
Abstract
The aim of this study was to perform a systematic review in order to identify predictors of secondary displacement in distal radius fractures. We performed a systematic review and identified all studies that reported secondary displacement following distal radius fractures. Where possible, we pooled the odds ratios of predictors. The initial search yielded 3178 studies of which 27 were included. Multiple studies found that age, shortening, volar comminution, loss of radial inclination, the presence of a volar hook, AO type 3 fractures (A3, B3, C3) and the Older classification were significant predictors of secondary displacement. Pooling revealed a significantly increased risk of secondary displacement in fractures with dorsal comminution, in women and in patients aged >60 years. An associated ulna fracture or intra-articular involvement does not result in an increased risk of secondary displacement. The overview provided in this study can help surgeons to inform patients of the chances of success of closed treatment regarding the radiological outcome and facilitate shared decision making.
Keywords
Introduction
Initial treatment of patients with distal radius fractures generally consists of closed reduction and plaster immobilization (Arora et al., 2012; Earnshaw et al., 2002; Kumar et al., 2008; Mackenney et al., 2006). However, fracture re-displacement following closed reduction occurs in up to 64% of the patients (in part depending upon the definition) (Jenkins, 1989; Mackenney et al., 2006; Makhni et al., 2008). Most surgeons would agree that distal radius fractures with re-displacement outside acceptable parameters (>10° dorsal angulation, radial shortening >3 mm or intra-articular step-off) (American Academy of Orthopaedic Surgeons Board of Directors, 5 December 2009) benefit from surgical fixation, taking into account patient-related factors.
Patients with a distal radius fracture with a perceived high risk of re-displacement may be recommended primary surgical treatment. Unfortunately, patients with these potentially more unstable distal radius fractures are difficult to identify.
In 1989, Lafontaine et al. identified five factors predictive of fracture instability: dorsal angulation exceeding 20° at presentation; dorsal comminution; extension of the fracture into the radiocarpal joint; an associated ulnar fracture; and age over 60 years (Lafontaine et al., 1989). According to Lafontaine et al. (1989), a fracture can be considered potentially unstable if three or more factors are present.
Since then, several studies have confirmed and refuted the importance of these five risk factors, and new clinical and radiological predictors have been identified (Abbaszadegan et al., 1989; Nesbitt et al., 2004; Poigenfürst, 1980; Tahririan et al., 2013). Other authors have quantified predictors and presented scoring systems to predict the risk of secondary displacement based on clinical and radiological variables (Adolphson et al., 1993; Mackenney et al., 2006).
Although several risk factors of secondary displacement are commonly accepted, the evidence for some predictors is limited. An overview of all known predictors of fracture instability in literature, and their relative weight (pooled odds ratios), could assist physicians in decision making regarding the optimal method of treatment for patients with distal radius fractures.
The aim of this study was to perform a systematic review in order to identify predictors of secondary displacement in distal radius fractures.
Methods
This review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2010). A review protocol was drafted and registered on PROSPERO with number CRD42014010828. All of the following steps were performed by two independent reviewers (SA and MMJW). Disagreements between the two reviewers were discussed until a consensus was reached.
Eligibility criteria systematic review
Any study that could potentially provide information on predictors of secondary displacement was eligible for inclusion. Therefore, studies describing non-operative treatment in patients with distal radius fractures were also included. We anticipated that these studies would report secondary displacement during follow-up.
Inclusion criteria were studies that addressed adult (18 years and older) patients with distal radius fractures initially treated with plaster immobilization, with or without closed reduction of the fracture. Reviews, animal studies, cadaver studies, case reports, surveys, current (management) concepts, editorials, commentaries, conference abstracts and letters were excluded. Since there are numerous definitions of displacement and instability, we did not predetermine a definition that should have been used for a study to be included. For the same reason we did not define what constitutes a displaced, undisplaced or minimally displaced fracture.
Eligibility criteria meta-analysis
For the meta-analysis, an additional inclusion criterion was studies that reported odds ratios of predictors of secondary displacement, or provided sufficient information to calculate odds ratios. We required studies to have had a minimal radiological follow-up of 4 weeks for the assessment of secondary displacement.
Literature search and study selection
We conducted a systematic search of the MEDLINE and EMBASE databases on 28 August 2013, and updated the search on 19 March 2015 (Appendix 1, available online), to identify all studies on patients with distal radius fractures and reporting displacement or fracture instability. To ensure proper interpretation of the results by our team, publication language was restricted to English, German, Spanish, French, Turkish or Dutch. The resulting titles and abstracts were reviewed. If the eligibility criteria were met, full manuscripts were procured and reviewed. The bibliographies of all included studies were manually screened for additional articles of interest.
Data extraction
Data were extracted using a standardized data collection form that was developed according to the Cochrane guidelines (Higgins and Green, 2011). Items collected included publication details, study type, numbers of patients, fracture types, the definition of displacement, the type of statistical analysis and details regarding treatment. For each study we determined which predictors of secondary displacement were found statistically significant (p < 0.05). Additionally, we assessed if the predictor was tested in a univariate or a multivariable analysis. For the meta-analysis, predictors and odds ratios or coefficients of predictors of secondary displacement were obtained and collected in a database.
