
Abstract
We report the outcomes of repair of the flexor digitorum profundus tendon in zone 2a in 22 fingers. The tendon was repaired with a six-strand repair method and the A4 pulley was completely released. Release of the C2 pulley combined with the A4 pulley was necessary in 12 fingers, nine fingers underwent a complete release of the A3, C2, and A4 pulleys, and one finger underwent a release of the C1, A3, C2, and A4 pulleys. The mean total active motion of the three finger joints was 234° at 5 to 12 months of follow-up. No bowstringing was noted in these fingers. The good and excellent recovery of active digital motion was in 20 (91%) out of 22 fingers according to Strickland’s criteria or Tang’s criteria. Our results suggest that release of the A3, C2, and A4 pulleys makes the repair surgery easier and does not cause tendon bowstringing.
Introduction
Flexor tendon repair, particularly in zone 2, is still challenging. It is generally considered that the distal margin of the insertion of the flexor digitorum superficialis (FDS) tendon on the middle phalanx is the margin of the zone 2 (Strickland, 1985; Tang and Shi, 1992; Verdan, 1964). On the basis of anatomical study, Tang and Shi (1992) divided zone 2 into four subdivisions in consideration of the biomechanical and structural differences of each segment of the tendon inside this area. These subdivisions include zone 2a (from the distal margin to the proximal margin of the FDS insertion) and 2b (from the proximal margin of the FDS insertion to the distal edge of the A2 pulley). In repairing the flexor digitorum profundus (FDP) tendon in zone 2a, release of the A4 pulley is occasionally required to allow the placement of core suture and eliminate constriction of the oedematous repaired tendon (Kwai Ben and Elliot, 1998).
The aim of this study was to assess the outcome of release of the entire A4 pulley to facilitate zone 2 flexor tendon repair using a six-strand suture in the Yoshizu #1 technique (Moriya et al., 2015; Yoshizu, 1996), followed by early postoperative active mobilization.
Methods
Patients
We retrospectively analysed the medical records of patients with FDP lacerations in zone 2, with or without concomitant FDS lacerations, which were repaired at our institution between 1993 and 2014. The patients were identified via a search of the International Classification of Diseases-10 code S561 from our institution’s billing records. During this period, 83 patients (97 fingers) with complete zone 2 FDP lacerations were treated; 64 fingers in 52 patients had injuries at or around the A4 pulley. Patients with extensor tendon injuries, fractures, joint injuries, bilateral digital artery injuries, or skin defects were excluded from the study; however, patients with other neurovascular injuries were included. Using Tang’s subdivisions of zone 2 (Figure 1), there were 22 fingers with zone 2a injuries and 42 fingers with zone 2b injuries. Of these, the A4 pulley was partially or completely released in 48 fingers. All fingers with a zone 2a tendon injury requiring with release of the A4 pulley had a complete release of the pulley. We analysed 22 fingers with zone 2a injuries in 15 patients (11 men and four women). In these 22 fingers (four index, six middle, five ring, and seven little fingers) the A4 pulley was completely released. Seven fingers were repaired within 1 day without prior skin closure and 15 after 2 to 13 days, following primary skin closure.
