
Abstract
Transfer of the contralateral C7 nerve for reconstruction of the brachial plexus in infants with obstetrical brachial plexus injury has rarely been reported. We developed a new endoscopy-assisted technique via the prevertebral (retroesophageal) route for the transfer of the contralateral C7 nerve in reconstruction of the brachial plexus. The reconstruction was performed in 20 infants (14 boys and six girls). Motor recovery was assessed using the Gilbert and Raimondi scales. The Narakas Sensory Grading System was used to evaluate hand sensation. The mean follow-up period was 45 months (SD 18.2). Of the 20 children, nine had contralateral C7 transfer to lower nerve roots, two had transfer to upper nerve roots and nine had transfer to both upper and lower roots. The postoperative shoulder and elbow functions were good or satisfactory according to the Gilbert classification in all children whose preoperative scores were poor. All patients with lower roots reconstruction (9) had satisfactory hand function. A total of 15 children had a Narakas score of S3. Our technique enables safe contralateral C7 transfer to the avulsed roots in severe obstetrical brachial plexus injury infants with a satisfactory functional recovery.
Introduction
A complete obstetric brachial plexus injury (OBPI) results in devastating loss of upper extremity form and function. The primary option for reconstruction of the avulsed roots is nerve transfer(s). Several sources of sensory and motor axons, including ipsilateral nerve roots, intercostal nerves, the phrenic nerve, the spinal accessory nerve and more peripheral nerves such as the Oberlin transfer have been used for reinnervation.
Different authors set different priorities for surgical reconstruction following these injuries. Some authors prioritize regaining satisfactory shoulder and elbow motor function followed by basic sensorimotor function of the hand (Grossman, 2006; Shenaq et al., 2004); others focus on improving hand function (El-Gammal et al., 2010; Gilbert, 1995; Gilbert et al., 2006; Kawabata et al., 1987; Pondaag and Malessy, 2006). The functional recovery of the shoulder and elbow is usually better than the hand due to shorter regeneration distances and less complex muscle function. In recent years, there has been a particular emphasis on reconstruction of C8 and T1 root lesions because of their key role in good hand function, even in cases with recovery of extrinsic finger flexor function (El-Gammal et al., 2010).
Recovery of the hand is expected to continue for up to 8 years (Haerle and Gilbert, 2004); denervated target muscles that have been in a state of irreversible atrophy can be innervated by regenerated nerves (Jane et al., 2006; Lu et al. 1997). Wu et al. (2013) showed that intrinsic hand muscles undergo faster irreversible atrophy than the proximal arm muscles. They also found that the numbers of motor end plates of muscles was significantly more in reconstruction subgroups where atrophy of muscles was reversible, than in those where atrophy of muscles was irreversible. The authors stated that the muscle, rather than the nerve, limits the restoration of muscle fibres in reconstruction subgroups with irreversible muscle atrophy. In theory, the faster the reinnervation, the better the functional improvement. Gilbert et al. (2006) recommend transferring upper nerve roots to the medial cord. El-Gammal et al. (2010) recommend using the best ipsilateral root stump to reinnervate the medial cord for reconstruction of the hand and the contralateral C7 (CC7) to the axillary nerve or the posterior cord via sural nerve grafts. Terzis and Kokkalis (2008) recommend a CC7 transfer for median nerve neurotisation, because it has a large number of fibres.
Transfer of the CC7 nerve has shown promising results in adults and has become one of the treatment options for root avulsions (Chuang and Hernon, 2012; Gu et al., 1992; Songcharoen et al., 2001; Terzis and Kokkalis, 2009; Wang et al., 2013). The average number of axons within the C7 root is significantly greater than in the median, ulnar and radial nerves (Bonnel, 1984). Although in children recovery of some function has been achieved using the CC7 (Chen et al., 2007; El-Gammal et al., 2003), the effectiveness and feasibility of CC7 transfer remains controversial due to difficulties with the surgical techniques.
Several routes for CC7 transfer have been described. One aim of the CC7 transfer is to provide a route that is as short and safe as possible. McGuinnes and Kay (2002) transferred the nerve through the retropharyngeal space. Xu et al. (2008) performed the transfer through a tunnel posterior to the scalenus anterior muscle. Chuang and Hernon (2012) prefer a subcutaneous transfer to monitor the progression of Tinel sign, although the nerve route is longer than the prevertebral route. Similarly, Zhang and Gu (2011) transferred via a cross-chest subcutaneous tunnel. We have developed a new endoscopically assisted technique for CC7 nerve transfer via the prevertebral retro-oesophageal route.
The aim of this study was to assess the mid-term results of primary nerve reconstruction of OBPI with an endoscopically-assisted CC7 transfer.
Methods
Patients
We retrospectively reviewed the functional outcomes of children with severe OBPI treated surgically. The diagnosis of OBPI was based on a detailed history of the birth, a clinical evaluation and neurophysiological findings. Magnetic resonance (MR) myelography was performed in all infants under general anaesthesia using a 1.5 Tesla AeraTim MR imaging (Siemens, Erlangen, Germany). The technique we used provided a sequence with very high cerebrospinal fluid (CSF)-to-tissue contrast with the elimination of pulsation artefacts and optimal visualization of the exiting cervicothoracic nerve root (Somashekar et al., 2014). The extent of dural damage and rootlet injury were evaluated (Tse et al., 2014). The definitive assessment of the nerve injury was based on the surgical findings.