Quality assessment
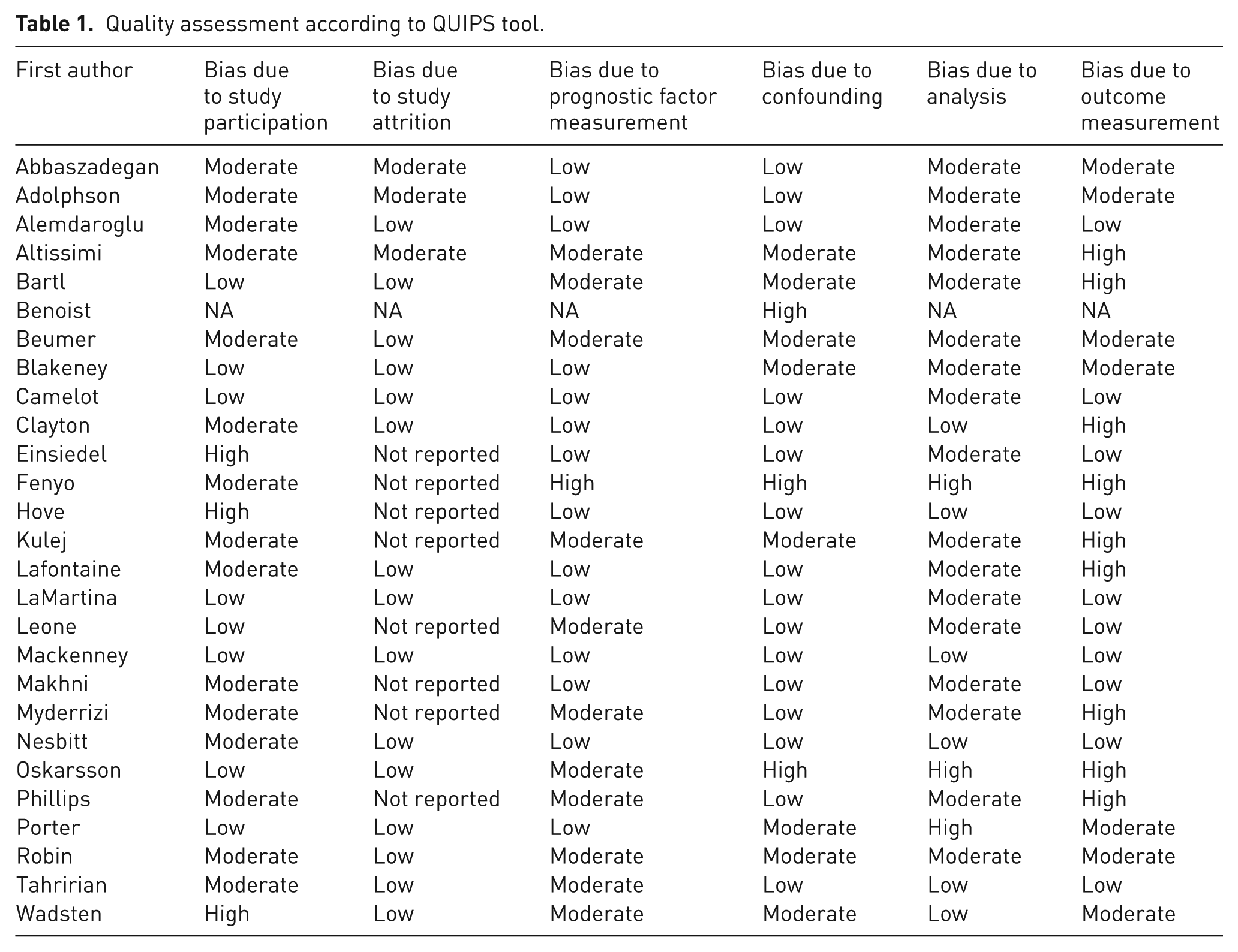
Quality and heterogeneity across studies was assessed using the Quality in Prognostic Studies (QUIPS) tool (Hayden et al., 2013; Huguet et al., 2013) (Table 1 and Appendix 2, available online). The QUIPS tool rates individual studies according to the potential risk of bias associated with six domains: (1) study participation; (2) study attrition; (3) prognostic factor measurement; (4) outcome measurement; (5) confounding measurement and account; and (6) analysis. Two reviewers (SA and MMJW) independently assessed the potential risk of basis of each study based on information available in the manuscripts. Disagreements were discussed by the reviewers until a consensus was reached.
Quality assessment according to QUIPS tool.
Synthesis of results of meta-analysis
For the meta-analysis, univariate odds ratios were pooled using the random effects model. The random effects model involves an assumption that the effects being estimated in the different studies are not identical, but follow some distribution (Higgins and Green, 2011). If coefficients from a logistic regression analysis were reported, odds ratios were calculated by taking the exponential. Odds ratios for instability or displacement at any point during follow-up (early or late) were added as separate odds ratios to the analysis. Data were pooled with the log odds ratio and the standard error with the generic inverse variance.
To test the robustness of the results, sensitivity analyses were performed by comparing the results obtained with the random effects model with the fixed effects models (Higgins and Green, 2011). Similar results imply that the results are robust.
Statistical heterogeneity for each analysis was tested with I2. The I2 is a statistic that indicates the percentage of variance and is qualified as follows: 0% to 40% (might not be important); 30% to 60% (may represent moderate heterogeneity); 50% to 90% (may represent substantial heterogeneity); 75% to 100% (considerable heterogeneity) (Higgins and Green, 2011).
Results
Search results
The initial search yielded a total of 3178 studies, of which 2249 remained after excluding the duplicates. The full text manuscripts of 133 studies were evaluated and 27 studies were included in the systematic review (Figure 1) (Abbaszadegan et al., 1989; Adolphson et al., 1993; Alemdaroglu et al., 2010; Altissimi et al., 1994; Bartl et al., 2014; Benoist and Freeland, 1995; Beumer and McQueen, 2003; Blakeney and Webber, 2009; Camelot et al., 1998; Clayton et al., 2009; Einsiedel et al., 2009; Fenyo and Johansson, 1974; Hove et al., 1994; Kulej et al., 2007; Lafontaine et al., 1989; LaMartina et al., 2015; Leone et al., 2004; Mackenney et al., 2006; Makhni et al., 2008; Myderrizi, 2011; Nesbitt et al., 2004; Oskarsson et al., 1997; Phillips and Al-Shawi, 2014; Porter and Stockley, 1987; Robin et al., 2014; Tahririan et al., 2013; Wadsten et al., 2014). The full text manuscript of one study could not be procured, even after contacting the authors (Plaweski S et al., 1997).
