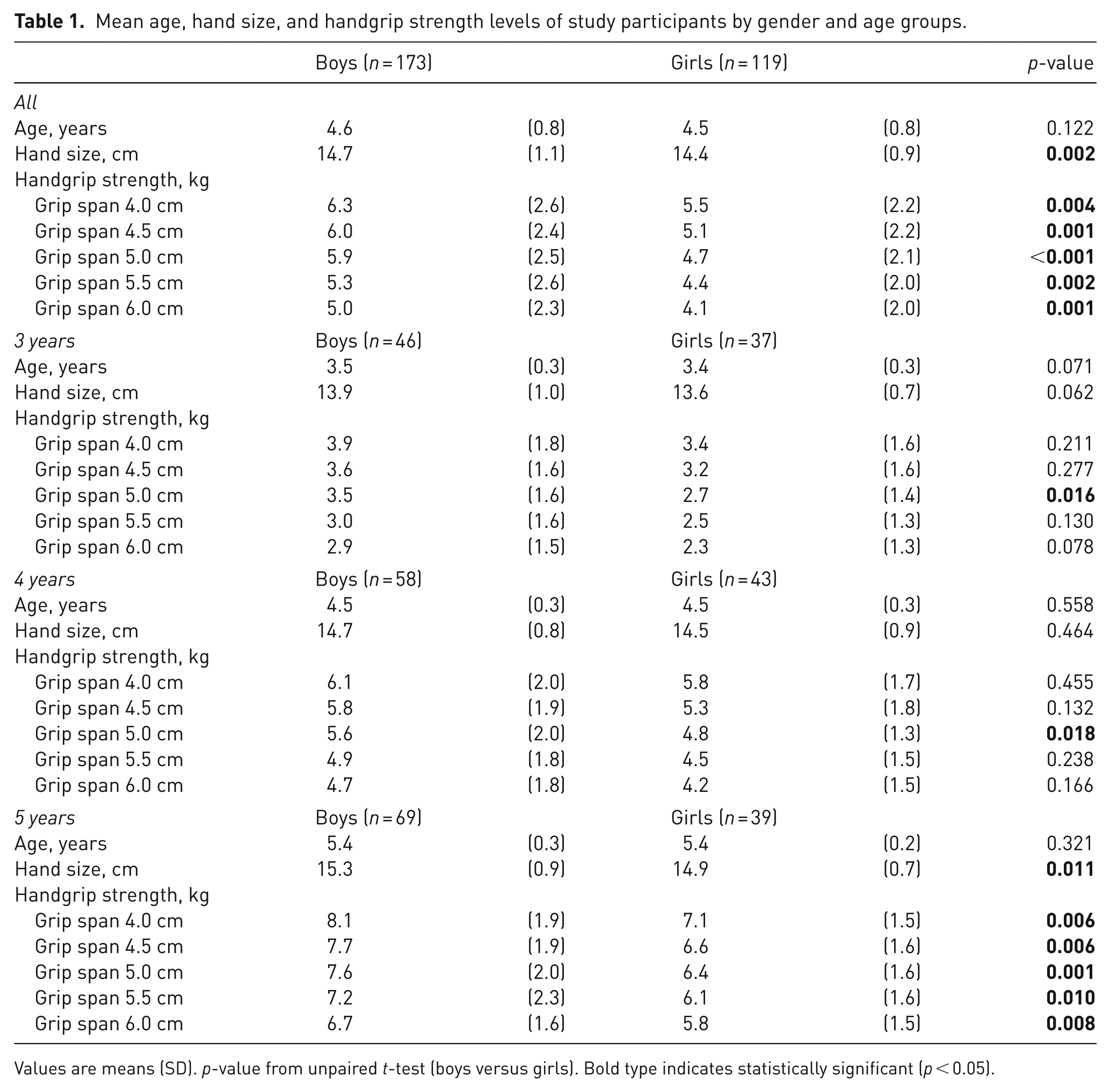
Values are means (SD). p-value from unpaired t-test (boys versus girls). Bold type indicates statistically significant (p < 0.05).
Figure 2 shows the handgrip strength levels obtained at each grip span (4.0, 4.5, 5.0, 5.5, and 6.0 cm) by gender, age, and hand size groups. In all cases, analyses showed that there was a significant association between grip span and handgrip strength; so that the higher the grip span the lower the handgrip strength. This applied to boys and girls, age groups (3, 4, and 5 years) and hand size (Figure 2). Moreover, there was no significant interaction between grip span and gender, age, or hand size groups. The grip span at which participants obtained the maximum handgrip strength (4.0 cm) was consistent in all cases. The handgrip strength levels obtained with the grip span set at 4.0 cm was significantly higher than the handgrip strength levels obtained with the grip span set at 4.5 cm or higher in all cases except in children aged 3 years (3.7 (SD 0.2) and 3.4 kg (SD 0.2) for 4.0 and 4.5 cm, respectively; p = 0.193), and in children with a hand size of 12 cm (2.8 (SD 0.4) and 2.7 kg (SD 0.3), for 4.0 and 4.5 cm, respectively; p = 0.999), 15 cm (7.4 (SD 0.2) and 7.0 kg (SD 0.2), for 4.0 and 4.5 cm, respectively; p = 0.250), and 16 cm (8.2 (SD 0.3) versus 8.0 kg (SD 0.4), for 4.0 and 4.5 cm, respectively; p = 0.999).

