
Abstract
Few randomized trials have shown how the placement of a palmar locking plate affects outcomes. The purpose of this study was to compare clinical and radiological outcomes of fixation using locking plates with different concepts for placement relative to the watershed line in a prospective randomized trial. Sixty-four patients with a displaced distal radius fracture were divided into two groups according to the plates used for fixation: distal-type (AcuLocTM, Group A) and proximal-type (VariAxTM, Group V). Wrist function including the range of motion and grip strength was compared at 1, 2, 3 and 6 months postoperatively. Loss of reduction was assessed radiologically. Both groups demonstrated overall satisfactory function at 6 months with no significant difference found between the groups. Minimal loss of reduction was demonstrated in both groups. Internal fixation using the palmar locking plates with two different placements provided satisfactory outcomes at 6-month follow-up, but our results indicate that plates placed distal to the watershed line may delay recovery of wrist motion.
Introduction
Recent studies have demonstrated that surgical fixation with a palmar locking plate results in satisfactory outcomes for displaced fractures of the distal radius (Chung et al., 2006; Goehre et al., 2014; Jupiter et al., 2009; Koshimune et al., 2005; Walenkamp et al., 2015). Despite promising outcomes, some clinical reports have indicated that the distal part of the palmar locking plate could project close to the flexor tendons, potentially causing subsequent damage in the tendon (Adham et al., 2009; Arora et al., 2007; Bentohami et al., 2014; Soong et al., 2011). Based on the relevant anatomy, Orbay defined the watershed line, which is the prominent line on the palmar surface of the distal radius (Orbay, 2005). He suggested that placement of the plate distal to this line should be avoided to prevent damage to the flexor tendons. Accordingly, some commercially available plates have been developed on the basis of his concept.
To date, few studies have investigated the differences in clinical and radiologic outcomes between fixation using palmar locking plates placed proximal or distal to the watershed line. In particular, there are no randomized trials that have assessed the outcomes of different plate placement. Therefore, the purpose of this study was to compare post-operative outcomes in patients who underwent surgical treatment with palmar locking plates, placed proximal or distal to the watershed line for fixation of distal radius fracture.
Methods
This study was a single-centre, parallel group, participant-blinded, randomized controlled standard-of-care trial. The trial was given ethical approval by our institute (No. H23-4). (Consort Checklist, supplementary material)
All patients aged over 20 years with a displaced distal radius fracture, of type 23-A.2, A.3, B or C according to the AO classification (Marsh et al., 2007), were eligible for this study. Patients were recruited between September 2011 and October 2012. We used the indications for internal fixation proposed by Kapoor et al. (2000); angle of radial inclination (RI) <15°; dorsal tilt (DT) or palmar tilt (PT) >15°; ulnar variance (UV) >3 mm using preoperative plain radiographs; or articular step-off >2 mm using preoperative plain computed tomography. Exclusion criteria included the existence of an open fracture and associated fractures of the distal ulna with the exception of styloid tip fractures. Patients with previous dis-orders in their upper extremities, brain or cervical spine, based on their self-reported medical histories, were also excluded. All the patients signed informed consent to participate in the study as well as for the evaluation and publication of their results.
A total of 216 patients were diagnosed with a distal radius fracture during the period. Of these, 144 patients were excluded, including six patients (2.8%) who declined participation in the study. Seventy-two patients were enrolled in this study, and randomly assigned into two groups (36 patients in Group A and 36 patients in Group V). Four patients in each group were lost to follow-up; therefore, 64 patients (32 patients for each group) were included in this study (Figure 1). The baseline demographic data are shown in Tables 1 and 2. There were no significant differences between groups regarding their age, sex, hand dominance and the duration from the injury to surgery. In addition, there was no significant difference between the groups for either fracture type according to the AO classification, nor the number of cases with a fragment located distal to the watershed line. We compared outcomes between two types of distal radius locking plates with different placements; the AcuLocTM distal radius plate system (Acumed, Hillsboro, OR, USA; Group A, n = 32; Figure 2), which is placed distal to the watershed line, and the VariAxTM distal radius locking plate system (Stryker, Fraiburg, Germany; Group V, n = 32; Figure 3), which is designed for placement proximal to and without overlying the watershed line. Patients were allocated to one of the two groups, based on a randomized permuted blocks design (Matts and Lachin, 1988) performed by one of the investigators (H. T.).