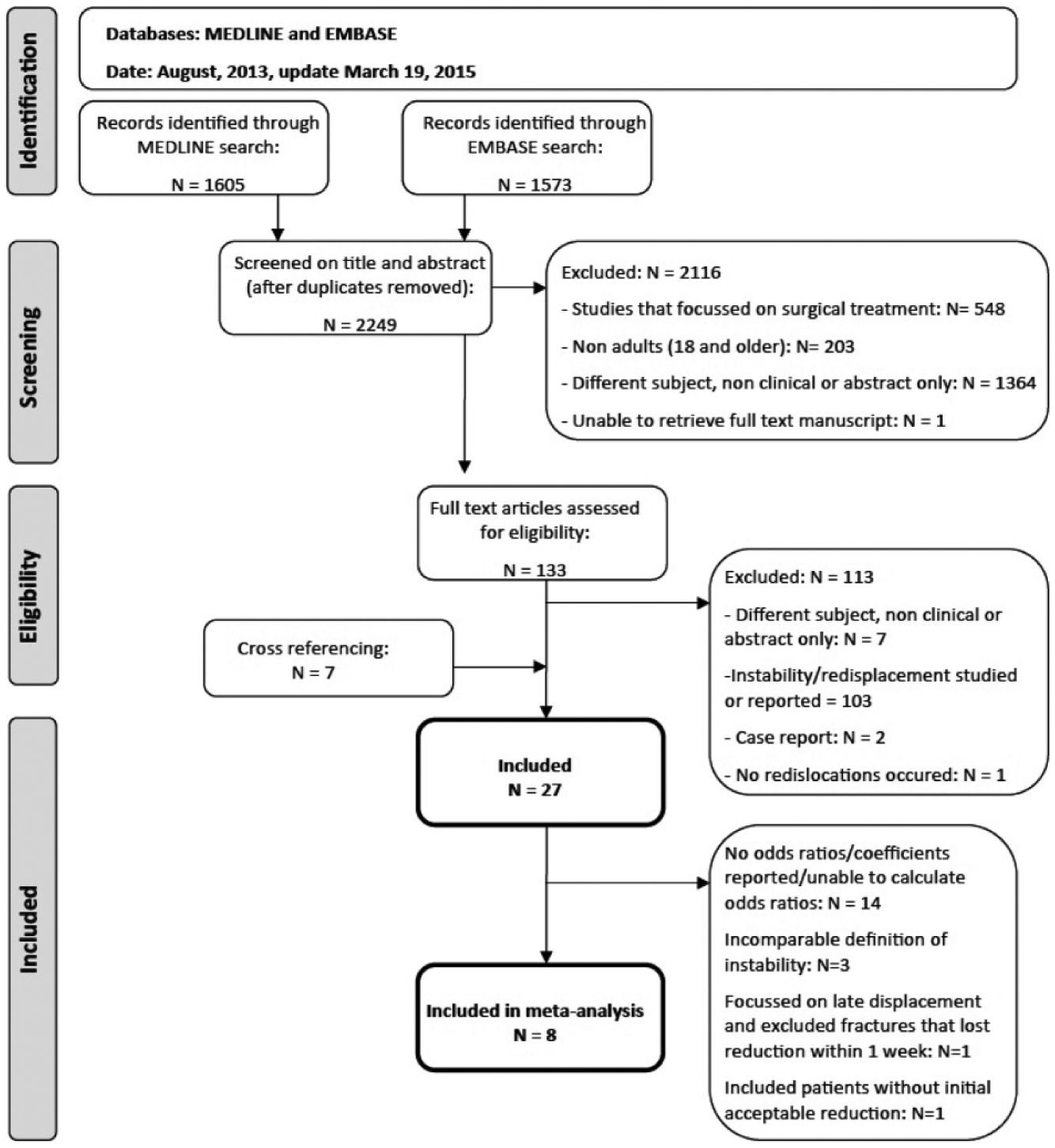
Flowchart.
Systematic review
The characteristics of the studies included are outlined in Table 2. All but three studies focused primarily on secondary displacement or radiographic outcome (Bartl et al., 2014; Oskarsson et al., 1997; Porter and Stockley, 1987). One study excluded fractures that lost reduction within 1 week and assessed late secondary displacement at 2 months (Myderrizi, 2011). Quality and risk of bias were variable (Table 1 and Appendix 2, available online).
Characteristics of studies included (N = 27).