The major inclusion criteria for this study were babies with total brachial plexus dysfunction who underwent surgical exploration and endoscopically assisted CC7 nerve transfer via the prevertebral (retro-oesophageal) route between May 2008 and April 2013 (Figure 1). We operated on 20 infants (14 boys and six girls) with complete OBPI at a mean age of 7.9 months (range 3–19; SD 3.9) with a mean follow-up period of 45 months (SD 18.2) (Tables 1 and 2).
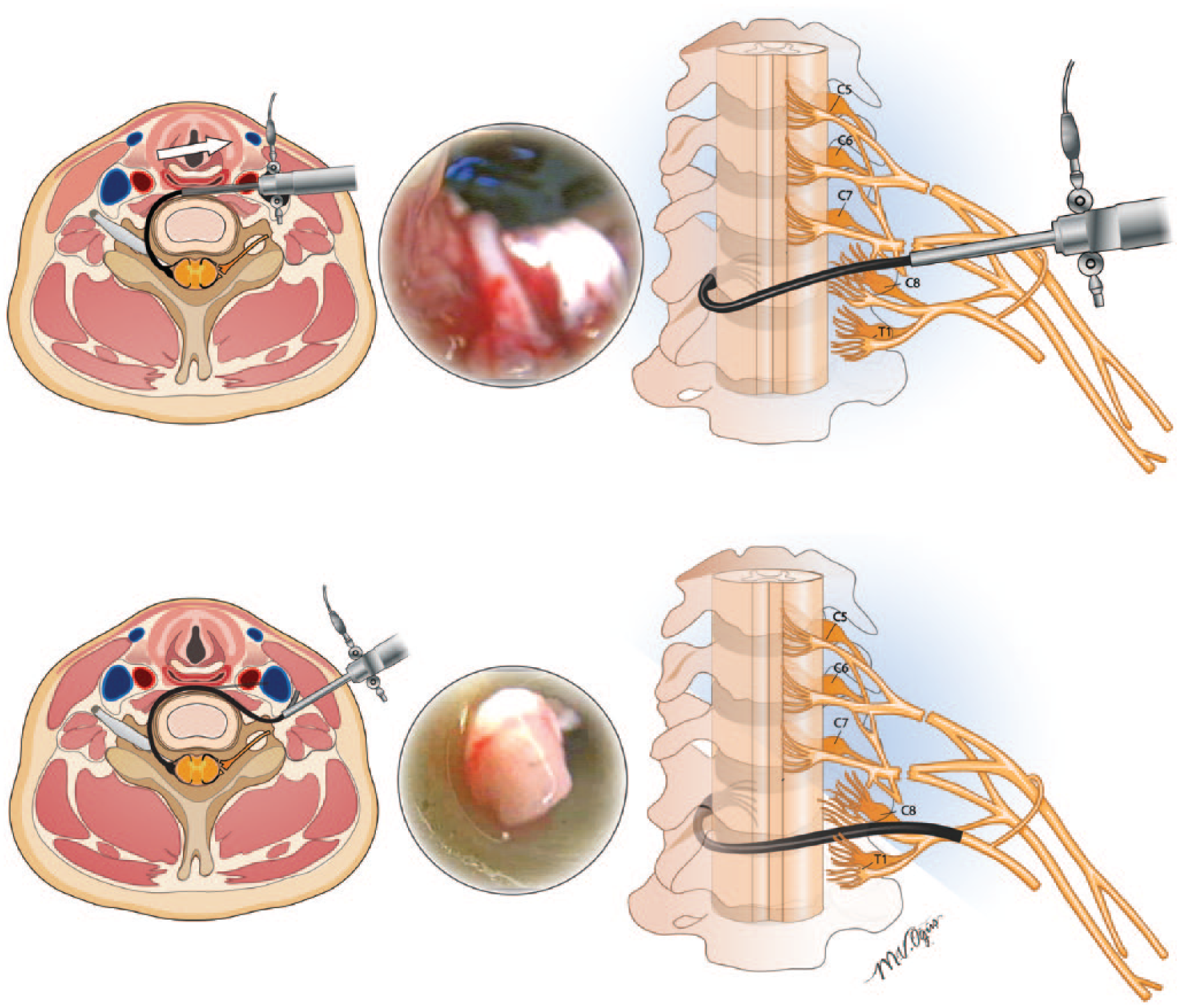
The tract of the scope is shown schematically. A scope was inserted between the prevertebral space and oesophagus from the injured side to the contralateral side and passed to the contralateral side posterior to both phrenic nerves.
The characteristics and findings of the children with CC7 transfer to lower roots.
