
Abstract

Dear Sir,
Closed reduction and percutaneous Kirschner wire (K-wire) fixation is a recognized method in the treatment of displaced distal radial fractures. It is a common belief that additional immobilization in a plaster splint is mandatory, as the fixation does not provide enough stability to maintain reduction until the fracture heals. However, our clinical observations of patients who removed their splints prematurely without consequences prompted us to investigate the need for prolonged immobilization after this procedure.
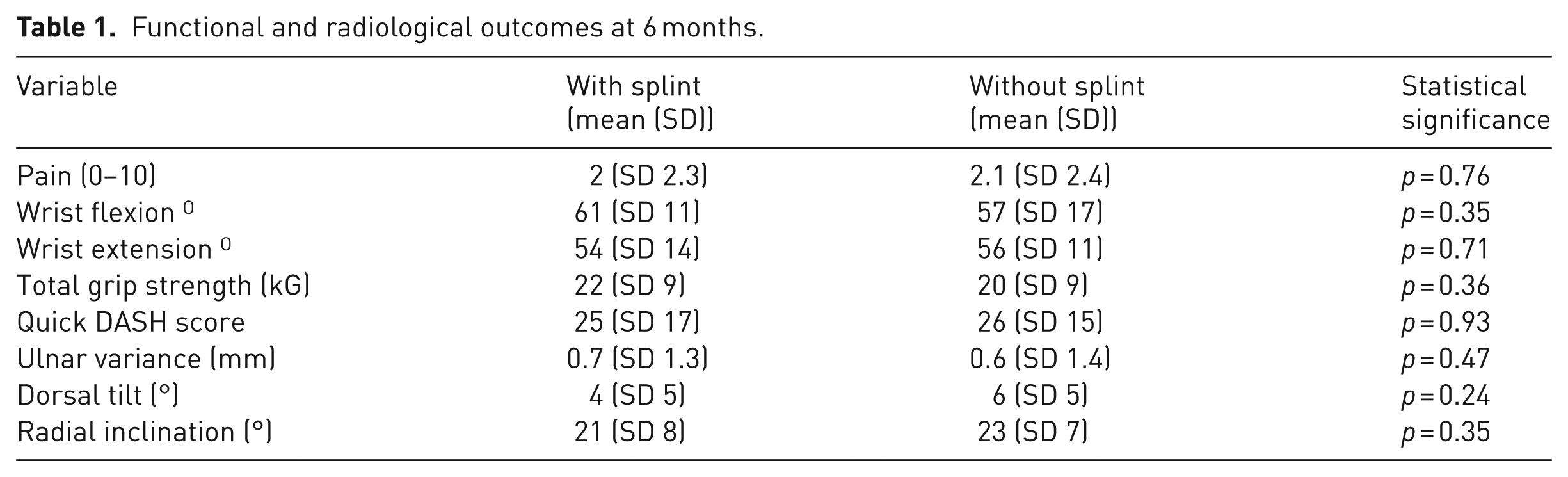
We performed a randomized study on 50 patients with distal radial fractures treated by close reduction and fixation with K-wires. The operative technique consisted of mixed transtyloid and intrafocal fixation, with 5–7 K-wires of 1.4–1.6 mm diameter (‘augmented’ fixation) (Figure 1). Patients were randomly allocated to post-operative wrist immobilization in a short splint for 4 weeks, or to splint immobilization for 1 week, followed by a soft dressing limited to the pin sites. Of the 63 patients initially recruited, 50 (79%) were available at 6-months follow-up, with 26 splinted for 4 weeks and 24 for 1 week, this group being the subject of the study. There were 41 women (82%) and nine men (18%), with a mean age of 57 years (range 25–80). The fracture configurations according to AO classification were: A3 – 11, C1 – 8, C2 – 7 in the plaster splint group, and A3 – 9, C1 – 11, C2 – 6 in the non-plaster group. There were no differences in sex, age, fracture configuration and involvement of the dominant hand between the groups. All patients had a clinical and radiological review in an out-patient clinic at 2 and 6 weeks post-operatively, when the K-wires were removed. The final clinical and radiological assessment was performed at 6 months, including pain in numeric scale (0–10), wrist movements, total grip strength, quick DASH scores and radiological parameters. Statistical calculations were performed by Mann–Whitney U-test. At the 6-month follow-up, no statistically significant differences were noted in any of measured functional or radiological variables between the group, with and without splinting, as shown in Table 1. No unacceptable displacement was noted. Four patients (8%), two in either group, reported transient inflammation around one of the pins, successfully treated with oral antibiotics.