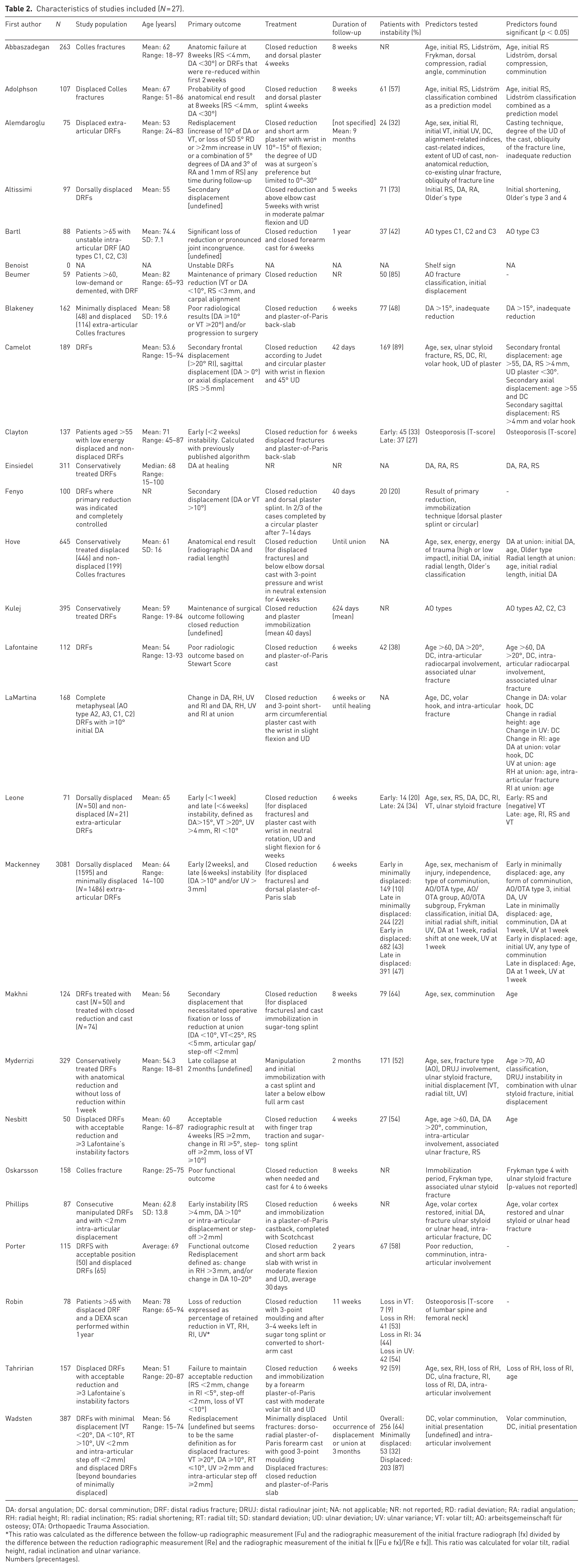
DA: dorsal angulation; DC: dorsal comminution; DRF: distal radius fracture; DRUJ: distal radioulnar joint; NA: not applicable; NR: not reported; RD: radial deviation; RA: radial angulation; RH: radial height; RI: radial inclination; RS: radial shortening; RT: radial tilt; SD: standard deviation; UD: ulnar deviation; UV: ulnar variance; VT: volar tilt; AO: arbeitsgemeinschaft für osteosy; OTA: Orthopaedic Trauma Association.
This ratio was calculated as the difference between the follow-up radiographic measurement (Fu) and the radiographic measurement of the initial fracture radiograph (fx) divided by the difference between the reduction radiographic measurement (Re) and the radiographic measurement of the initial fx ([Fu e fx]/[Re e fx]). This ratio was calculated for volar tilt, radial height, radial inclination and ulnar variance.
Numbers (precentages).
A total of 7574 patients were included. Secondary displacement occurred in 10% to 89% of the fractures. A total of 44 different predictors of secondary displacement were reported. An overview of the most common predictors and in which study they were assessed is outlined in Table 3.
Overview results of each study for the most common predictors.
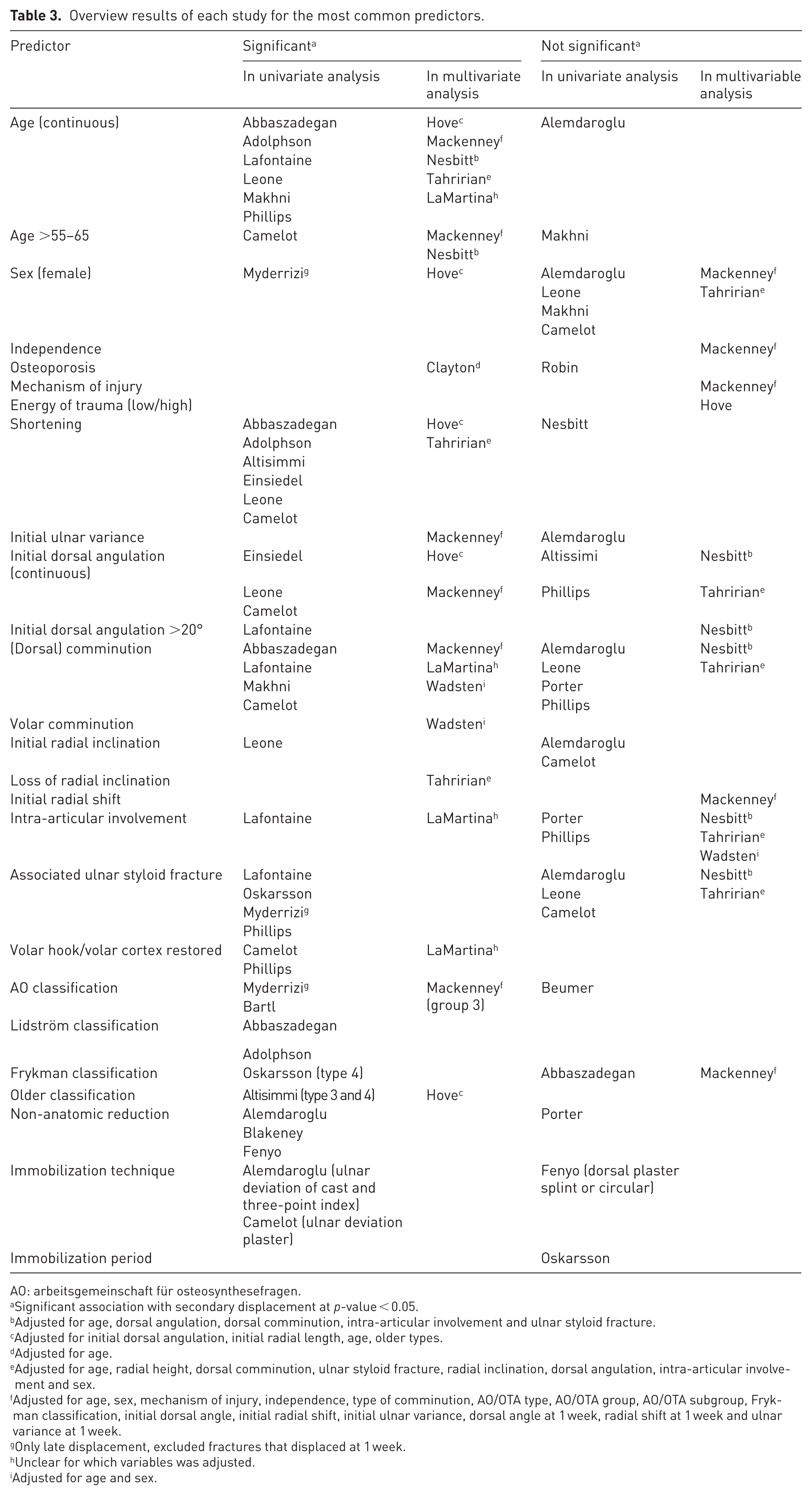
AO: arbeitsgemeinschaft für osteosynthesefragen.