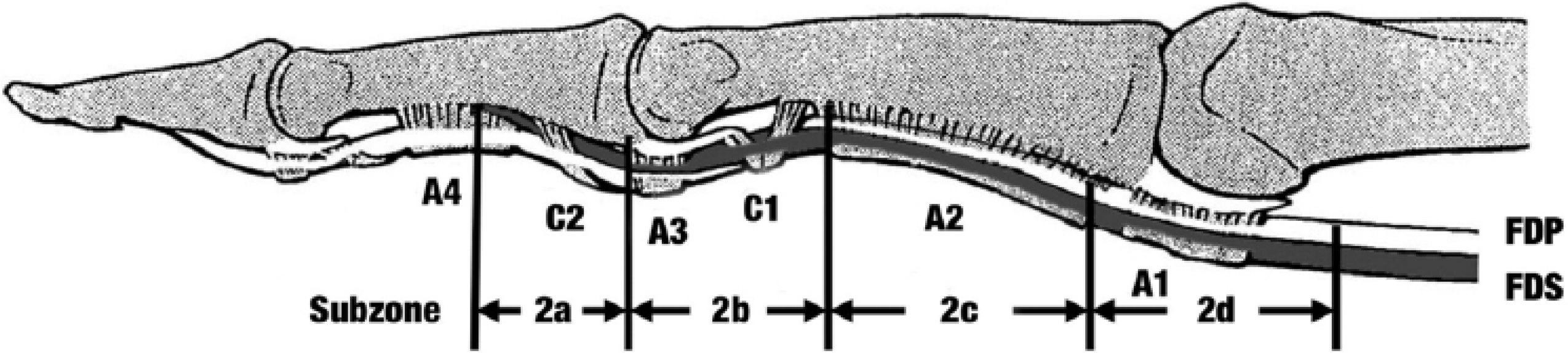
Tang’s subdivisions of zone 2. 2a – from the distal margin of the insertion of the FDS tendon to the proximal margin of the insertion. 2b – from the proximal margin of the insertion of the FDS to the distal margin of the A2 pulley. 2c – the area covered by the A2 pulley. 2d – from the proximal margin of the A2 pulley to the proximal reflection of the synovial sheath.
Surgical methods
The laceration in the digital fibrous flexor sheath, either distal or proximal to the A4 pulley, was opened over a distance of about 2 to 3 cm through a lateral incision of the sheath. The FDP tendon was repaired using a six-strand suture described in the Yoshizu #1 technique (Moriya et al., 2015; Yoshizu, 1996), accompanied by a simple running peripheral epitenous suture using 6-0 monofilament nylon (Figure 2). All of the opened part of the sheath was not usually repaired.
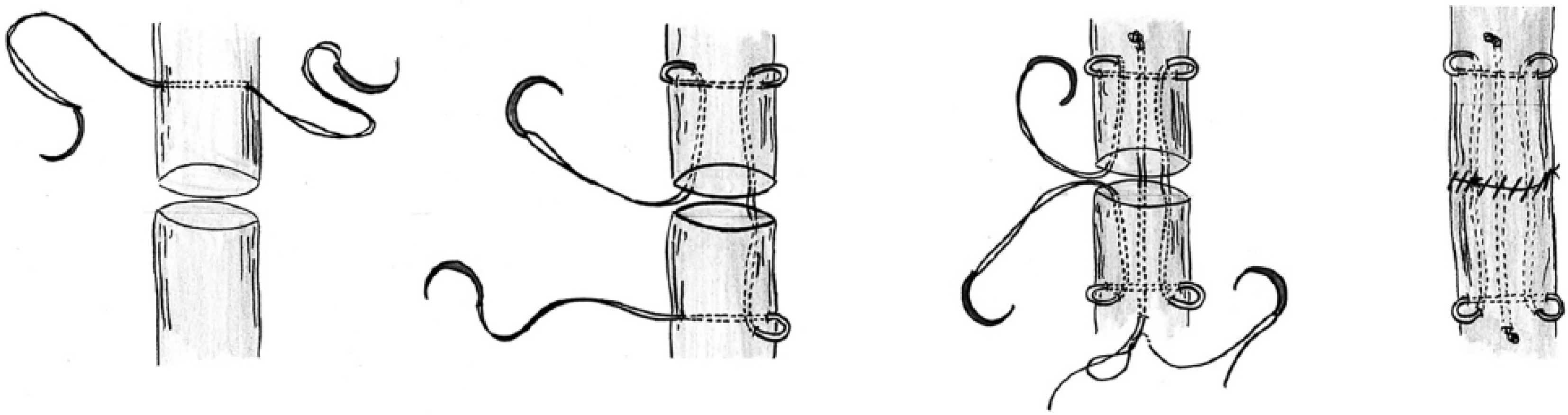
The Yoshizu #1 technique uses a combination of the Tsuge suture with a 4-0 looped thread and the modified Kessler suture using a 4-0 double strand with two needles and a running 6-0 monofilament epitendinous suture.