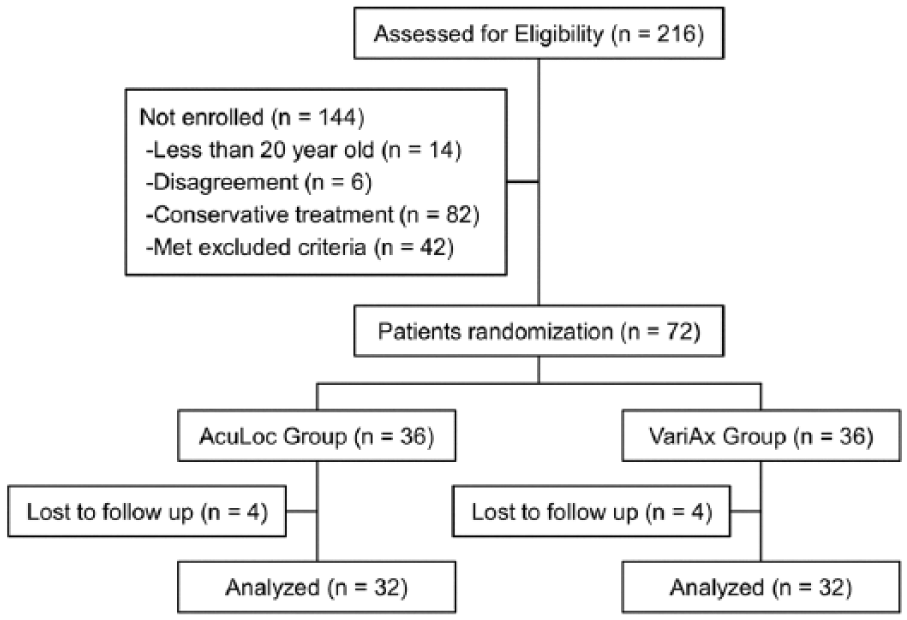
Study flow sheet.
Patient characteristics.
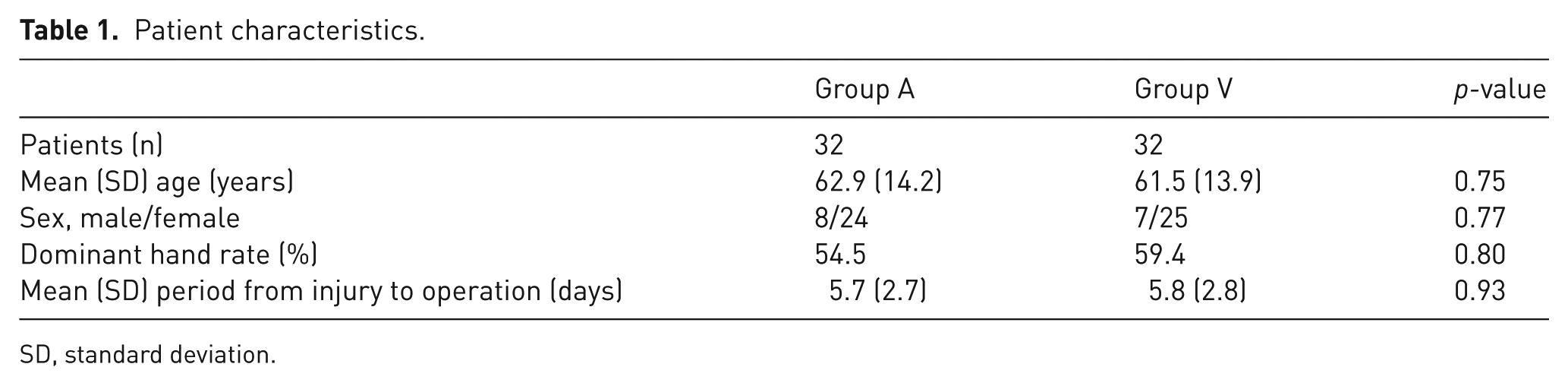
SD, standard deviation.