Significant association with secondary displacement at p-value < 0.05.
Adjusted for age, dorsal angulation, dorsal comminution, intra-articular involvement and ulnar styloid fracture.
Adjusted for initial dorsal angulation, initial radial length, age, older types.
Adjusted for age.
Adjusted for age, radial height, dorsal comminution, ulnar styloid fracture, radial inclination, dorsal angulation, intra-articular involvement and sex.
Adjusted for age, sex, mechanism of injury, independence, type of comminution, AO/OTA type, AO/OTA group, AO/OTA subgroup, Frykman classification, initial dorsal angle, initial radial shift, initial ulnar variance, dorsal angle at 1 week, radial shift at 1 week and ulnar variance at 1 week.
Only late displacement, excluded fractures that displaced at 1 week.
Unclear for which variables was adjusted.
Adjusted for age and sex.
Only a few predictors were also tested in a multivariable analysis, adjusting for other covariates. Of these, age, shortening, volar comminution, loss of radial inclination, the presence of a volar hook, AO type 3 fractures (A3, B3, C3) and the Older classification were found to be significant predictors in one or more studies.
The mechanism of the injury, the forces involved, i.e. the estimated energy of the injury, the independence of a patient (defined as being able to go shopping), initial dorsal angulation >20° from neutral, the initial radial shift, the presence of an associated ulnar styloid fracture and the Frykman classification were revealed not to be significant predictors of secondary displacement in one or more studies that adjusted for other covariates. For gender, initial ulnar variance, comminution and intra-articular involvement, there were studies that found a significantly increased risk of secondary displacement and others that did not.
Meta-analysis
We were able to extract or calculate odds ratios from 11 articles (Alemdaroglu et al., 2010; Bartl et al., 2014; Blakeney and Webber, 2009; Hove et al., 1994; Lafontaine et al., 1989; Leone et al., 2004; Mackenney et al., 2006; Makhni et al., 2008; Myderrizi, 2011; Nesbitt et al., 2004; Tahririan et al., 2013). We contacted the corresponding authors of four additional articles that reported p-values without odds ratios or only adjusted odds ratios to request additional information (Camelot et al., 1998; LaMartina et al., 2015; Phillips and Al-Shawi, 2014; Wadsten et al., 2014). The authors of two studies provided further data (Phillips and Al-Shawi, 2014; Wadsten et al., 2014) so we could extract or calculate odds ratios from 13 studies. Ten of these studies used a comparable definition for secondary displacement and were therefore eligible for pooling (Alemdaroglu et al., 2010; Blakeney and Webber, 2009; Leone et al., 2004; Mackenney et al., 2006; Makhni et al., 2008; Myderrizi, 2011; Nesbitt et al., 2004; Phillips and Al-Shawi., 2014; Tahririan et al., 2013; Wadsten et al., 2014). Myderrizi (2011) excluded patients with loss of reduction at 1 week and this study was therefore not included in the analysis. Wadsten et al. (2014) also analysed the 92 patients who went on to surgery because their post reduction films revealed an unacceptable position, and therefore we did not include this study. From the remaining eight articles, we were able to pool the odds ratios of seven predictors. A total of 3807 patients were analysed.
Female gender, age >60–65 years and dorsal comminution were significant predictors of secondary displacement (Figures 2–4). An associated ulnar styloid fracture, intra-articular involvement, dorsal angulation >15° from neutral and dorsal angulation >20° from neutral were not significantly associated with secondary displacement (Figure 5–8).
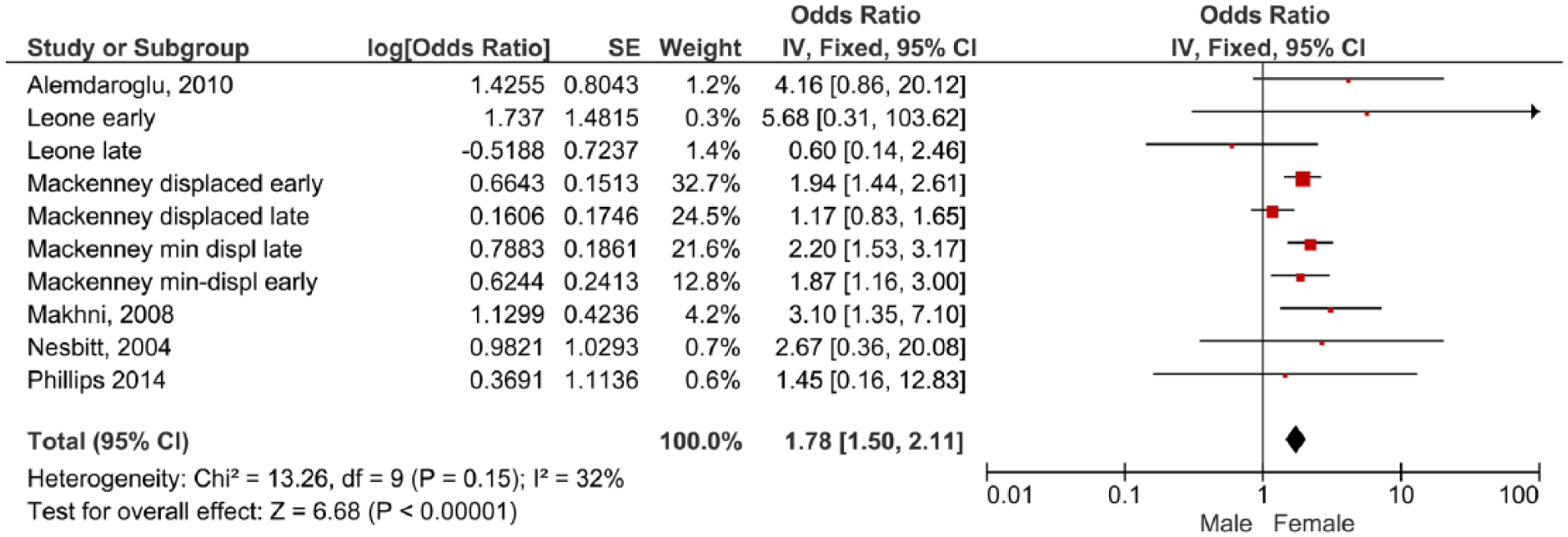
Forest plot of comparison female versus male. The four odds ratios from Mackenney et al. (2006) represent early and late instability in minimally displaced and displaced fractures. The odds ratios from Leone et al. (2004) represent early and late instability in all fractures.