Our indications for surgical release of the A4 pulley are: (1) the ends of the lacerated FDP tendon were found to be difficult to pass under the A4 pulley; (2) the A4 pulley had to be opened to achieve surgical tendon repair (when the FDP tendon laceration site was very close to or under the A4 pulley); or (3) the repaired site was caught on the proximal edge of the A4 pulley when the finger was in the extended position. In addition, the C2 and A3 pulleys were incised if necessary, to allow the repaired tendons to move freely without impingement when the C1 and A2 pulleys were intact. Digital nerves were repaired as required with either 9-0 or 8-0 nylon sutures. The anastomoses of unilateral digital artery injuries were also performed using 10-0 nylon. According to Tang’s levels of surgical expertise (Tang, 2009, 2013), the tendons in 18 fingers (80%) out of 22 fingers were repaired by five consultants (one expert, four highly experienced specialists); while eight less-experienced specialists performed tendon repairs in four fingers. All patients were managed postoperatively in our hand therapy unit according to the controlled active mobilization regime previously described (Moriya et al., 2015).
Follow-up and evaluation
The mean follow-up period for all patients was 9 months (range 5–12). Active digital motion was measured with a goniometer at the final follow-up evaluation by five surgeons and three therapists.
Clinical results were evaluated using total active motion (TAM) of the fingers, Strickland and Glogovac’s criteria (Strickland and Glogovac, 1980), Tang’s criteria (Tang, 2013), and Moiemen and Elliot’s system (Moiemen and Elliot, 2000). TAM is the sum of the maximal active motion ranges at the metacarpophalangeal and/or the two interphalangeal joints in the fist position, minus the total extension deficit at these joints. Tang’s criteria has a more stringent excellent category than in Strickland’s criteria and separately grades the fingers fail to reach 30% return to active range of motion of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints as failure. Results are classified as excellent (90%–100% of the TAM of the normal PIP and DIP joints), good (70%−89% of the normal), fair (50%–69% of the normal), poor (30%–49% of the normal), or failure (< 30% of the normal). Moiemen and Elliot’s (2000) system assesses only the range of motion of the DIP joint and uses the following grades: excellent, 62°–74°; good, 51°–61°; fair, 37°–50°; and poor, 0°–36°.
Results
We treated 15 patients with a mean age of 34 years (range 20–50). Nine hands had clean injuries (cut by a clean sharp instrument) and six had more complex injuries (multiple fingers injured or a blunt/crush cut by machinery or saws, or concomitant with bilateral digital nerve injuries). The FDS tendon was repaired in six fingers, untreated in five, and excised locally in five. A total of 12 fingers had complete release of two pulleys – C2 and the A4 and nine fingers had a complete release of three pulleys, i.e. A3, C2, and A4. In the remaining one finger, the C1, A3, C2, and A4 pulleys were released, but only the C1 pulley was reconstructed using the resected FDS tendon (Figure 3).