Fracture type.
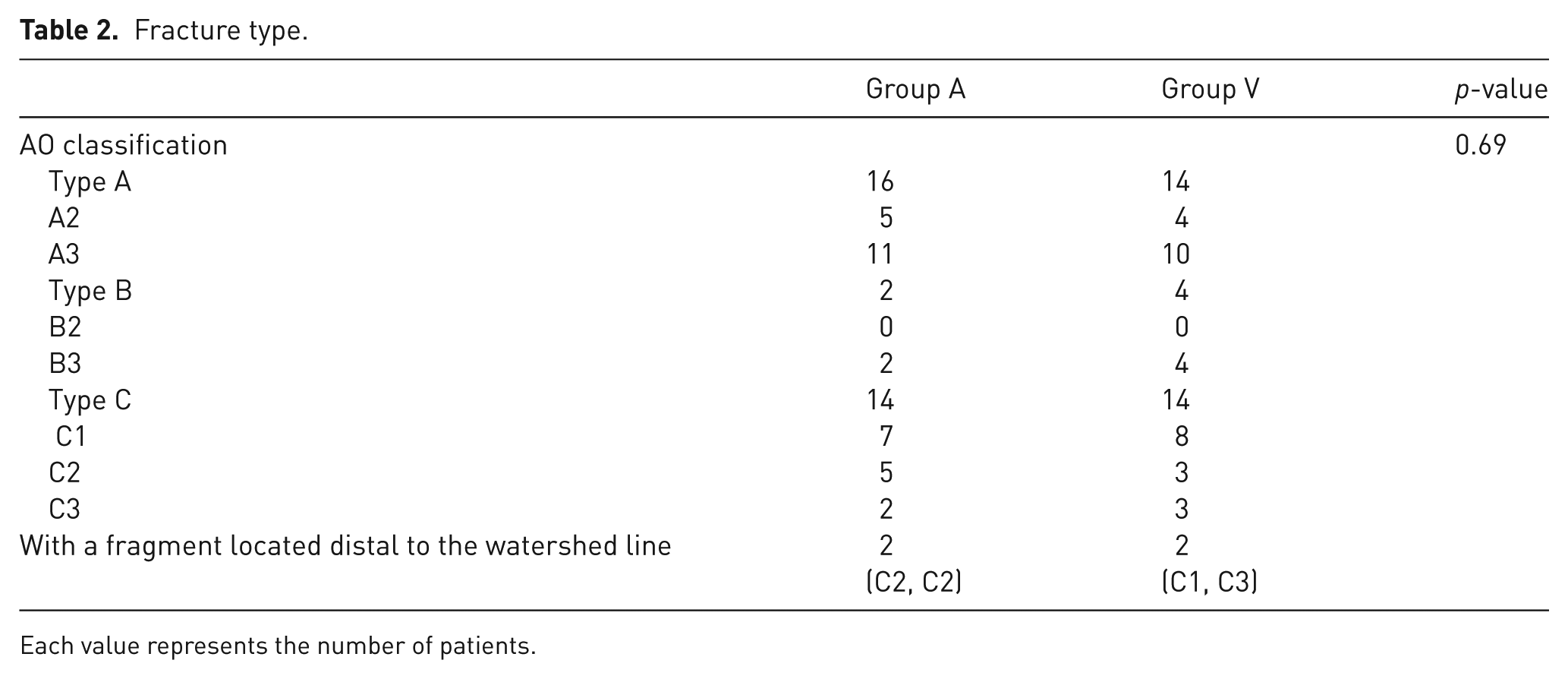
Each value represents the number of patients.

Radiographs for the AcuLoc distal radius plate system (Group A). Preoperative anteroposterior (A) and lateral (B) view; postoperative anteroposterior (C) and lateral (D) view.

Radiographs for the the VariAxTM distal radius locking plate system (Group V). Preoperative anteroposterior (A) and lateral (B) view; postoperative anteroposterior (C) and lateral (D) view.