Mean handgrip strengths shown by gender, age, and hand size groups. Error bars show 95% confidence intervals. p from repeated measures analysis.
Figure 3 shows the levels of handgrip strength obtained with the grip span set at 4.0 cm across hand size groups in boys and girls. Handgrip strength was greater for larger hand sizes after adjusting for age.
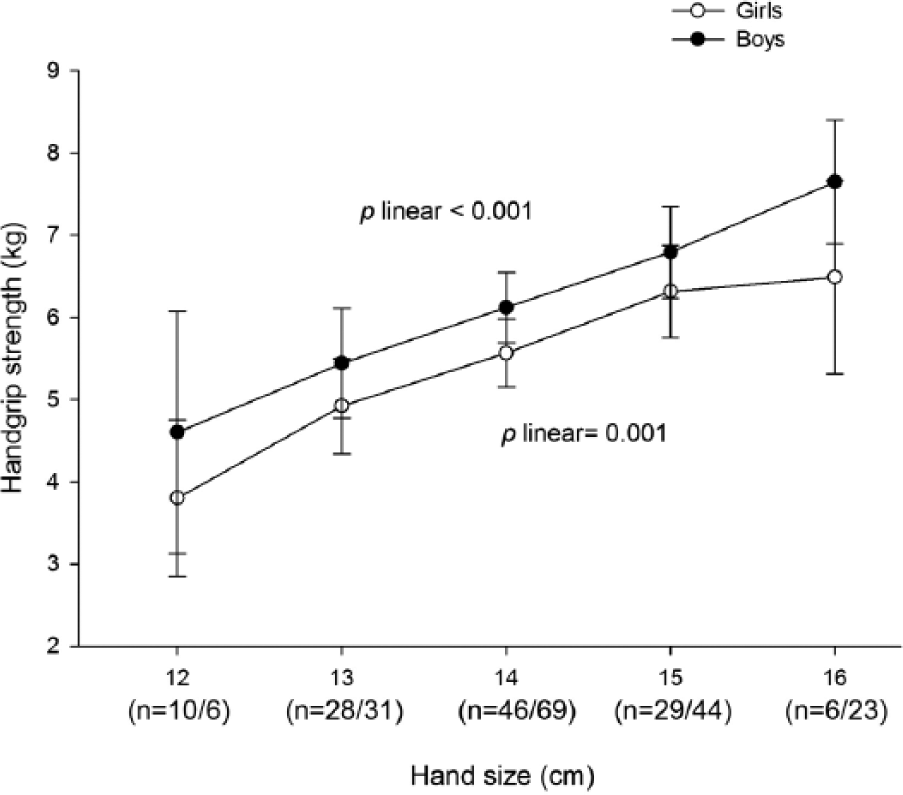
Handgrip strength levels obtained with grip span set at 4.0 cm across hand size groups in boys and girls. Values are age-adjusted means. Error bars show 95% confidence intervals. Within parentheses are the frequencies of girls/boys by hand size group.
Reliability
Paired t-tests showed no significant differences between test and retest in all participants (6.6 (SD 3.0) and 6.4 kg (SD 2.7), respectively; mean difference 0.20 kg; 95% confidence interval −0.10 to 0.51; p = 0.193). In boys the obtained values were 6.6 (SD 3.0) and 6.2 kg (SD 2.6), respectively; mean difference 0.39 kg; 95% confidence interval −0.04 to 0.82 kg; p = 0.074. In girls the obtained values were 6.6 (SD 3.1) and 6.7 kg (SD 3.0), respectively; mean difference −0.04 kg; 95% confidence interval −0.50 to 0.42 kg; p = 0.854. Reliability coefficients (i.e. intra-class correlation coefficient) were 0.919 for all participants, and 0.908 and 0.936 for boys and girls, respectively.
Discussion
The results of this study suggest that there is an optimal grip span of 4.0 cm to which the dynamometer should be adjusted when measuring handgrip strength in preschool children aged 3–5 years. This optimal grip span was the same for, children aged 3, 4, or 5 years, and children with different hand sizes (12, 13, 14, 15, and 16 cm), which simplifies the measurement in this population. Moreover, there was no gender interaction, which indicates that the association between hand size and handgrip strength is unaffected by gender. Boys may have a larger hand size than girls of the same age, but the increase in hand grip strength with increasing hand size is similar for boys and girls. We also observed that the optimal grip span was reliable in preschool children.