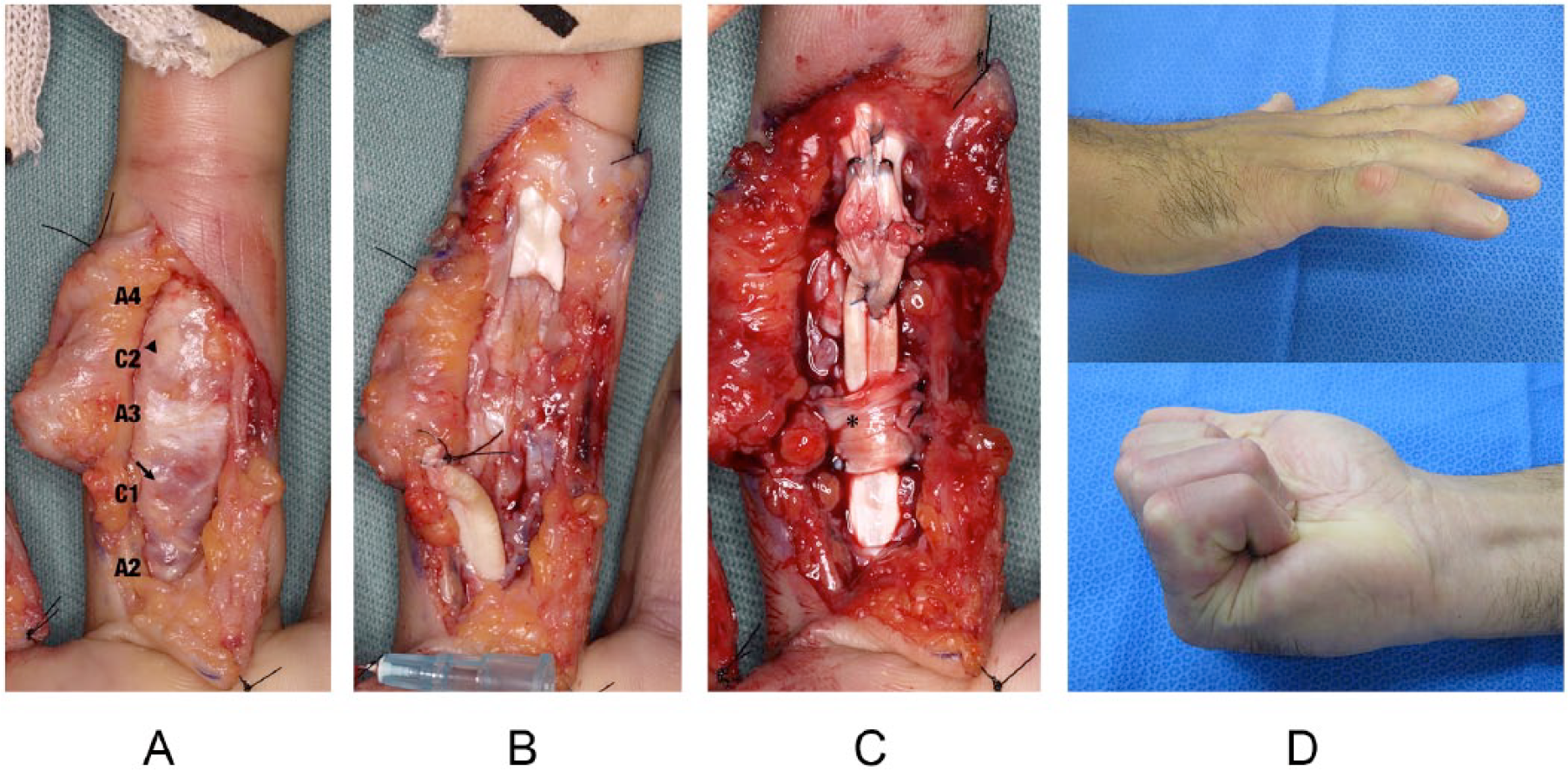
A case of delayed primary repair of the FDP tendon injury of the ring finger. (A) The laceration occurred through the C1 pulley (arrow). The distal flexor tendon stump could be observed through the distal section of the C2 pulley (arrowhead). (B) The pulleys from the damaged C1 to the intact A4 were incised to provide exposure for tendon repair. (C) The C1 pulley was reconstructed with the resected FDS tendon after the repair of the FDP tendon using the Yoshizu #1 technique (asterisk). (D) Postoperative extension and flexion 12 months after surgery.
TAM of the fingers
The average TAM of the metacarpophalangeal, PIP and DIP joints was 234° (range 143°–278°) and that of the PIP and DIP joints was 149° (range 57°–183°). The range of motion of the DIP joint averaged 60° (range 26°–80°) at the final evaluation. Table 1 summarizes the results of TAM according to the extent of the pulleys releases, excluding one finger, in which the C1 pulley was reconstructed.
Average TAM and functional results (degrees) after release of different sets of pulleys.

The one finger with C1 pulley reconstruction was excluded from the table. Numbers shown in the parenthesis are ranges.
DIP: distal interphalangeal; MP: metacarpophalangeal; PIP: proximal interphalangeal; TAM: total active motion.