All patients in both groups underwent surgical treatment according to a standardized procedure: the trans-flexor carpi radialis (FCR) approach; temporary fixation of the fragments or reduction with K-wires; and internal fixation with either plate (AcuLoc or VariAx). Distal locking screws were inserted into the subchondral area with the aid of fluoroscopy. All patients were operated on by the same surgical team, made up of four surgeons including a senior trauma surgeon. The rehabilitation protocol was initiated at 24 h after surgery, commencing with finger movements, and gradually introducing active and passive movements of the wrist (1 week and 3 weeks after surgery, respectively). The rehabilitation staff were not involved in the study and did not know the treatment group to which each patient had been assigned.
The primary outcome measures were range of motion (ROM) in wrist flexion and extension and the grip strength at 1, 2, 3 and 6 months after surgery. These values were calculated as a percentage of their uninvolved side to account for individual differences. Clinical outcomes were measured with the Mayo Wrist score (Cooney et al., 1994) and the Disability of the Arm, Shoulder, and Hand (DASH) score (Hudak et al., 1996) at the 6-month follow-up. The incidence of complications, including tendon rupture, carpal tunnel syndrome and complex regional pain syndrome (CRPS) was also assessed in both groups. All data were recorded in the electronic database of our institute.
Secondary outcome measures were performed using radiographs and sonograms. To assess the union of the fracture, AP and lateral radiographs were examined at every visit with the following parameters for loss of reduction: RI (°); UV (mm); and PT (°). Each parameter was measured postoperatively (0 months) and at the 6-month follow-up. Loss of reduction was calculated from the difference between immediate postoperative values and those at the 6-month follow-up. In addition, we assessed the implant prominence to the palmar side using a lateral radiograph. According to a previous study (Soong et al., 2011), a line parallel to the axis of the radius was drawn on the tip of the palmar side of the radius. The degree of plate prominence was classified into three grades: grade 0 (distal part of the plate placed without extending palmar to the line); grade 1 (contact to the line without crossing it); and grade 2 (completely crossing the line).
We further assessed the proximity of the plate to the flexor pollicis longus (FPL) tendon at the 6-month follow-up using ultrasound examination (LOGIQe, GE healthcare Bio-Sciences, Pittsburgh, PA, USA). Ultrasound examination was performed with the patients at the sitting position. The ultrasound probe (15-4 MHz) was placed longitudinally on the palmar side of their wrists keeping their elbows at 90° flexion. In addition to dynamic assessment of FPL tendon movement above the plate, the distance between the plate and the FPL tendon was measured.
A power analysis was completed a priori to guide sample size for this study. Using data from a previous study (Hatta et al., 2010), which focused on the effect of implant placement on postoperative recovery for wrist ROM, the sample size for each treatment group was calculated based on a 10% difference. This indicated that 30 patients per group would be required to achieve 80% power with alpha equal to 0.05.
Statistical analyses
Statistical analyses were performed using JMP Pro 11 (SAS Institute Inc., Cary, NC, USA). Paired t-test and Fisher’s exact test were used to compare demographic data and clinical results between the Group A and Group V. The level of significance was set at p = 0.05.
Results
Functional assessments
Both groups showed satisfactory outcomes at final follow-up, and there were no significant differences in wrist flexion or extension ROM between the groups (Table 3). Group V showed significantly better ROM than Group A at 1-month follow-up (p = 0.04). There were no significant differences in grip strength between groups at any time points.
Clinical outcomes and complications.
