
Abstract

Dear Sir,
We describe an external circumferential glove reduction (ECGR) technique that has been used successfully by a single surgeon (BHM) to help closed reduction of phalangeal fractures prior to closed (percutaneous) K-wire fixation (Figures 1–3, Video 1 available online). The fracture patterns should have a longitudinal or oblique axis, or be ‘pilon-type’.
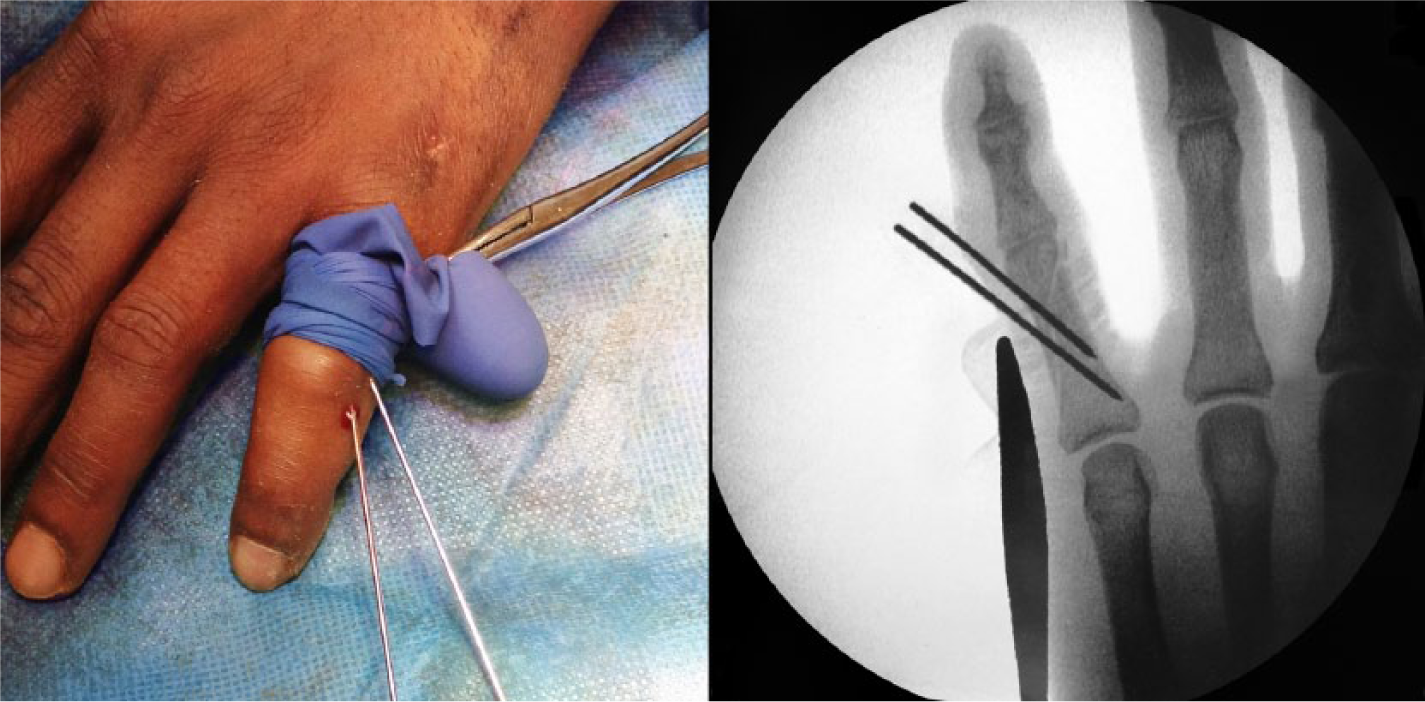
Intra-operative photograph (left) and radiograph (right) of the ECGR technique.