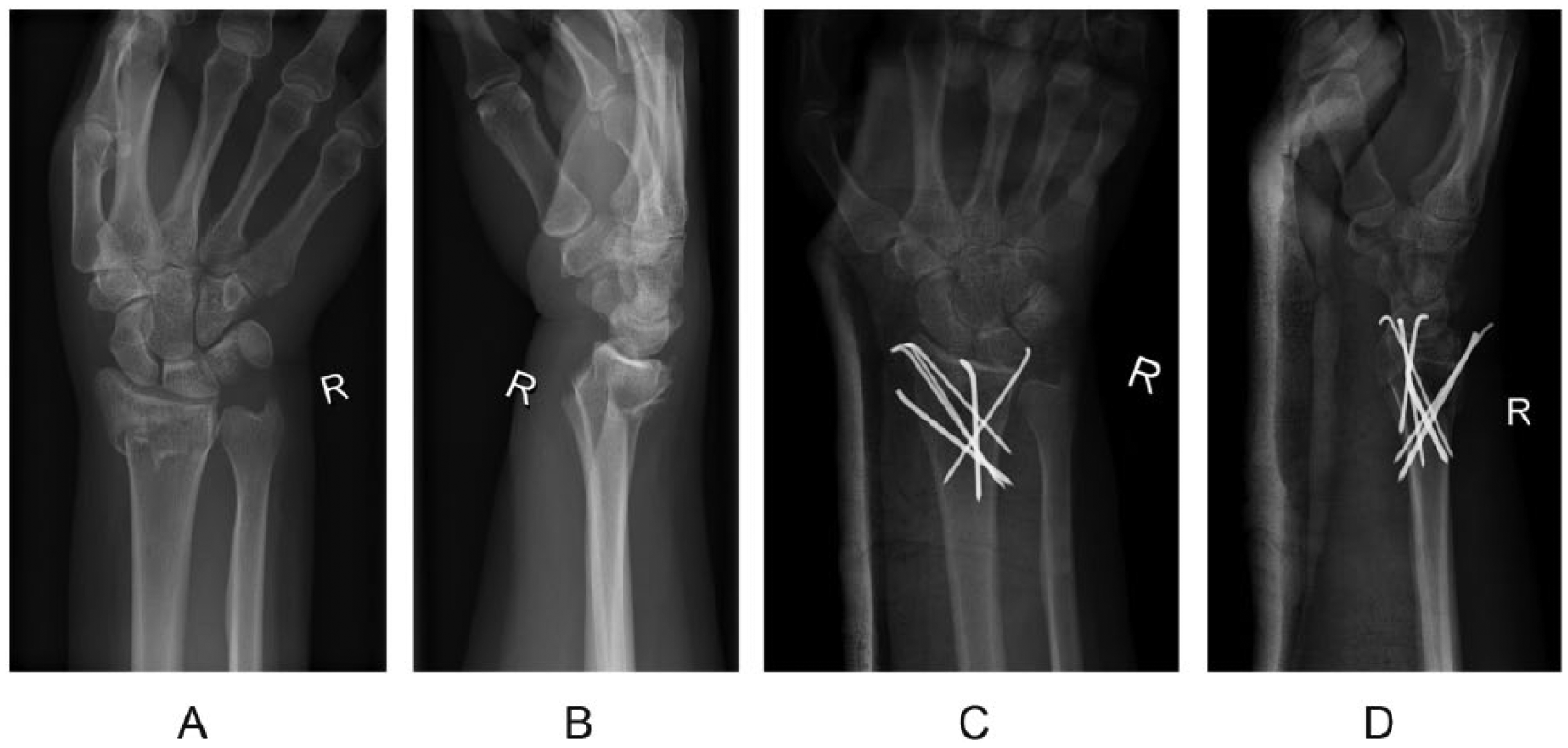
Illustration of an ‘augmented’ technique of K-wire fixation of type AO A3 distal radial fracture.
Functional and radiological outcomes at 6 months.
Almost all studies on K-wire fixation of distal radial fractures suggest plaster immobilization to be necessary in post-operative care (Barton et al., 2005; Hull et al., 2011). There was one study by Allain et al. (1999) showing outcomes similar to ours at 1-year follow-up after treatment of 60 patients without immobilization. The results of this study show that ‘augmented’ K-wire fixation of displaced distal radial fractures is sufficiently stable in the majority of cases to allow treatment of patients without additional plaster splint, except for comfort during the first week after operation. However, in some circumstances (such as imperfect fixation, osteoporotic bone or poor patient compliance) additional immobilization in a plaster splint may be judged necessary.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Local Ethics Committe of Pomeranian Medical University in Szczecin, Poland.