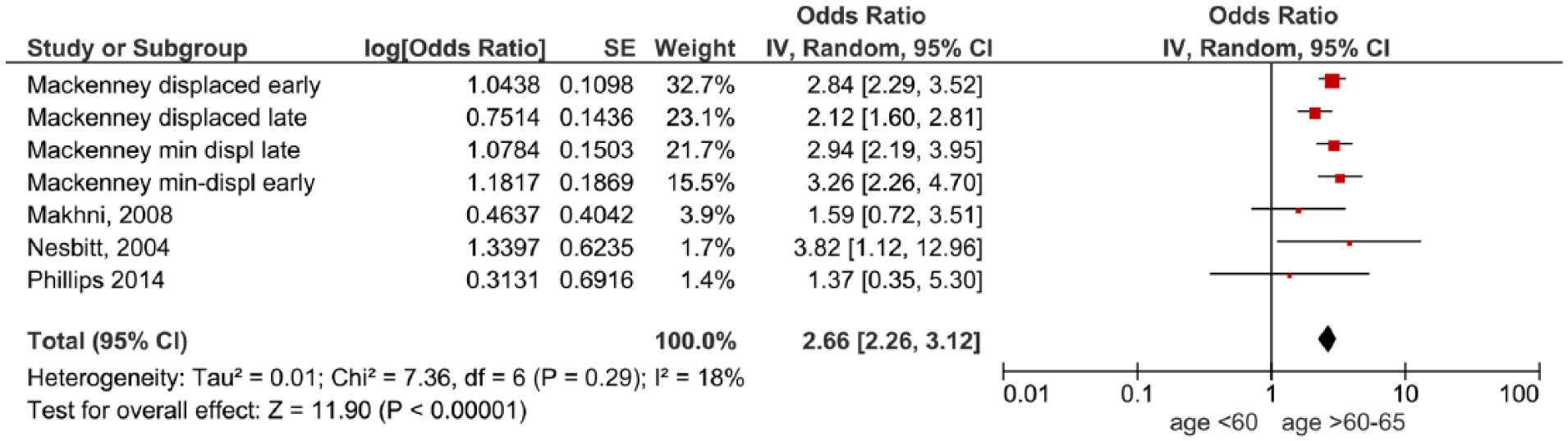
Forest plot of comparison age >60 years versus <60–65 years. Mackenney et al. (2006) represent early and late instability in minimally displaced and displaced fractures.
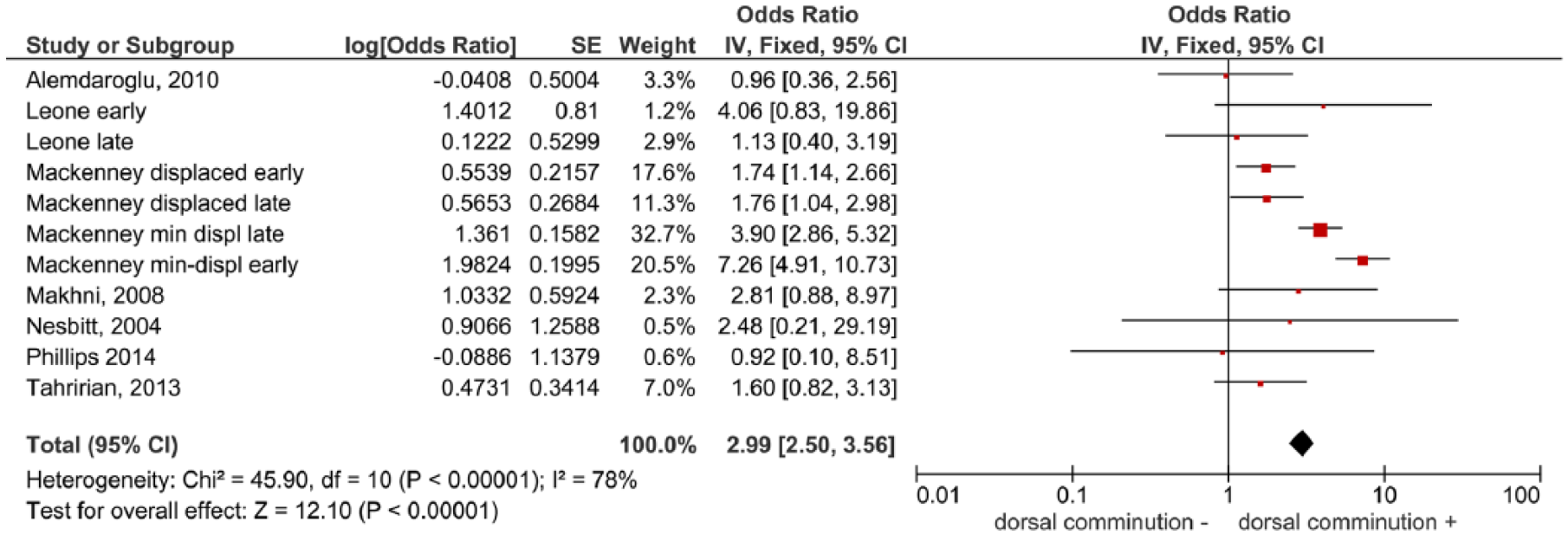
Forest plot of comparison dorsal comminution versus no comminution. The four odds ratios from Mackenney et al. (2006) represent early and late instability in minimally displaced and displaced fractures. The odds ratios from Leone et al. (2004) represent early and late instability in all fractures.