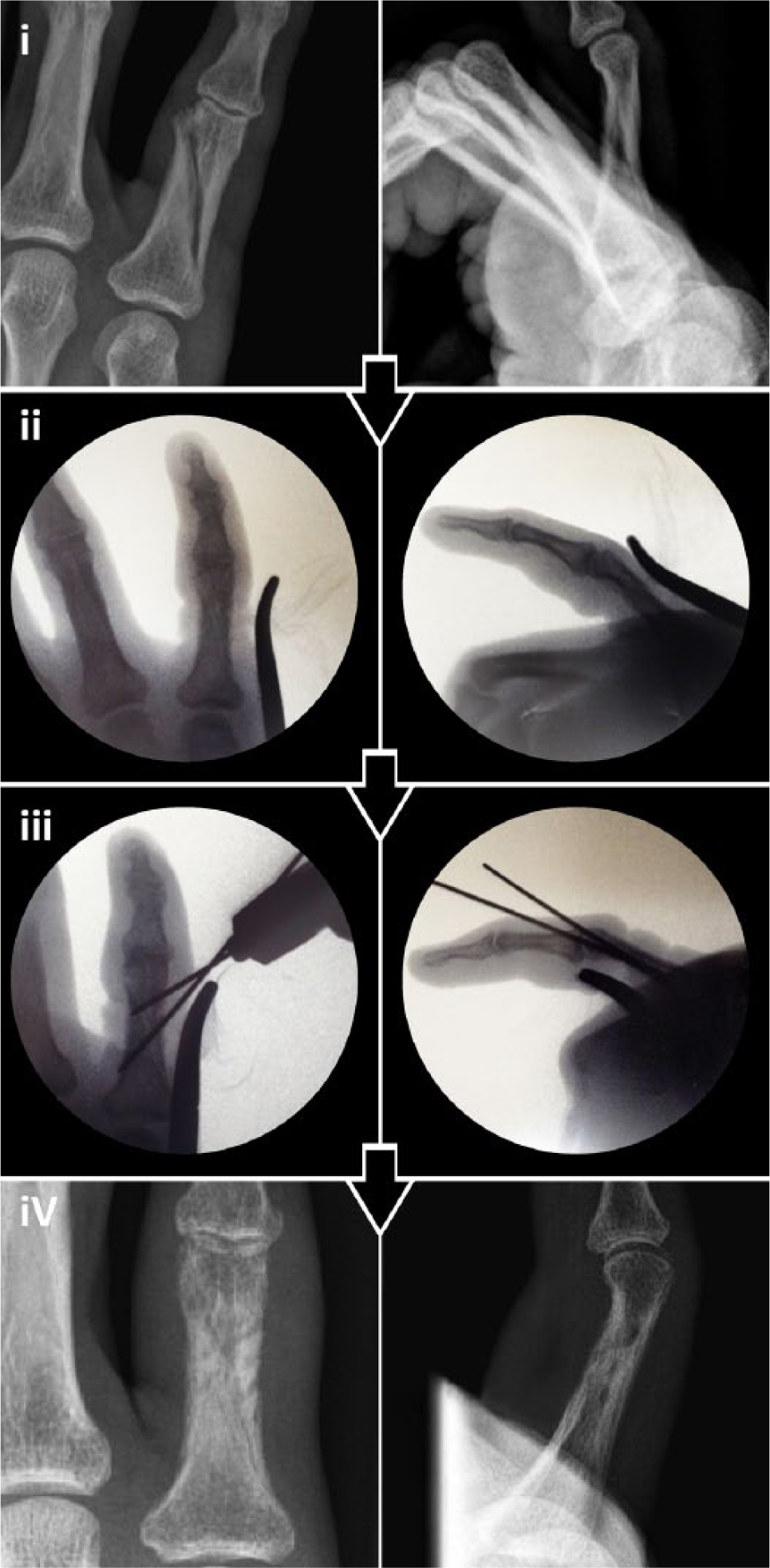
A representative case of K-wiring. (i) Pre-operative radiographs. (ii) Proximal-distal glove application after manual reduction (Video 1, available online). (iii) Evaluation of space for accurate K-wire fixation. (iv) Post-operative radiographs at 6 weeks.