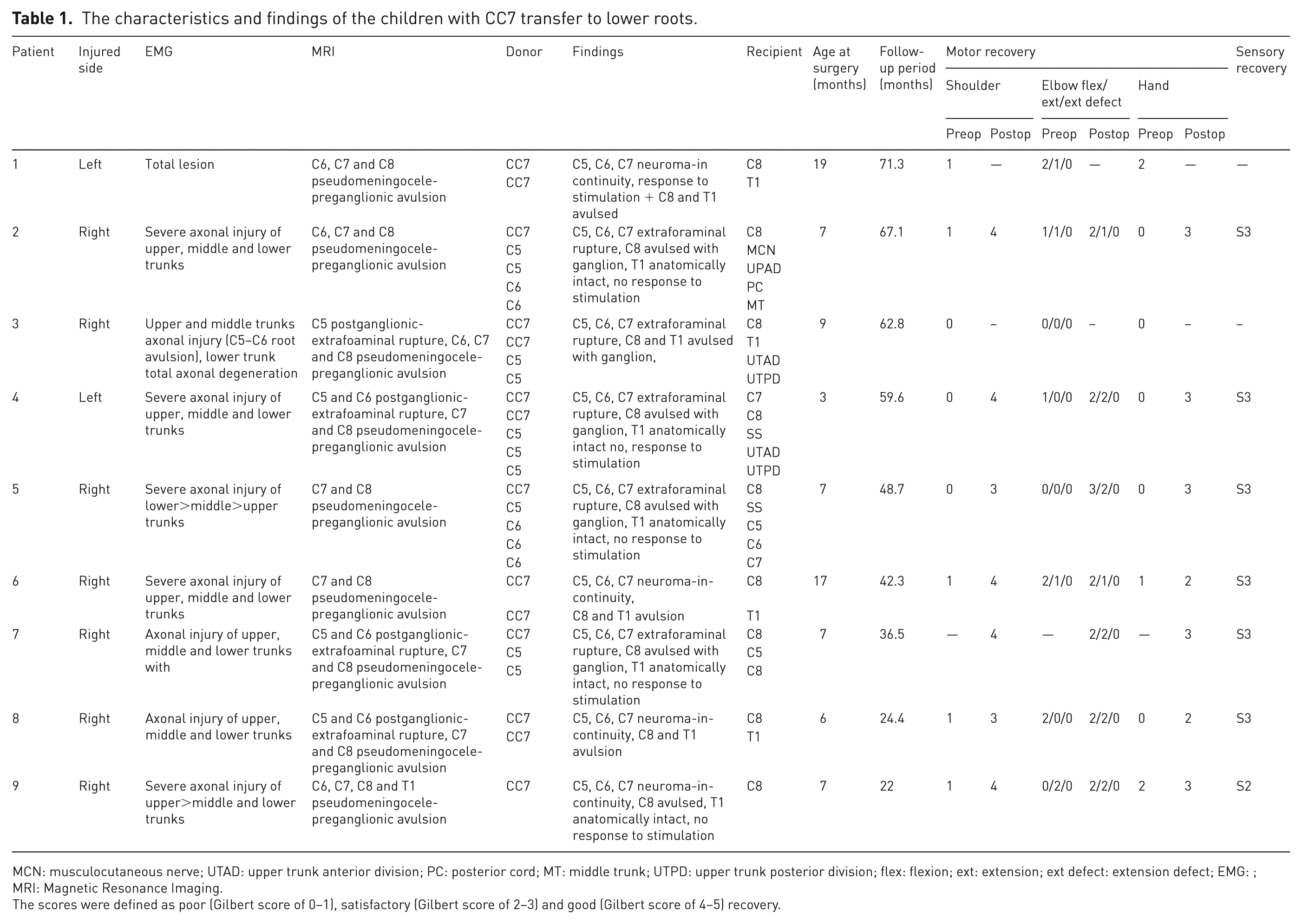
MCN: musculocutaneous nerve; UTAD: upper trunk anterior division; PC: posterior cord; MT: middle trunk; UTPD: upper trunk posterior division; flex: flexion; ext: extension; ext defect: extension defect; EMG: ; MRI: Magnetic Resonance Imaging.
The scores were defined as poor (Gilbert score of 0–1), satisfactory (Gilbert score of 2–3) and good (Gilbert score of 4–5) recovery.
The characteristics and findings of the children with CC7 transfer to upper and lower roots.