Functional grading of the fingers
Patients had an excellent functional outcome in 14 fingers, good in six fingers, fair in one finger, and poor in one finger, according to Strickland’s criteria. When assessed by Tang’s criteria, nine fingers were excellent, 11 good, one fair, and one poor. No finger was rated as failure by Tang’s criteria. Using Moiemen and Elliot’s system, 11 fingers were rated as excellent, four as good, six as fair, and one as poor. Using Strickland’s criteria or Tang’s criteria, 91% of the fingers were rated good or excellent; using Moiemen and Elliot’s method only 68% were rated as good or excellent.
Outcomes after different lengths of release and in different fingers
Table 2 shows the number of digits rated excellent or good compared with the lengths of pulley release. We found the longer release of C pulleys together with the A4 pulley had similar excellent and good rate as release of only the A4 pulley. Table 3 shows the digital function results in different fingers. We found that the rate of excellent and good results is the lowest in the little finger.
Functional outcomes.
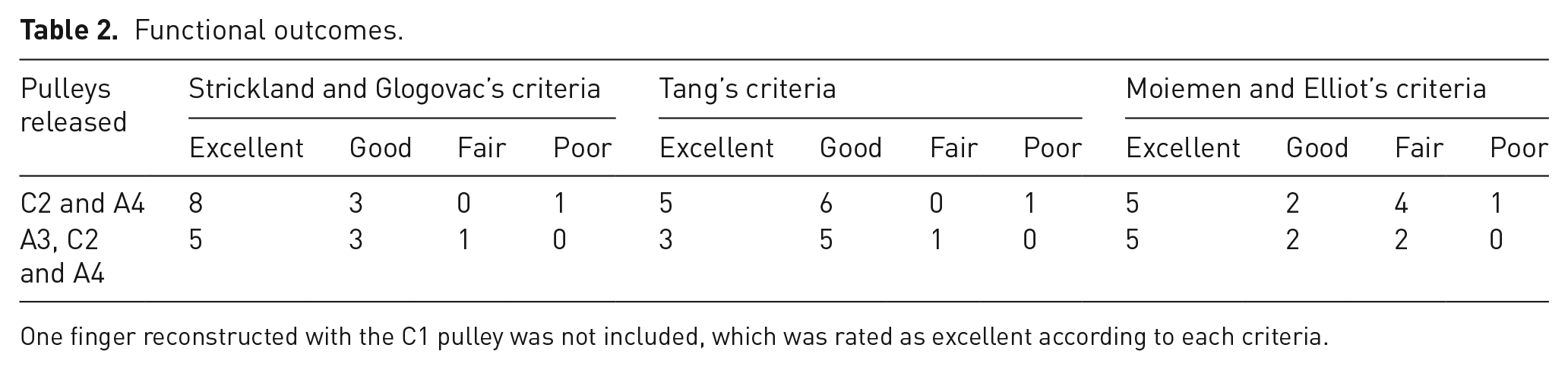
One finger reconstructed with the C1 pulley was not included, which was rated as excellent according to each criteria.
Numbers of index, middle, ring, and little fingers with excellent or good function recovery.