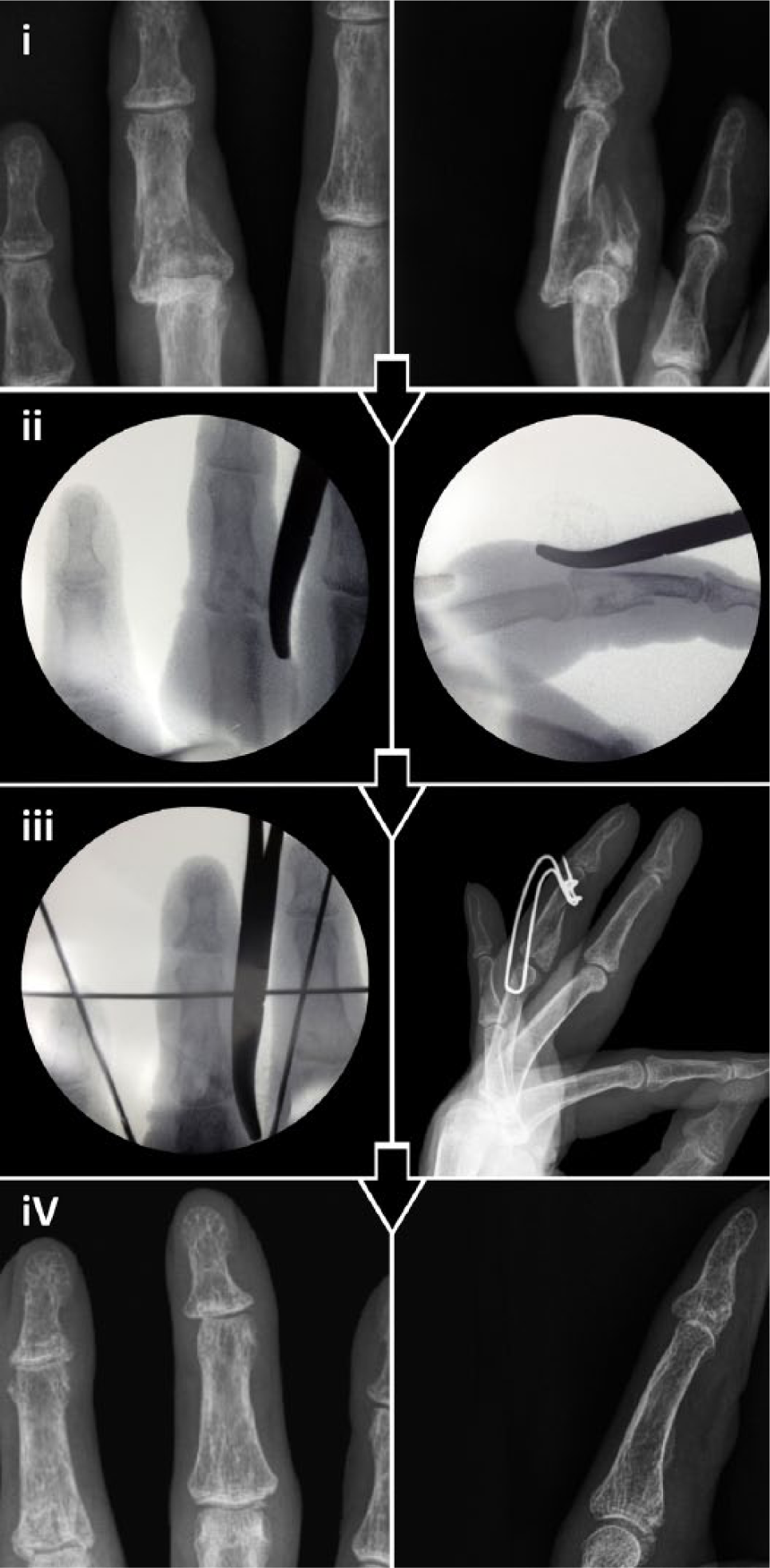
A representative case of application of a distraction frame. (i) Pre-operative radiographs. (ii) Proximal-distal glove application after manual reduction (Video 1, available online). (iii) Evaluation of space for accurate distraction frame application. (iv) Post-operative radiographs at 10 weeks.