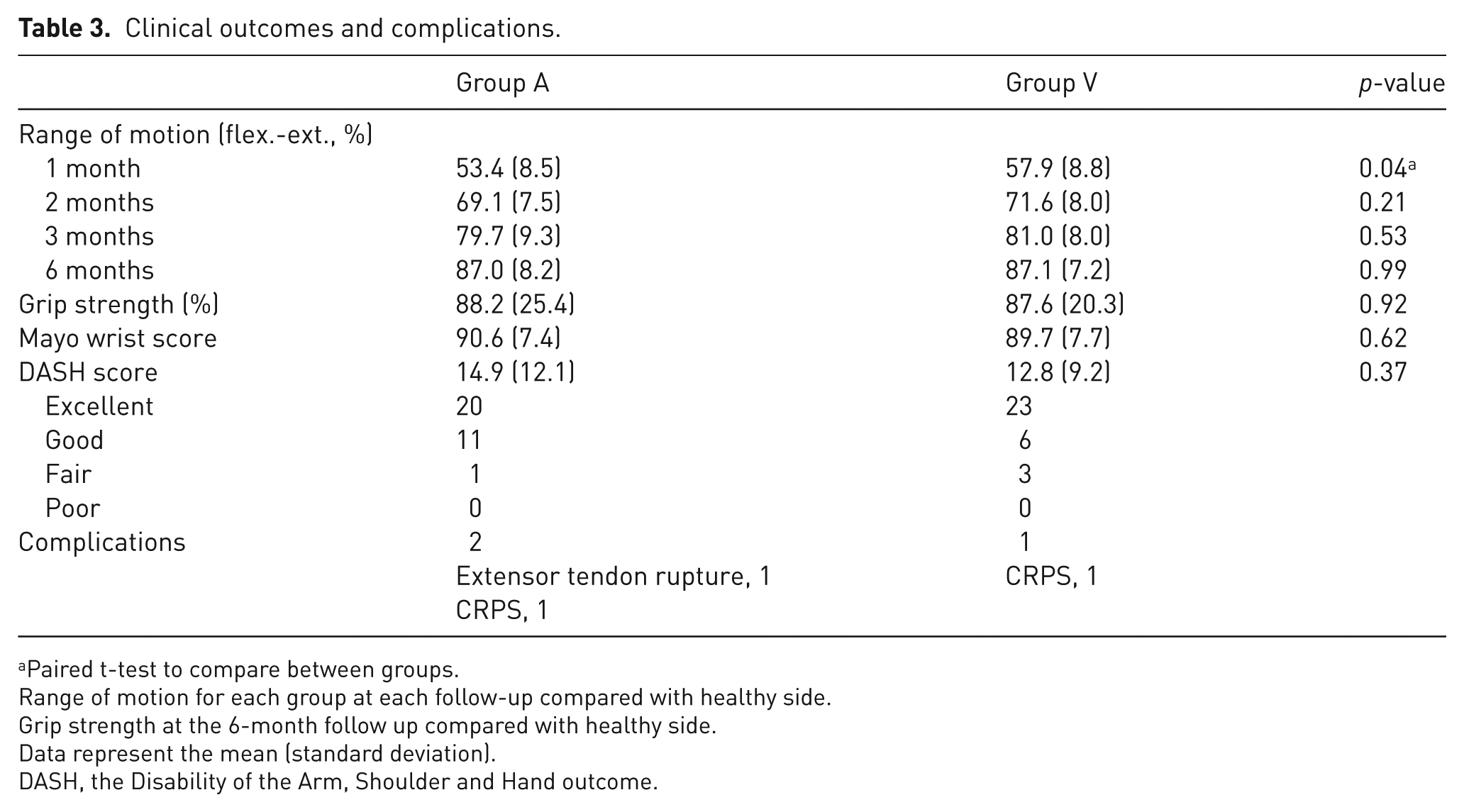
Paired t-test to compare between groups.
Range of motion for each group at each follow-up compared with healthy side.
Grip strength at the 6-month follow up compared with healthy side.
Data represent the mean (standard deviation).
DASH, the Disability of the Arm, Shoulder and Hand outcome.
The Mayo Wrist Score and the DASH score demonstrated that internal fixation using both plates provided satisfactory outcomes of wrist function at the 6-month follow-up with no significant differences between groups. The mean Mayo Wrist Score was 90.6 points in group A and 89.7 points in group V (p = 0.62), and the mean DASH score showed 14.9 points in group A and 12.8 points in group V (p = 0.37).
Complications
Overall, three patients (4.7%) developed postoperative complications as shown in Table 3. There were no patients with deep infection or flexor tendon rupture. One patient in Group A was diagnosed with a tendon rupture of the extensor pollicis longus (EPL) at 12 weeks after surgery due to insufficient reduction of a dorsal fragment. This patient did not wish to take surgical treatment until final follow-up. Two patients (one in each group) had residual pain due to CRPS.