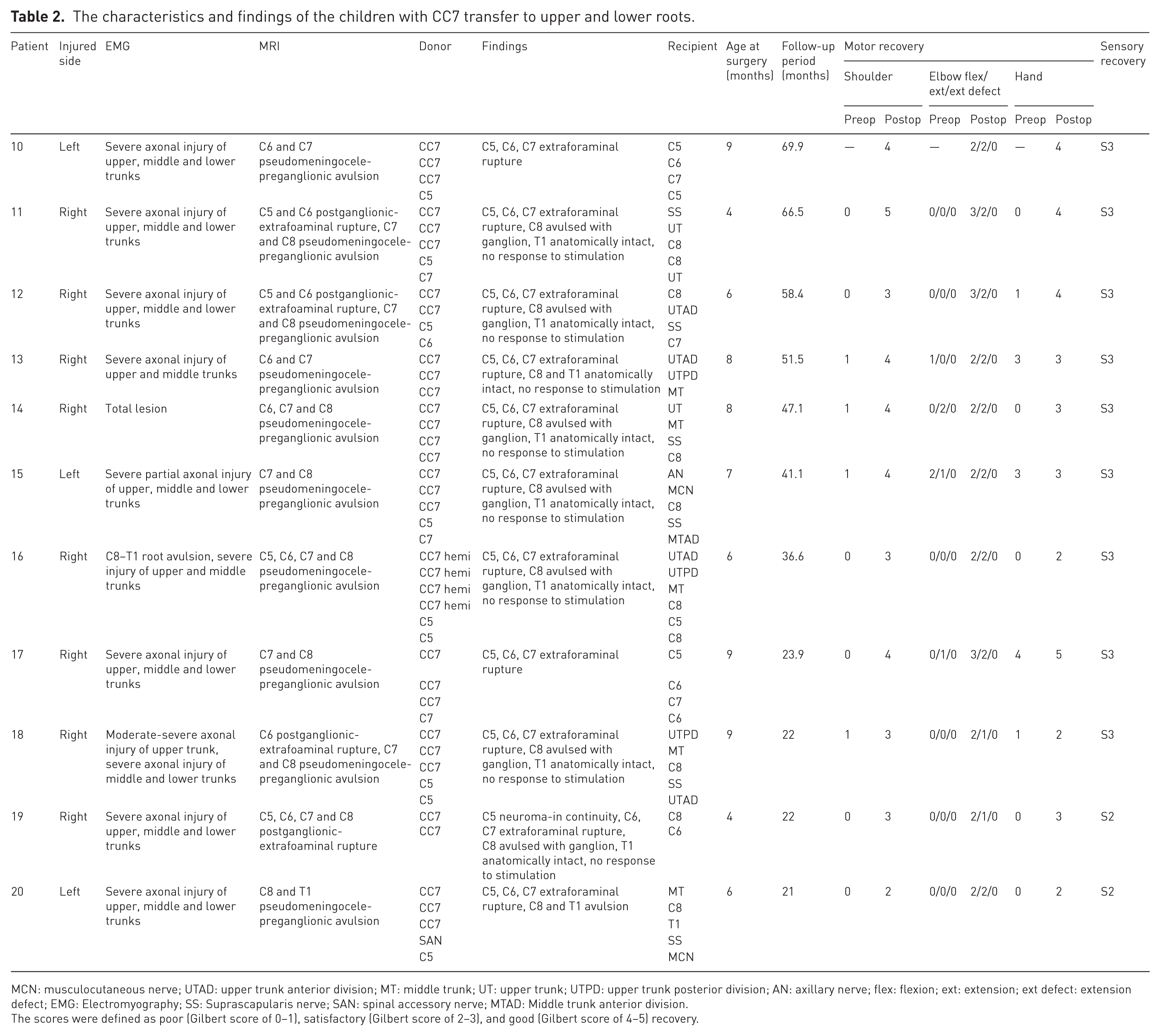
MCN: musculocutaneous nerve; UTAD: upper trunk anterior division; MT: middle trunk; UT: upper trunk; UTPD: upper trunk posterior division; AN: axillary nerve; flex: flexion; ext: extension; ext defect: extension defect; EMG: Electromyography; SS: Suprascapularis nerve; SAN: spinal accessory nerve; MTAD: Middle trunk anterior division.
The scores were defined as poor (Gilbert score of 0–1), satisfactory (Gilbert score of 2–3), and good (Gilbert score of 4–5) recovery.
The decision to use the CC7 as a donor was made during surgery based on the availability of proximal donor nerves. If there were two or fewer nerve roots available for reconstruction then the CC7 was used. Among the 20 cases, there were cases in which CC7 had been transferred to only lower roots (nine cases), to only upper roots (two cases) and to both upper and lower roots (nine cases) (Tables 1 and 2). The C5, C6 and C7 roots and extraplexal sources were used to reconstruct the upper part of the brachial plexus. The senior author (GL), level V experience (Tang, 2009), performed all the procedures.
Surgical exploration and intervention
The brachial plexus is exposed though a V-shaped incision at the injured side (Marcus and Clarke, 2003). Once the total brachial plexus injury was confirmed, the contralateral side was explored. A supraclavicular transverse incision was made just above the clavicle on the contralateral side. A similar technique was employed to expose the contralateral brachial plexus. The C5, C6 and C7 roots were identified. In 12 cases (2, 4, 5, 7, 9, 11, 12, 14, 15, 16, 18, 19), although the T1 roots were anatomically intact at operation, there were no response to electrical stimulation (Table 1 and 2). In all of these cases preganglionic injury of the C8 roots was obvious and confirmed with frozen section histology during surgery. In these cases, we preferred selective neurotization of the C8 root only with the CC7 (El-Gammal et al., 2010).