Technique
One ‘digit’ is cut from a sterile glove and applied circumferentially, from proximal to distal, around the fracture site, which has been partially reduced with traction (Video 1, available online). The glove ends are clamped flush to the glove that is now wrapped around the digit, thereby providing stable reduction. Sufficient space should be allowed either side of the glove for proximal or distal K-wire placement. Care must be taken to ensure that K-wires are not driven through the glove, which could potentially introduce foreign material into the digit (Figures 2 and 3). Once the reduced fracture is secured with K-wires, the glove digit is removed and the finger dressed appropriately. Hand therapy-guided early active mobilization was commenced at a mean of 3 days post-operatively; K-wires were removed at a mean of 4 weeks post-operatively.
Assessment
Objectively the hand therapists measured jointranges of motion (Table 2) (Kleinert and Verdan, 1983; Libberecht et al., 2006). Subjectively, three Consultants, who were ‘blind’ to the procedure, assessed post-operative radiographs within 7 days after surgery at a weekly trauma meeting; posterior-anterior and lateral radiographs were examined for acceptable reduction, defined by straight alignment with cortical contact and articular congruity. Return to normal activity and any ongoing symptoms or issues were assessed by a hand therapy telephone follow-up at a mean of 6 months (range 5–7) post-operatively.
We treated 33 patients with a mean age of 42 years (standard error of mean (SM) ±2.6 years) (Table 1). There were 19 men and 14 women. One patient was treated for a thumb injury and was excluded from total active motion calculations; at discharge they had a Kapandji score of 8. Of the remaining 32 patients, we treated 22 oblique, three spiral, one comminuted distal phalangeal base fracture(s), and one fracture subluxation with K-wires and five pilon-type fractures with distraction frames (Table 1, Figure 3). A total of27 patients were followed-up by the hand therapy department fully to a mean of 3.9 months (SM ±0.3 months). The mean total active motion was 87% (range 72–99%) (Table 2). Six patients were excluded from total active motion calculations due to non-attendance. Of the 27 patients, 26 were contactable by phone; all reported a return to normal activity in that there were no tasks in the post-rehabilitation period that patients could not perform as compared with the pre-injury period. Furthermore, all 24 employed patients had returned to their original work. Only three patients reported episodic mild and improving joint tenderness with heavy use. No further complications, symptoms, or issues were reported, either during hand therapy follow-up or at telephone contacting.
Patient demographics, associated fracture patterns and fixation methods employed using ECGR.