Radiological and sonographic assessment
No significant differences in loss of reduction for RI, UV and PT were observed between groups at the final follow-up (Table 4). According to Soong’s classification (Soong et al., 2011) plates in Group A were placed with a palmar prominence more frequently than those in Group V (p = 0.002). Sonographic analysis revealed a greater distance between the plate and the FPL tendon in Group V (mean, 1.0 mm) than that in Group A (mean, 0.5 mm) (p = 0.003). The movements of the FPL tendon were subjectively analysed by the examiner, looking for deviation from the normal smooth, linear motion. No such abnormalities were noted in any case in either group.
Radiological and sonographic outcomes.
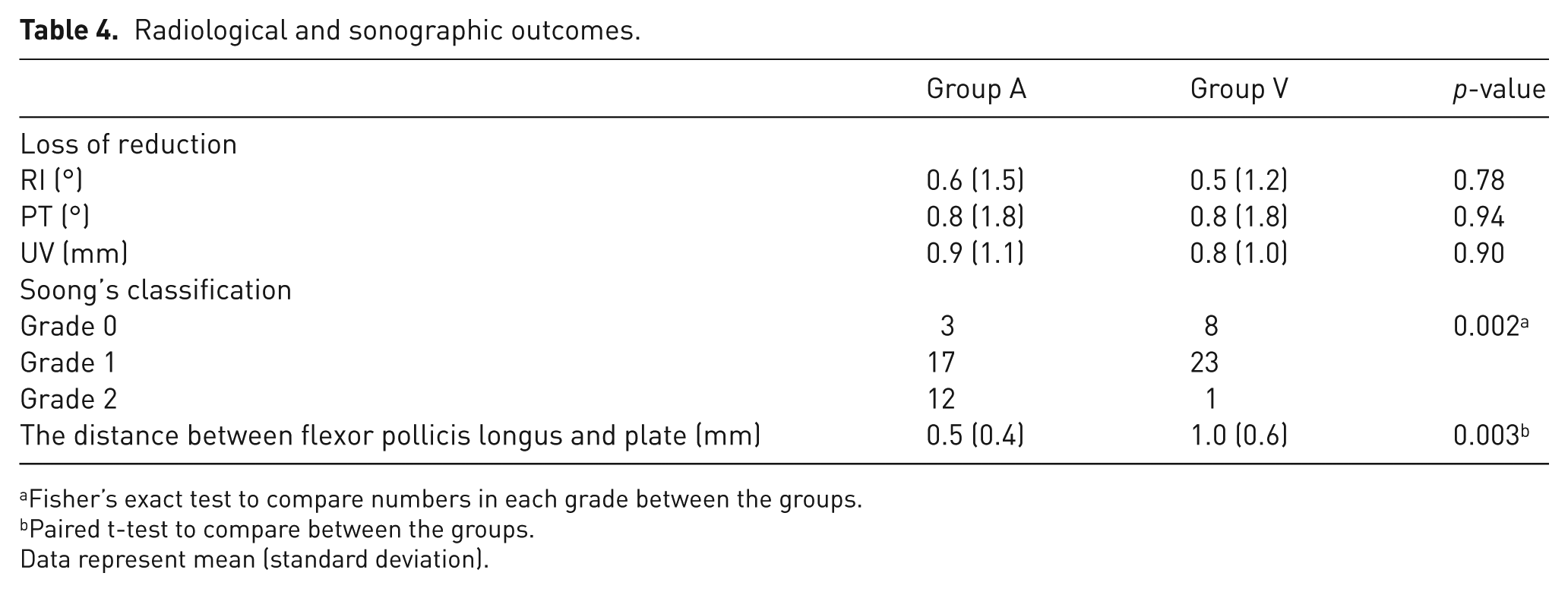
Fisher’s exact test to compare numbers in each grade between the groups.
Paired t-test to compare between the groups.
Data represent mean (standard deviation).