The CC7 root was dissected as distally as far as possible and divided, mostly at the level of the divisions. Autologous sural nerve grafts were prepared from both sides and were coapted to the CC7 stump with 10-0 nylon, creating two nerve loops. A 4-mm Karl Storz arthroscope (Karl Storz Inc.; Hopkins II telescope 30°, 4 mm, 18 cm, CN: 28731BWA) was inserted to the contralateral side from the injured side between the prevertebral space and oesophagus and gently passed to the contralateral side posterior to both phrenic nerves (Figure 1). The scope was withdrawn 2 mm, keeping the sheath in place. The nerve graft loops were placed and sucked into the open end of the sheath using low-pressure suction. Negative pressure was maintained to keep the nerve loops inside the sheath while the scope was being withdrawn to the injured side. The negative pressure of suction can be adjusted to a level, which is high enough to suck the nerve grafts into the sleeve of the arthroscope, but still low enough not to disrupt the neurorraphy site at the CC7. When the suture junction comes behind the oesophagus and can no longer be observed, the suction is turned off and the sleeve is withdrawn back leaving the grafts in the desired position. Intraoperative rupture of the neurorraphy junction has not been seen so far. As the phrenic nerve runs along the front of the anterior scalene muscle, there is a risk of injury to the phrenic nerve. On the contralateral side, the phrenic nerve is carefully dissected and the scalenus anterior muscle is transected at the level of the retro-oesophageal tunnel. The nerve graft lengths were trimmed and coapted to the upper and lower trunk stumps with 10-0 nylon.
The position of splintage of the upper extremity at the injured side was determined intraoperatively by checking the position of the least tension at the neural coaptation sites, especially the CC7. The stabilization of the injured upper extremity was typically with the shoulder in 90° of abduction and external rotation and the elbow in 90° flexion. After 6 weeks of immobilization, rehabilitation was initiated.
Postoperative care
The rehabilitation programme was supervised by a physiotherapist (CA) for several years depending on the children’s progress. Parents/carers also performed a daily home exercise programme. The major focus of rehabilitation before sufficient motor recovery was sensory re-education to achieve increased awareness of the affected limb and hopefully improve cortical brain representation. Nerve regeneration evaluated through neurophysiological testing guided the rehabilitation programme based of motor (Leblebicioglu et al., 2013; Ramos and Zell, 2000) and sensory re-education (Rosen and Lundborg, 2004). We mask cutaneous sensation in the donor limb via long gloves or socks while performing a variety of sensory re-education techniques for the affected limb to prevent expansion of the receptive field of the donor side over the cortical area corresponding to the newly re-innervated affected limb. Positioning the affected arm in the field of vision during daytime may increase awareness of the injured limb. Children usually benefit from aquatic therapy, which improves sensory feedback and provides a gravity-free exercise environment (Dumas and Francesconi, 2001).
Neuromuscular electrical stimulation of target muscles was initiated after regeneration was confirmed by a positive response to faradic current and was implemented as a home programme using a portable electrical stimulator. The parents/carers performed daily stimulation of target muscles for 12 minutes at a frequency of 30–70 Hz, pulse width of 1 milliseconds–300 microseconds with an output current giving a visible strong contraction (Lima et al., 2009).
In addition to neuromuscular electrical stimulation, a variety of therapeutic exercises were performed, which progressed in accordance with the overall motor development of the child. Alternate limb exercises and midline-crossing activities were used to improve bilateral coordination and mirrors were placed near the affected limb to produce mirror motor facilitation effects while movements were performed. Orthotic supports were used for the elbow and wrist joints to optimize recovery and function while awaiting recovery.
Assessment
All children were evaluated preoperatively (one day before surgery) and every 3 months postoperatively by a physiotherapist (CA) to note sensorimotor recovery and donor limb morbidity.
Assessment of motor recovery with muscle strength testing is difficult in children. We therefore used scales for shoulder, elbow and hand. Motor recovery was assessed using the Gilbert shoulder scale, the Gilbert–Raimondi elbow scale and the Raimondi hand evaluation scale (Table 3) (Haerle and Gilbert, 2004). The elbow scale, which is based on elbow flexion, elbow extension and fixed flexion contracture, is scored over five points, similar to the scoring for the shoulder and hand scales. The scores for shoulder, elbow and hand scales were defined as poor (Gilbert score of 0–1), satisfactory (Gilbert score of 2–3) or good (Gilbert score of 4–5) (Haerle and Gilbert, 2004). Previous authors have suggested that a Raimondi score of 0 to 2 does not give any useful hand function, whereas scores of 3 to 5 gives some useful hand function (Haerle and Gilbert, 2004). Moreover, motor recovery was tracked using neurophysiological methods, including faradic and galvanic tests. Tests were performed by the second author (CA) every 3 months postoperatively.
The motor recovery following CC7 transfer to lower and upper roots.