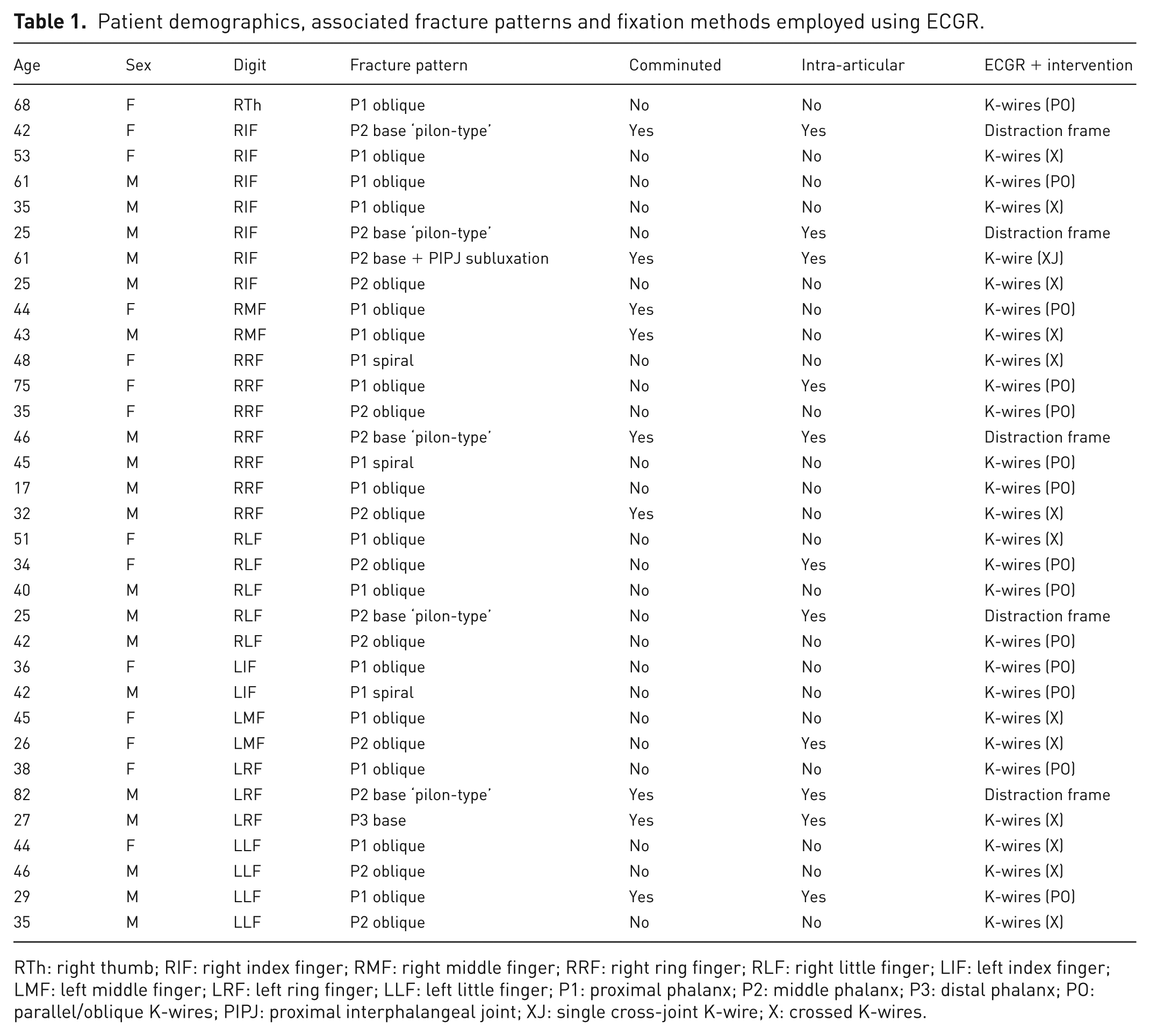
RTh: right thumb; RIF: right index finger; RMF: right middle finger; RRF: right ring finger; RLF: right little finger; LIF: left index finger; LMF: left middle finger; LRF: left ring finger; LLF: left little finger; P1: proximal phalanx; P2: middle phalanx; P3: distal phalanx; PO: parallel/oblique K-wires; PIPJ: proximal interphalangeal joint; XJ: single cross-joint K-wire; X: crossed K-wires.
Mean joint ranges of motion at final hand therapy assessment.