Discussion
This prospective study demonstrated that internal fixation using palmar plates placed proximal or distal to the watershed line provided overall satisfactory outcomes at the 6-month follow-up. To the best of our knowledge, there have been few studies comparing postoperative outcomes using different types of locking plates. Cho et al. (2014) retrospectively investigated the postoperative outcomes using different shapes of locking plates. They found no differences between the plates for either radiological or clinical outcomes after a minimum of 1-year follow-up. A recent study also compared clinical outcomes of comminuted fractures fixed with different types of locking plates, and found that the plate shapes did not affect outcomes after 2-year follow-up (von Recum et al., 2012). Similar to these studies, our study revealed minimal differences in outcomes with use of two different locking plates, VariAx and AcuLoc.
It has been reported that complications, including tendinitis, tendon rupture, carpal tunnel syndrome and CRPS, may occur after fixation with locking plates (Arora et al., 2007; Rozental and Blazar, 2006; von Recum et al., 2012). Overall reported complication rates are in the range of 3.0–27% following fixation with a palmar plate (Arora et al., 2007; Kamano et al., 2005; von Recum et al., 2012; Zenke et al., 2011). Complications were noted in three patients (4.7%) in our study, which is comparable with these previous reports. Specifically, flexor tendinitis or tendon rupture may depend on the shape and placement of selected locking plates (Orbay, 2005). Cho et al. (2014) reported flexor tendinitis after locking plate fixation with a prevalence of 3.8% for the AcuLoc plate and 0% for the Locking Compression Plate (LCP) Distal Radius System (LDRS; Synthes, Paoli, PA, USA). Soong et al. (2011) also found a similar prevalence of flexor tendon rupture (approximately 4%) with the AcuLoc plate compared with other plates. In our study, there were no cases of flexor tendinitis or flexor tendon rupture in groups that had undergone fixation with either the AcuLoc or VariAx plates. We consider that our results indicate that both plate designs can be used with minimal risk of excessive contact or irritation to the flexor tendons overlying the plates, when these are placed appropriately. In contrast, we found one case of EPL tendon rupture in the AcuLoc group; this was unrelated to plate design.
For the treatment of distal radius fractures, residual shortening of the radius and poor alignment are known to result in limited motion, deformity or arthrosis (Aro and Koivunen, 1991; Fernandez, 1993; McQueen and Caspers, 1988). To obtain essential anatomical reduction and rigid internal fixation, both plates used in this study have been designed with biomechanical evidence of rigid fixation against compression stresses (Kamei et al., 2010; Martineau et al., 2014). All cases in our series progressed to solid union after surgery, and radiological values (RI, UV and PT) presented satisfactory outcomes. These features are consistent with previous radiological analyses (Cho et al., 2014; Minegishi et al., 2011).
We hypothesized that distal placement of the locking plate might cause delayed recovery, or long-term limitation of wrist function (Hatta et al., 2010). Our results at 6-month follow-up demonstrated that wrist flexion and extension ROM recovered to approximately 88% of the unaffected side, and both groups showed similar results. At 1 month after surgery, in contrast, ROM in Group A was inferior to that in Group V; the difference was 4.5% (mean, 53.4% in Group A and 57.9% in Group V) and this was statistically significant. This finding may indicate that plating distal to the watershed line could lead to imperceptibly delayed recovery of wrist ROM. However, by the 6-month follow-up, both groups achieved similar outcomes.
A limitation of our study was a short follow-up period of 6 months. We believe this follow-up duration is appropriate to focus on the main outcome: postoperative recovery of wrist function. Further studies with a longer follow-up period will be required to compare the postoperative complications between the plates, focusing on mid- to long-term assessment of flexor tendon function.
Conclusion
In conclusion, internal fixation using palmar locking plates with different placements in relationship to the watershed line provide similar and satisfactory outcomes at 6 months after surgery. However, our results also indicate that locking plates placed distal to the watershed line may delay recovery of the wrist ROM.
Footnotes
Acknowledgements
The authors thank Dr. Yasushi Omori and Dr. Atsuko Kanno for the precious help in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The current study was given ethical approval by Iwaki Kyoritsu General Hospital (No. H23-4).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.