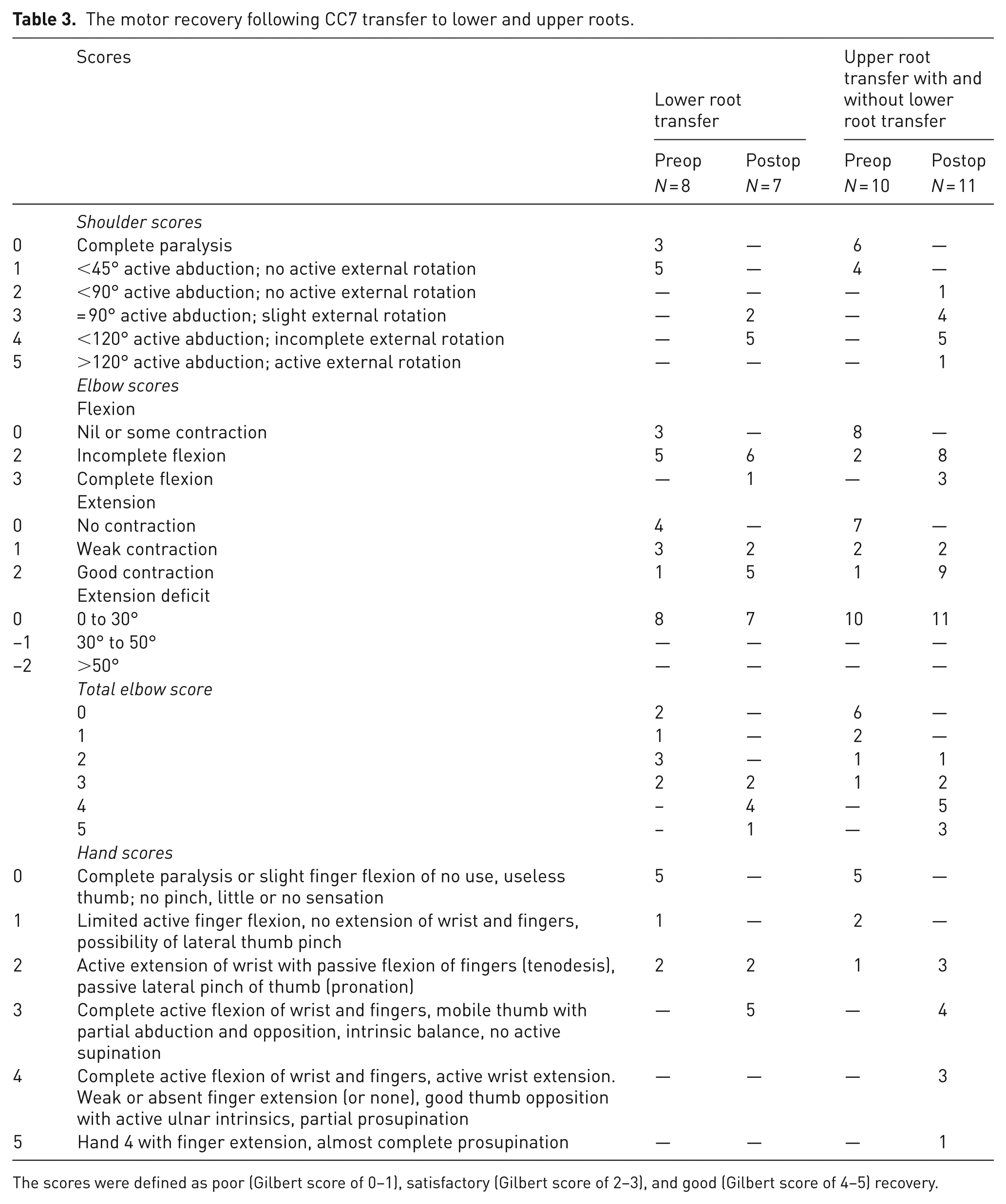
The scores were defined as poor (Gilbert score of 0–1), satisfactory (Gilbert score of 2–3), and good (Gilbert score of 4–5) recovery.
Detailed sensory assessment is very difficult in young children. The minimum age for Semmes Weinstein Sensory Testing and stereognosis is 6 years old, when most children can follow directions (Ho, 2015). We prefer to use the Narakas Sensory Grading System to evaluate hand sensation. Narakas has classified the sensory response into four grades based on response to pain, touch and light touch (Narakas, 1985). The grading system is: S0, no reaction to painful or other stimuli; S1, reaction to painful stimuli but not to touch; S2, reaction to touch but not to light touch; and S3, apparently normal sensation (Narakas, 1985).
Donor-side morbidity including motor deficit, sensory abnormality and synchronized motion were evaluated. Motor deficit, evaluated by physical examination, includes CC7-innervated motor weakness, including shoulder adduction, elbow extension, wrist and finger extension (Yang et al., 2015). Early sensory abnormality, including abnormal two-point discrimination, numbness, hyperalgesia and hypoalgesia, is usually experienced by patients following a CC7 transfer. Assessment of sensory abnormalities is difficult in children because assessment is mostly based on patient-reported interview or physician-measured sensory testing (Yang et al., 2015). Assessment of sensory abnormalities, including detailed sensory evaluation of pain with pinprick test, light touch test with a piece of cotton, pressure sense with Semmens Weinstein monofilament test and two-point discrimination test, could not be assessed in this study group of young children. Synchronized movement, which is defined as spontaneous contractions of muscles on the affected side innervated by the roots repaired by CC7 in synchrony with movements of donor limb muscles supplied by the C7 root, were also evaluated (Chen et al., 2007). Assessment of synchronized movements of the donor limb includes the evaluation of the muscles innervated primarily or partially by the C7 root. Primary motor functions of the C7 nerve root include adduction of the shoulder and extension of the elbow, wrist and fingers. Movements partially contributed by C7 include flexion of the elbow, wrist and fingers.