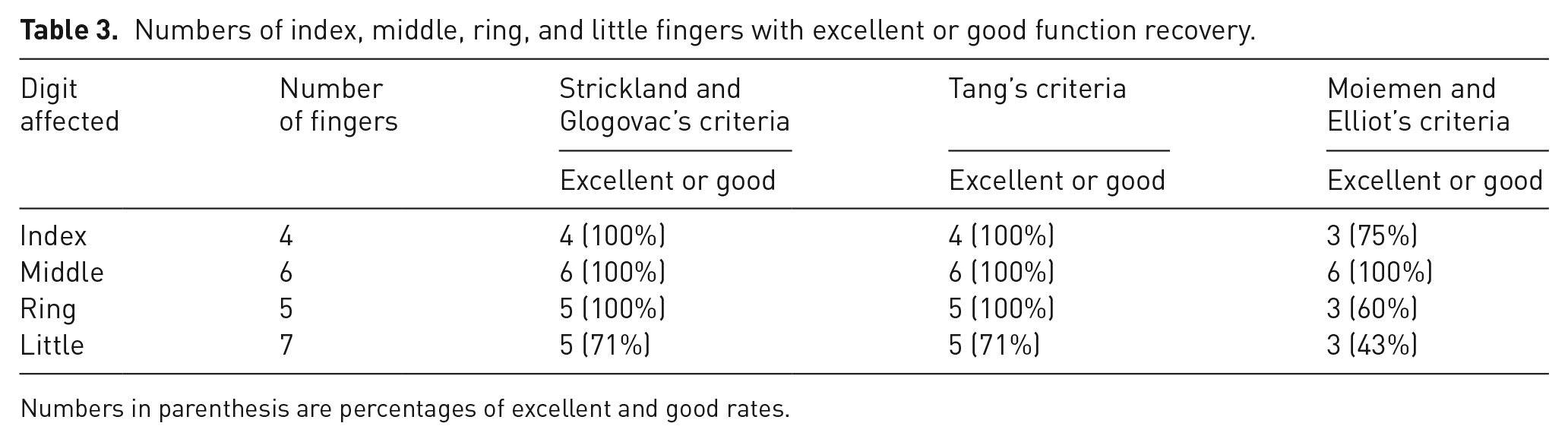
Numbers in parenthesis are percentages of excellent and good rates.
Complications and revision operations
No tendon ruptures or bowstringing occurred in any of the patients, nor were any wound complications or infections present (Figure 4). Tenolysis was performed in one little finger where the entire C2 and the A4 pulleys were released, and in another little finger where we released the A3, C2, and A4 pulleys.

A 30-years-old female who sustained zone 2a flexor tendon injuries in the middle, ring, and little fingers of the left hand. The middle and ring fingers had complete release of the C2 and A4 pulleys, and the little finger had a complete release of the A3, C2, and A4 pulleys. Follow-up at 12 months after surgery, bowstringing in each finger did not occur.
Discussion
The flexor tendon system in zone 2 has complicated anatomy, which differs at each tendon segment. The most effective method for enhancing the clinical outcome of flexor tendon repairs in zone 2 is to utilize different treatments for the tendons, sheaths, pulleys, and subcutaneous tissue to suit each region (Tang and Shi, 1992). Pulley release is considered to be as important as the use of a stronger repair for increasing the margin of safety for early active mobilization following a multi-strand tendon repair, such as the Yoshizu #1 technique we employed in our patients (Elliot and Giesen, 2013; Tang, 2007). In Tang’s zone 2a or 2b, in particular, a partial or complete release of the A4 pulley is required (Kwai Ben and Elliot, 1998; Tang, 2014b). Kwai Ben and Elliot (1998) reported that the entire A4 pulley had to be divided in 11% of zone 2a and 2b flexor tendon injuries. In our study, the percentage of zone 2 flexor tendon repairs in which release of the entire A4 pulley was necessary is 13%, very similar to that reported by Kwai Ben and Elliot (1998). In 27% of fingers, the FDS tendon insertion point lies proximal to the A4 pulley (Kwai Ben and Elliot, 1998). When this occurs, tendon repairs in zone 2a may not need the A4 pulley release.
The A4 pulley has traditionally been preserved or surgically closed when it is divided for the repair of the flexor tendon, to prevent the suture site on the tendon from impinging on the edge of the annular pulley and to prevent tendon bowstringing. Various studies have pointed out that a closure of the pulley might narrow its diameter and restrict the gliding of repaired and thickened flexor tendons (Franko et al., 2011; Lowrie and Lees, 2014; Mitsionis et al., 1999; Savage, 1990). The A4 pulley has been released to increase the margin of safety for early active mobilization (Elliot and Giesen, 2013; Tang, 2007; Wu and Tang, 2014). Franko et al. (2011) found slight anterior displacement of the tendon after partial and complete release of the A4 pulley in cadaveric hands. Tang and Xie (2001) reported that tendon excursion and bowstringing increased significantly in patients with an intact sheath when the C2 and A3 pulleys were incised in addition to the A4 pulley. However, Yoshizu et al. (1999) noted that the incision of the A3, C2, and A4 pulleys had an insignificant effect on digital flexion, if the C1 pulley was intact, based on their anatomical study using cadavers. The extent of sheath to be resected should be determined by estimating the physiological gliding amplitude of the FDP tendon at zone 2 (Kwai Ben and Elliot, 1998). In addition, Tang (2014a) found that the total allowable length of incision (of the synovial sheath and the pulley) should not exceed 2 cm. We believe that the extent of pulley release, which does not clinically influence tendon function during finger motion, needs further clinical investigation. However, our data support release of the entire A4 pulley together with a part of adjacent sheath (including some cruciform pulleys) as it does not measurably affect finger function.