The handgrip strength test is currently used worldwide because it is a relatively cheap test that gives practical information on muscle, nerve, bone, or joint disorders (Adams et al., 2004; Alperovitch-Najenson et al., 2004; Louhevaara et al., 2000; Merkies et al., 2003; Schreuders et al., 2000; Wessel et al., 1999). It has also been associated with bone mineral density, impaired cognition, and risk factors for cardiovascular disease in children and adolescents (Ortega et al., 2008; Ruiz et al., 2011). Handgrip strength has also been measured in preschool children (Bear-Lehman et al., 2002; Benefice et al., 1999; Molenaar et al., 2008; Robertson and Deitz, 1988), but it is not known whether it is associated with health outcomes in this population. Moreover, no detailed information about the protocol was provided in these earlier studies. The present study provides information to better standardize the procedure and increase its reliability. Without standardization and reliability, the measurement error may be too large to detect actual changes in strength after an intervention, for instance.
The findings of this study concur with previous reports in adults (Ruiz-Ruiz et al., 2002; Trampisch et al., 2012), adolescents (Ruiz et al., 2006b), and in children (Espana-Romero et al., 2008), which shows that there is an optimal grip span to measure handgrip strength, and that this grip span is reliable. Preschool children have smaller hand sizes and lower handgrip strength compared with older children, adolescent and adults (Bear-Lehman et al., 2002; Ploegmakers et al., 2013). Because of these differences, one would expect that each age group may need a different optimal grip span when measuring handgrip strength (Ortega et al., 2015). We observed that the optimal grip span in preschool children is similar to that observed in children aged 6–12 years with a hand size of 15 or 16 cm (Espana-Romero et al., 2008). España-Romero et al. (2008) showed that the optimal grip span observed in children aged 6–12 years with a hand size of 15 or 16 cm ranged between 4.0 and 4.4 cm. Interestingly, in the present study, we observed similar levels of handgrip strength when the test was carried out with a grip span of 4.0 and 4.5 cm in preschool children with a hand size of 15 or 16 cm.
We observed that the optimal grip span was not influenced by children’s hand size, as has also been shown in adult men (Ruiz-Ruiz et al., 2002). We do not know whether handgrip strength levels would have been higher at smaller grip spans because the dynamometer used in the present study did not allow setting grip spans smaller than 4.0 cm. Future studies should examine the optimal grip span using a dynamometer model with smaller grip spans in this population group. Meanwhile, as there is a clear need to standardize handgrip strength measures in fitness studies in preschool children, our results are useful to standardize measurements carried out with currently available dynamometers.
The Jamar hand dynamometer (Fit System Inc., Calgary, Canada) is probably the dynamometer that is most used in the clinical setting and in research. However, we decided to use the TKK dynamometer (TKK model 5001, Grip-A, Takei, Tokyo, Japan) based on previous findings that showed higher criterion-related validity and reliability when comparing the TKK model with the Jamar and DynEX (MD System, Inc., Westerville, OH, USA) dynamometers (Espana-Romero et al., 2010).
One strength of this study is the relatively large sample size, which allowed us to conduct the analysis by gender, age, and hand size groups. We observed however, a higher variation in handgrip strength in the groups with a hand size of 12 and 16 cm, which might be explained by the smaller sample size compared with the other groups. Whenever possible, future studies should increase the sample size, especially in children with these hand sizes. The study sample was not designed to statistically represent the whole population of Spanish preschool children; however there are no reasons to believe that the children participating in this study are different from other Spanish children of the same age. It must be borne in mind that different kinds of dynamometers and postures might change the results. We do not know whether these findings can be directly transferred to measurements with other dynamometers.
Footnotes
Acknowledgements
We thank the children who participated in the study, and their parents and teachers for their collaboration. We also thank the schools for their support to the study: C.P. Juan XXIII Chana (Granada), C.P. Carlos III (La Carolina, Jaén), C.P. Palacios Rubio (La Carolina, Jaén), C.P. Carlos III (Santa Elena, Jaén), Dulce Nombre de María PP. Escolapios (Granada).
Conflict of interests
None declared.
Ethical approval
The study protocol was performed in accordance with the ethical standards (Declaration of Helsinki, revised in 2013) and was approved by the University of Granada Review Committee for Research Involving Human Subjects.
Funding
The study was partially supported by the Spanish Ministry of Economy and Competitiveness [RYC-2011-09011, RYC-2010-05957 and BES-2014-068829] and the Spanish Ministry of Education, Culture and Sports [FPU 13/04365 and Beca de colaboración 8505733].