Results
The mean follow-up period was 45 months (range, 19–71; SD 18.2). Of the 20 children, two children (7, 10) did not complete the preoperative assessments and two (1, 3) did not complete the postoperative assessments. All children showed improvement in motor and sensory function.
The results are presented in two subgroups: (a) lower (C8, T1) root transfer (nine children); and (b) upper (C5–C7) root transfer with (nine children) or without (two children) lower root transfer (Tables 1 and 2).
The results of motor recovery are presented according to the Gilbert classification system. In the lower root transfer group four children (1, 6, 8, 9) had only lower root reconstruction by CC7 transfer; the remaining five children (2, 3, 4, 5, 7) had ipsilateral nerve transfer to upper roots in addition to CC7 transfer to lower roots (Table 1). Number 7 did not complete the preoperative assessments and two children (1, 3) did not complete the postoperative assessments. The results are shown in Table 1. In the lower root transfer group, none of the children had useful hand function (Gilbert score of 0–2) preoperatively. After reconstruction, five children (2, 4, 5, 7, 9) achieved a score of 3, which represents some useful hand function (Tables 1 and 3). Cases 6 and 8 scored 2, which represents poor hand function. Number 6 had surgery at the age of 17 months. Number 8 lives abroad and did not receive the complete physiotherapy programme. Postoperative shoulder and elbow functions were good or satisfactory (Gilbert score of 3–5) in all children in the lower root transfer group whose preoperative scores were poor (Gilbert score of 0–1) (Table 3). Only case 5 could achieve full elbow flexion comparable with the opposite side following surgery. However, six children (2, 4, 6, 7, 8, 9) had striking improvements in flexion (Table 1). All patients could perform at least 90° of elbow flexion.
The upper root transfer with or without lower roots transfer group consisted of 11 children. In nine of them, CC7 was transferred to both upper and lower roots (11, 12, 13, 14, 15, 16, 18, 19, 20) and in two of them to upper roots only (10, 17) (Table 2). All children had poor shoulder scores (Gilbert score of 0–1) with less than 45° active shoulder abduction preoperatively. After the operation, six children (10, 11, 13, 14, 15, 17) had good shoulder function with approximately 120° abduction and five had satisfactory shoulder function with approximately 90° abduction (Table 2). All cases, except cases 13 and 15, had no elbow flexion or extension preoperatively (Gilbert score of 0–1). Postoperatively, three children (11, 12, 17) could achieve full elbow flexion; the remainder had incomplete elbow flexion (approximately 120°). Cases 18 and 19 had weak elbow extension; the remainder had good elbow extension (Table 2). Seven children had poor hand function, ranging from complete paralysis to limited active finger flexion, and three had useful hand function with active finger and wrist flexion, and a mobile thumb preoperatively. Postoperatively, all children showed improvement; eight cases could achieve useful hand function. Three cases (16, 18, 20) whose preoperative scores were 0–1 improved to 2 on the Gilbert score (Table 3). Cases 16 and 18 did not receive our physiotherapy programme due to issues at home.
In all cases, recovery of sensory function of the hand was seen within 8 months of surgery. A total of 15 children had a Narakas score of S3, whereas the remainder had a score of S2 (Tables 1 and 2). We also observed an improved ability of the children to use their injured limb in daily activities.
There was no permanent impairment of donor limb function. Two children had transient weakness of elbow extension; this recovered within 6 months. Synchronized movement patterns were observed in 11 children at final follow-up. No children complained of pain in the donor limb. Parents did not report any change in use of the donor side.
Complications
In one case with mitochondrial myopathy, ventilatory support was needed for 4 weeks postoperatively. Electromyography studies of the diaphragm did not reveal any neuromuscular activity; a biopsy of the diaphragm showed no evidence of muscle fibres. Subsequent plication of the diaphragm has helped.
Discussion
The aim of surgical reconstruction of OBPI is to regain functional use of the injured limb for bimanual activities (Krumlinde-Sundholm and Eliasson, 2003). Even with satisfactory surgical nerve reconstruction there will be a poor outcome if the child does not use their extremity.
In intraplexal coaptation of the nerve grafts, the proximal stumps of the already injured nerves are used as donors. Theoretically, these nerve stumps provide fewer axons than uninjured nerves. Transfer of an uninjured CC7 nerve may provide more axons compared with ipsilateral donors (Chuang, 1995). Using long intercalated nerve grafts is a major concern. Although direct coaptation of CC7 with the injured trunks is possible in adults (Wang et al., 2013), it was impossible in our patients. The possibility of future limb length discrepancy in severe OBPI infants precludes humeral shortening. To shorten the intercalated nerve grafts lengths, we developed an endoscopic technique to shorten the route of the CC7 transfer. Endoscopic-assisted transfer of the CC7 nerve provided direct visualization of the interval between the oesophagus and prevertebral fascia. During the procedure, direct visualization and gentle traction on the grafts using suction through the arthroscope is possible; this may be safer than the open technique.