For zone 2 flexor tendon injuries that require the complete release of the A4 pulley, Tang (2014b) released the pulley system for 1.5 to 2 cm centred on the A4 pulley without including the A3 pulley, based on his experimental study of the effect of the A3 pulley and adjacent sheath integrity on tendon function. We followed the principle, in place since at least the reports of Savage (1990) and Yoshizu et al. (1999), of keeping the C1 pulley intact when the A4 and adjunct pulleys need to be incised. Savage (1990) also stated that the maximal changes associated with incisions into even all four pulleys (the C1, A3, C2, and A4 pulleys) were small in terms of all of FDP tendon excursion, the distance from the nail to the distal palmar crease, the FDP flexion force, and tendon bowstringing. Thus, defects in up to three pulleys (such as those caused by complete incision of the A3, C2, and A4 pulleys) appear to have minimal effect on finger flexion. Our findings suggest that biomechanical changes caused by release of all of the A3, C2, and A4 pulleys may not compromise clinical outcomes. However, we cannot fully determine it because our study was limited by its retrospective nature and a small patient number.
Although release of all of the C1, A3, C2, and A4 pulleys is unlikely to be necessary clinically, if it occurred tendon bowstringing may become marked (Savage, 1990; Yoshizu et al., 1999). In primary flexor tendon repair, sheath repair or reconstruction has rarely been performed (Tang et al., 2014a). If the C1 pulley is released in conjunction with the A3, C2, and A4 pulleys, we prefer to suture or weave the tendon graft, such as the resected FDS tendon or the palmaris longus tendon, through the C1 pulley rim using non-absorbable sutures (Kleinert and Bennett, 1978). This technique is weaker than the Boyes and Bunnell method or the Riordan method (Doyle and Blythe, 1975; Widstrom et al., 1989), however, we believe that this method might be sufficient for C1 pulley restoration because the C1 pulley is mechanically less stiff than the A2 or A4 pulleys (Lin et al., 1990), and C1 pulley reconstruction is performed while the A2 pulley remains intact.
One technical point is that during surgery we used the A3 pulley as a guide for identifying the C1 and C2 pulleys. When opening the digital flexor sheath to allow surgical repair of the tendon, particularly in zone 2a or 2b, we release the thin band adjacent to the distal end of the A3 pulley as the C2 pulley, and preserve another thin pulley between the A2 and A3 pulleys, which is located over the distal part of the proximal phalanx, as the C1 pulley.
According to Strickland’s, Tang’s, or Moiemen and Elliot’s criteria, the good and excellent outcomes (71%, 71% and 43%, respectively) in the little finger were lower than for the other fingers in this study. Our results suggest that the little finger has a worse outcome in flexor tendon repair than other fingers. We could not perform statistical analysis due to the small number of little finger injuries. In our patients, the results rated with Tang’s criteria are closer to Moiemen and Elliot’s criteria, which assesses only the range of motion of the DIP joint. From these results, we believe that Tang’s criteria can more strictly identify those patients with very excellent outcomes than Strickland’s criteria.
Our study is limited by the small and heterogeneous sample sizes. We lacked sufficient statistical power to reach conclusions about the extent of pulley release for zone 2a flexor tendon injuries. It is conceivable that the outcomes may have changed if we had included more fingers in our study.
Overall it remains unclear whether release of the A3 pulley combined with the C2 and A4 pulleys influences the clinical outcomes of flexor tendon repair in zone 2a based on this study.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.