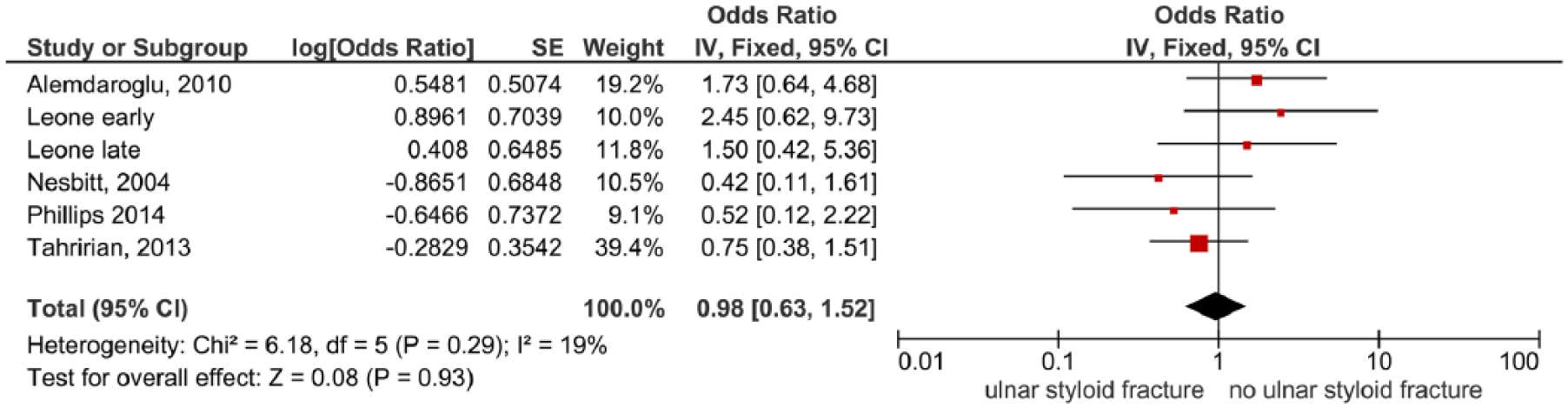
Forest plot of comparison presence of associated ulnar styloid fracture versus intact ulnar styloid. The odds ratios from Leone et al. (2004) represent early and late instability in all fractures.

Forest plot of comparison intra-articular fracture involvement versus no involvement.

Forest plot of comparison dorsal angulation >15° from neutral versus dorsal angulation ⩽15° from neutral.

Forest plot of comparison dorsal angulation >20° from neutral versus dorsal angulation ⩽20° from neutral.
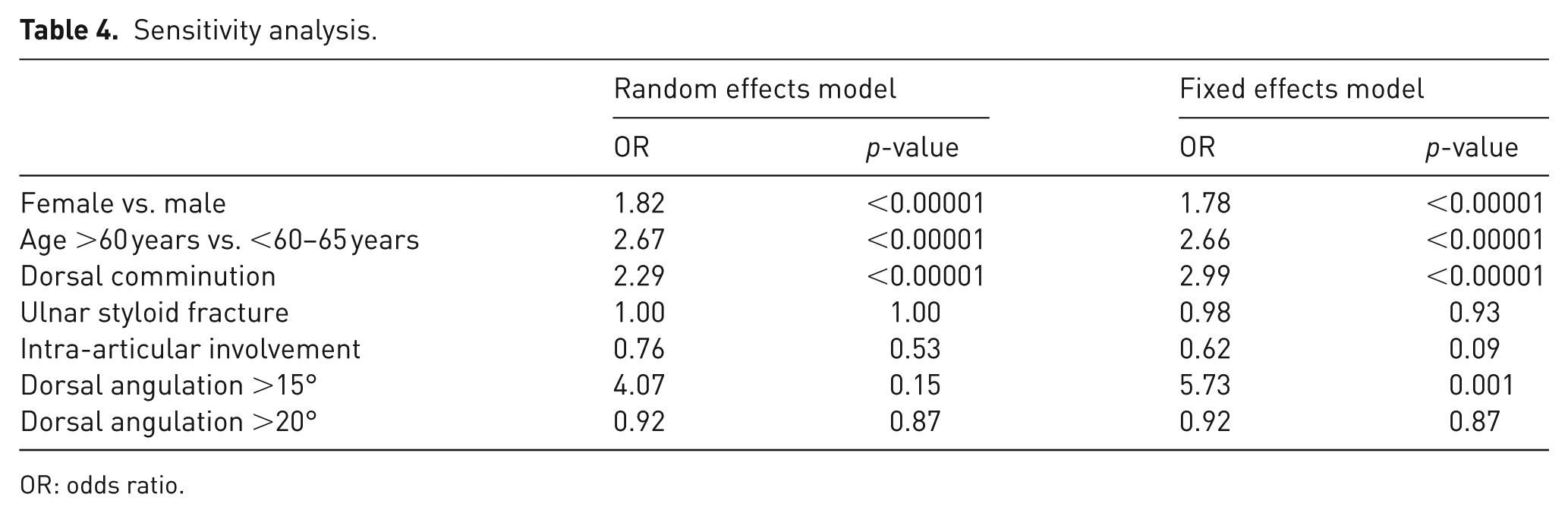
A sensitivity analysis showed similar estimates in the random and fixed effects models (Table 4). The odds ratio of intra-articular involvement and dorsal angulation >15° from neutral were both significant only in the fixed effects model.
Sensitivity analysis.
OR: odds ratio.