When compared with the preoperative findings, improvement in motor function was obtained for the shoulder, elbow and hand in OBPI children following the CC7 nerve transfer. Recovery of hand functions following lower trunk reconstruction is usually limited. El-Gammal et al. (2010) reported the results of hand recovery, analysed dependent upon the condition of the T1 root with a mean follow-up of 4.2 years. Of nine cases with T1 root avulsion, four cases younger than 9 months old could achieve a score of three or more, with satisfactory intrinsic function. Of 18 cases, only eight could achieve a functional hand score, even if the T1 roots were apparently intact at surgical exploration (El-Gammal et al., 2010). Pondaag and Malessy (2006) reported the outcome of hand function in 16 cases following primary reconstruction after a mean follow-up of 50 months. In their series, useful hand function was restored in ten cases with a Raimondi score of three or more. The authors concluded that restoration of hand function should be the first goal of nerve repair in infants with a flail arm. Haerle and Gilbert (2004) presented a series of 73 infants with complete paralyses with a mean follow-up of 6.4 years. The results included the outcome of combined treatment of nerve repair and tendon transfers. Good recovery of hand function was obtained in 35% patients at 2 years and 69% patients at 4 years (Haerle and Gilbert, 2004). Kirjavainen et al. (2008) reported the hand function of 105 patients who underwent surgical reconstruction with a mean follow-up of 13.4 years. Motor function was poor in patients with total palsy with a mean Raimondi score of 2.2. The authors concluded that better motor and sensory hand function could be regained with lower root reconstruction (Kirjavainen et al., 2008), supporting the results of Anand and Birch (2002). In our series, functional recovery in the hand was observed several months after surgery and improved thereafter. The use of CC7 for the reconstruction of the lower roots may provide better results in comparison with previous reports. In our study, the mean Raimondi hand score was 2.7 in patients with lower root transfer and 3.2 in patients with upper root transfer, after a mean follow-up of 44 months. At 4 years, 72% of the children achieved a score of three or more with a useful hand. The uninjured CC7 might be a very rich source for axons, in comparison with available but relatively damaged ipsilateral roots. As the recovery may continue to occur for many years, the results of long-term follow-up studies may clarify the optimal surgical strategy.
Intact hand sensorimotor function is an important way for a child to experience the environment, as sensory experience and feedback through the hand helps develop coordinated movements (Henderson and Pehoski, 1995). We proposed that rapid recovery of hand sensibility might help children to engage their affected limbs in a range of activities before sufficient motor recovery was obtained. In 12 cases, although the C8 root was avulsed, T1 was anatomically intact. In these cases, although there was no response to the stimulation of T1, it was left untouched, but the C8 root was reconstructed. We believe that the recovery took place at least partially from the CC7 as the cutaneous sensory stimuli of the injured side were perceived partly at the contralateral side. Dumont et al. (2001) reported that the sensory feedback system was associated with motor processing of movements and may influence body perception. Further studies are warranted to quantify sensorimotor alterations with objective measurements.
The possibility of controlling the repaired extremity with transhemispheric cortical reorganization is a concern (Jiang et al., 2010; Zuo et al., 2010). A high degree of transhemispheric cortical plasticity occurred after a CC7 nerve transfer in a rat model (Stephenson et al., 2013). Clinical experience over the last 20 years showed that using the CC7 nerve as a donor caused no significant loss of motor and sensory function in donor extremities (Chuang et al., 1993; Liu et al., 1997; Terzis and Kokkalis, 2009; Waikakul et al., 1999). Compared with the hemi-C7 transfer, a whole C7 transfer provided better recovery and preserved sensory function (Gao et al., 2013). In the present study, transient weakness of elbow extension was observed on the donor side in two patients. However, none of the families showed or reported any significant functional loss on the donor side at the final follow-up.
In the postoperative period, immobilizing the neck and upper extremity in a position that allows a tension-free neural coaptation may contribute. Facilitation of selective motor reorganization of the affected limb is important throughout the rehabilitation process for developing coordinated asynchronous movements of the affected limb.
There are several limitations to this study. The evaluation of sensory and motor functions in infants and children with OBPI is difficult. Follow-up after surgery is relatively long in this patient group. This may cause some difficulties in the regular visits during wintertime and for the patients with long travel distances. We believe that motivation of the children and their families is of upmost importance for adherence to the physiotherapy programme in the long term.
In cases with limited proximal donor nerves, whom have less than three available donor nerves, CC7 offers a rich source for the axonal growth, especially for hand function in addition to conventional reconstruction of the upper brachial plexus using intra- and extraplexal nerves. Establishment of the tunnel and transfer of the CC7 root and nerve grafts under direct visualization with the arthroscope is a safe and quick technique.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The authors confirm that the principles outlined in the Declaration of Helsinki were followed in this study and all patients provided written informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.