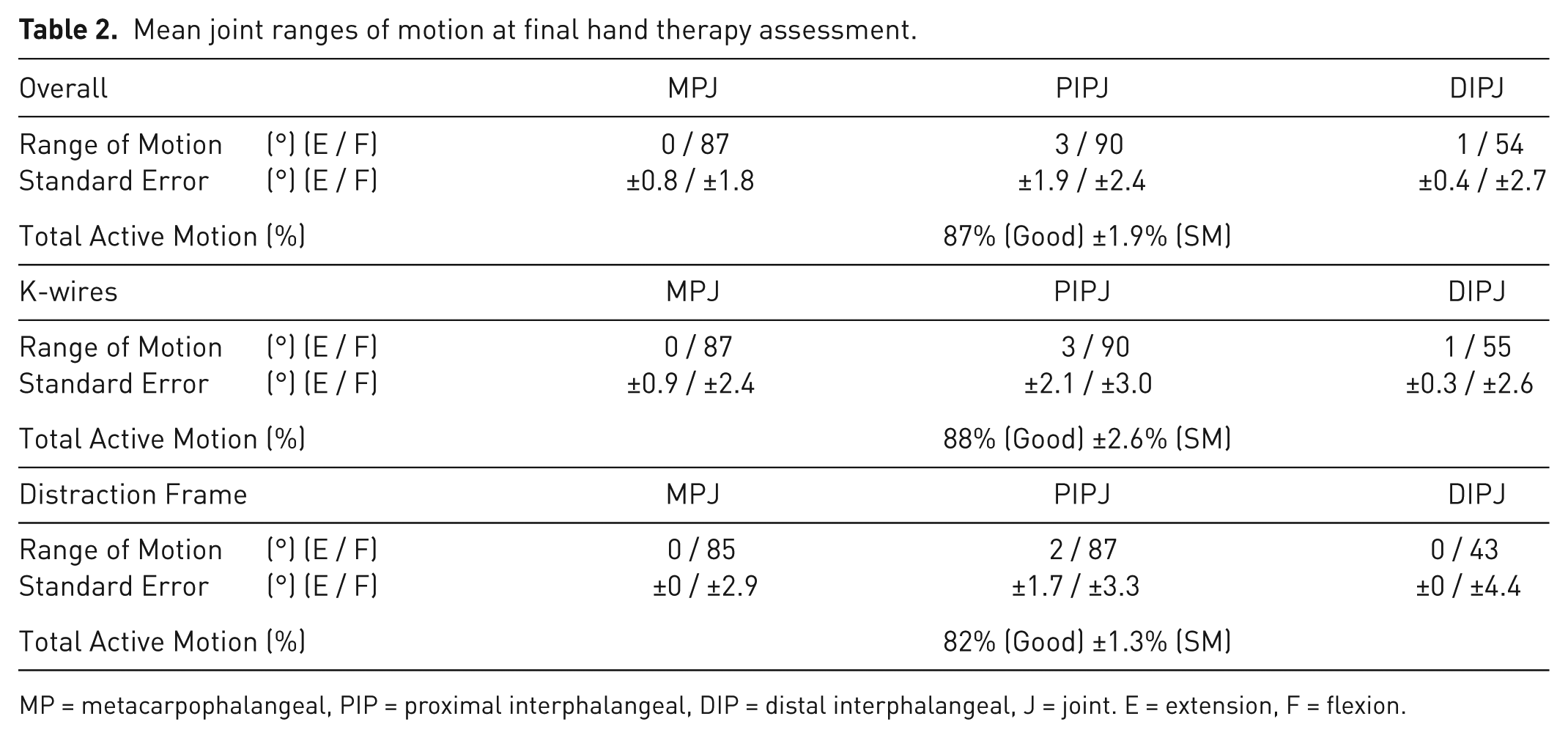
MP = metacarpophalangeal, PIP = proximal interphalangeal, DIP = distal interphalangeal, J = joint. E = extension, F = flexion.
Reducing and maintaining closed reduction of phalangeal fractures can be quite difficult, especially while avoiding irradiation of the surgeon’s own hand or avoiding damaging the skin and other soft tissues with sharp clamps. ECGR preserves sufficient space for efficient and unencumbered K-wire placement. Nonetheless care must be taken to ensure that K-wires are not driven through the glove material, which could potentially introduce foreign material into the digit. The ECGR technique has been found to be extremely useful in assisting more accurate and efficient closed reduction and percutaneous K-wire fixation of phalangeal hand fractures.
Footnotes
Declaration of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.