Discussion
This systematic review provides an overview of all predictors of secondary displacement of distal radius fractures in literature. We have demonstrated that not all popular predictors of instability that are persistently used in the literature have indeed been identified as significantly associated with secondary displacement. For instance, several studies that also adjusted for other covariates in their analyses did not find an increased risk of secondary displacement in fractures with an initial dorsal angulation exceeding 20° from neutral and neither in fractures with an associated ulnar styloid fracture.
For other popular risk factors, such as the female gender, dorsal comminution and intra-articular involvement, the results were inconclusive. Some studies with adjusted analyses did find a significant influence on secondary displacement and others did not.
In an attempt to provide a definite answer, we pooled the odds ratios of seven predictors, including gender, age >60–65, dorsal comminution, associated ulnar styloid fracture, intra-articular involvement and dorsal angulation exceeding 15° and 20° from neutral. Our results show a significantly increased risk of secondary displacement in fractures with dorsal comminution and in women. Additionally, the pooled results confirm the importance of age, demonstrating a significantly increased risk of secondary displacement of distal radius fractures in patients older than 60–65 years.
Conversely, our analysis reveals no significantly increased risk of secondary displacement in fractures with a dorsal angulation exceeding 15° or 20° from neutral, an associated ulna fracture or intra-articular involvement.
Intra-articular involvement is often mentioned as an indication for surgery and is one of Lafontaine’s often cited risk factors (American Academy of Orthopaedic Surgeons Board of Directors, 5 December 2009; Mackenney et al., 2006; Makhni et al., 2008). Nevertheless, we found no significant effect on secondary displacement of intra-articular fractures (0.52, p = 0.07). When the fixed effects model was used, risk of secondary displacement in intra-articular fractures was significantly lower (OR 0.5, p = 0.03). An explanation for this is that in the fixed-effects analyses, studies are weighted less equally than in the random effects. Therefore, the larger study of the two (that found a significant OR) has greater weight (Higgins and Green, 2011). Another possible reason could be that patients with more severe intra-articular fractures received primary operative treatment, resulting in less severe intra-articular fractures in the study population. The same reason may explain why dorsal angulation >15° from neutral was significant in the fixed-effects model and not in the random-effects model.
Another of Lafontaine’s risk factors is the presence of an associated ulnar styloid fracture, which is believed to result in injuries of the ulnocarpal ligaments and therefore constitute fracture instability (Poigenfuerst and Tuchmann, 1978; Poigenfürst, 1980). However, despite its popularity, this predictor was not identified as significantly associated with secondary fracture displacement in multiple studies. This is confirmed by the results of our meta-analysis, which do not show an increased risk of secondary displacement for an associated ulnar styloid fracture.
The strength of this study is that it provides a complete and comprehensive overview of all predictors known in literature. There is a considerable advantage to the novel approach we took in this study to pool odds ratios of predictors. This is especially demonstrated by the pooled results for gender and dorsal comminution. Table 3 shows evidence for both predictors seems inconclusive; however, by pooling we found that both are significantly associated with secondary displacement. Gender is not commonly addressed in popular definitions of an unstable distal radius fracture (Cooney et al., 1979; Lafontaine et al., 1989; Poigenfürst, 1980). Moreover, gender has been refuted as a predictor by several studies (Table 3). It is possible that by pooling, we identified a predictor that did not previously reach significance due to small study sizes. Nevertheless, the effect of female gender could be mitigated when accounting for age, because women reach a higher age than men and are more prone to suffer from osteoporosis. Thus the association between gender and fracture instability is probably indirect and should not be interpreted as direct causality.
This study has several limitations. The majority of studies that we included focused primarily on secondary displacement. Consequently, these studies only described patients who were treated conservatively. Patients treated initially with an operation were probably not included. This last group is likely to include the most unstable fractures. In our opinion, this limitation mostly applies to studies performed after the introduction of volar locking plates in 2000. Conversely, some patients might have been treated operatively who would have achieved excellent results with conservative treatment. Unfortunately, the decisions to perform primary surgical fixation and exclude these patients were only reported in a few studies. Intra-articular involvement, volar fracture displacement or open fractures were most commonly mentioned.
A limitation regarding the meta-analysis is the variation among study populations: four studies provided one common odds ratio for both non-displaced and displaced fractures; one study only provided odds ratios for displaced fractures; and one study reported separate odds ratios for displaced and minimally displaced fractures. We were unable to extract separate odds ratios for non-displaced and displaced fractures and therefore combined these data.
Of particular note is the definition of secondary displacement varied considerably across studies (Table 2). All studies included an alteration in dorsal angulation as a criterion of displacement in their definition. However, cut-off values varied from an absolute dorsal angulation of 10° or 15° from neutral to a change of 5°. The pooled odds ratios we found should therefore be interpreted with some caution.
Despite the obvious variability among studies, the statistical heterogeneity tests showed an I2 of 48% or less for all analyses but one. The heterogeneity for dorsal comminution was considerable (I2 = 78%). A possible explanation for this could be that the assessment of the presence of dorsal comminution was more subjective and variable across studies than other predictors, such as age and gender.
These limitations emphasize the need for consistency of definitions, measurement methods and a structured follow-up for patients with distal radius fractures. Standardization would allow easier comparison of studies and contribute to a higher level of evidence.
This systematic review provides a comprehensive overview of all known predictors and non-predictors of secondary displacement in patients with distal radius fractures. We have demonstrated that, despite their popularity as predictors of secondary displacement, distal radius fractures with an associated ulna fracture, a dorsal angulation >15° or >20° from neutral and intra-articular fractures do not have an increased risk of secondary displacement. We did find a significantly increased risk of secondary displacement for patients older than 60–65, women and fractures with dorsal comminution. Our results can provide a good basis for surgeons to inform patients on the probability of secondary displacement and therefore the chances of success from conservative treatment. This will facilitate shared decision making between patient and surgeon. Nevertheless, since secondary displacement does not always entail poor functional results after conservative treatment, especially in elderly patients (Bartl et al., 2014), future studies should focus on pooling important predictors of functional outcome.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.