
Abstract
Repeated local corticosteroid injections have become a common mode of treatment for carpal tunnel syndrome, despite an existing recommendation that no more than three injections should be given. We studied the clinical outcomes in 254 patients who initially opted for a corticosteroid injection into their carpal canal during 2007. Follow-up records of treatment were obtained for 157 patients of whom 41% had proceeded to surgery by 2015. A mean of 1.9 injections had been given before surgery. In the unoperated group, a mean of two (range 0–12) further injections had been given. The final subjective severity and functional status scores measured using the Boston carpal tunnel questionnaire were significantly lower in the operated than in the unoperated group, but both groups improved significantly from baseline. The differences between the final scores are less than the estimated minimal clinically important difference for these measures. We conclude that repeated steroid injection may be a valid treatment option for some patients with carpal tunnel syndrome.
Keywords
Introduction
A corticosteroid injection into the carpal canal (referred to hereafter as a steroid injection) has been clearly demonstrated to be an effective short-term treatment for carpal tunnel syndrome (CTS) (Marshall et al., 2007). Despite their demonstrated short-term efficacy, local corticosteroid injections remain unpopular with many surgeons, being perceived as either ineffective in the long term, risky or prejudicial to the outcome of subsequent surgery. Quantifiable data on the risks of one or more injections to the carpal tunnel is lacking, but the idea that prior injection prejudices the outcome of later surgery appears to be unfounded (Bland and Ashworth, 2016). Little is known about longer-term outcomes. One early study suggested that 92% of patients initially given two injections of 15 mg methylprednisolone had relapsed after 2 years (Girlanda et al., 1993). More recently in the steroid injection arm of a randomized controlled trial, 50% of 30 patients initially injected with 40 mg methylprednisolone were still in remission after 1 year (Dammers et al., 1999). A further study in the Netherlands found remission rates of 63% at 6 months, 48% at 12 months and 34% at 18 months after a single injection of 40 mg methylprednisolone (Visser et al., 2012).
Many patients who have experienced marked remission of symptoms after a first injection return to our clinic asking if the injection can be repeated. Our literature search found no formal studies of repeated injection as a long-term treatment strategy. Despite the lack of evidence, the European Federation of Societies for Surgery of the Hand (FESSH) has recommended that no more than three injections should be given to one wrist (Huisstede et al., 2014).
There is little evidence relating to second injections. In the study by Girlanda et al. (1993), 26 hands were injected twice, with mean remission periods of 4.2 months for the first injection and 2.2 months for the second. In another trial, 29 patients who requested a second injection of betamethasone showed a median duration of response to the second injection of 3.2 months (Armstrong et al., 2004). Second injections were found to have a 72% success rate in a trial of different doses (Dammers et al., 2006). There is a single study specifically attempting to assess the outcome of second injections in comparison with first injections (Ashworth and Bland, 2013). This found no significant difference in either initial response rate, measured in terms of improvement in the symptom severity scale (SSS) of the Boston carpal tunnel questionnaire (Levine et al., 1993), or length of remission between first and second injections in the same hand, but the improvement in the functional status scale of the Boston questionnaire (FSS) was significantly greater after the second injection.
The longest follow-up reported in the literature comes from a Scottish study of 824 patients initially treated with a steroid injection (Jenkins et al., 2012). The authors searched the records of their institution for re-presentations of these patients for treatment of CTS over a 5-year period and found that 15% had had surgical decompression after 1 year and 33% after 5 years. They were unable to actively contact patients who had not returned for further treatment, thus outcomes in patients who had not returned are unknown. During the 5 years of follow-up, 372 patients received a second injection, 53 a third, 21 a fourth, five a fifth and three a sixth of 20 mg methylprednisolone (personal communication from the authors, Paul Jenkins 22 Jul 2015). One other study deliberately employed multiple injections (Berger et al., 2013). Over a 1-year period, 46 (38%) of 120 patients were rendered symptom free to the extent that no further treatment was necessary using one (30 patients), two (11 patients) or three (five patients) injections.
In our clinic we have adopted a policy of allowing patients to have repeat injections as long as they are not given more frequently than once every 6 months on average (we will allow two injections at a shorter interval provided a longer interval precedes or follows these), nerve function is not measurably deteriorating on nerve conduction studies and the patient understands that this mode of treatment is unproven.
The aim of this study was to assess the long-term outcome of patients with CTS who were given one or more steroid injections. The primary end-point was an ipsilateral carpal tunnel release (CTR).
Methods
Patients were identified from the Canterbury carpal tunnel database, which contains records of all patients referred to a dedicated carpal tunnel clinic. All patients seen in the carpal tunnel clinic for management of their CTS between January and December 2007, who opted for initial treatment of at least one hand by steroid injection, were included. The exclusion criteria were: patients under 16 years of age or non-English speaking or lacking capacity (none found). There were 520 new patients who had symptoms and nerve conduction abnormalities consistent with CTS. Nerve conduction studies were carried out according to American Association of Neuromuscular and Electrodiagnostic Medicine criteria (Jablecki et al., 2002). The Boston CTS questionnaire was completed by all patients attending the clinic as part of their initial documentation at first presentation. Nerve conduction studies were graded for severity of CTS using an established scale (Bland, 2000). All patients with CTS attending the clinic are offered night splints if needed. We discussed the treatment options of splinting, steroid injection and surgery with all patients and although we advised surgery for patients with nerve conduction studies abnormalities of Grade 4 and above, the final decision as to how to treat their CTS was left to the patient. All the injections performed by us were of 40 mg triamcinolone acetate without additional local anaesthetic.
Patients were contacted by post during 2015 seeking further information on their clinical course after 2007 unless any of the following applied: they had been seen within the last year for review anyway; had died; or were already known to have had surgery.
The initial postal packs contained an introductory letter, a patient information sheet, informed consent forms and a Boston CTS questionnaire. If no response was received to the initial letter, a second mailing was sent 2–4 weeks later. If there was still no response, we attempted to contact patients by telephone. Only one hand per patient was included in the analysis. If the CTS diagnosis was unilateral, the affected hand was analysed. If it was bilateral, the hand with the worse neurophysiological grading was analysed. If both hands had equal neurophysiological grading, the patient’s dominant hand was analysed.
The primary outcome measure was the proportion of patients who went on to have surgery. Secondary outcomes were: the mean Boston questionnaire scores for the symptom severity score (SSS) and functional status score (FSS); the number of further injections; and a global patient assessments of the outcome of surgery using a Likert scale (worse – unchanged – slightly improved – greatly improved – completely cured).
Statistical comparisons were made using Student’s t-tests or one-way analysis of variance for continuous variables with approximately normal distributions, Fisher’s exact test for proportions in 2 × 2 tables and Mann–Whitney U-tests for categorical variables. We also carried out a multivariate analysis using a generalized linear model attempting to find predictors of final SSS and FSS or change in SSS/FSS.
Results
We identified 254 patients (48% of the confirmed CTS cases during the year) who met the inclusion criteria. Patient flow through the study is shown in Figure 1. Full follow-up data was obtained for 157 patients (62% of the original cohort). Supplementing this with information already available regarding the deceased and non-participant patients, we have a record as to whether the hand of interest was treated with surgery between 2007 and 2015 for 70% of the total original cohort.
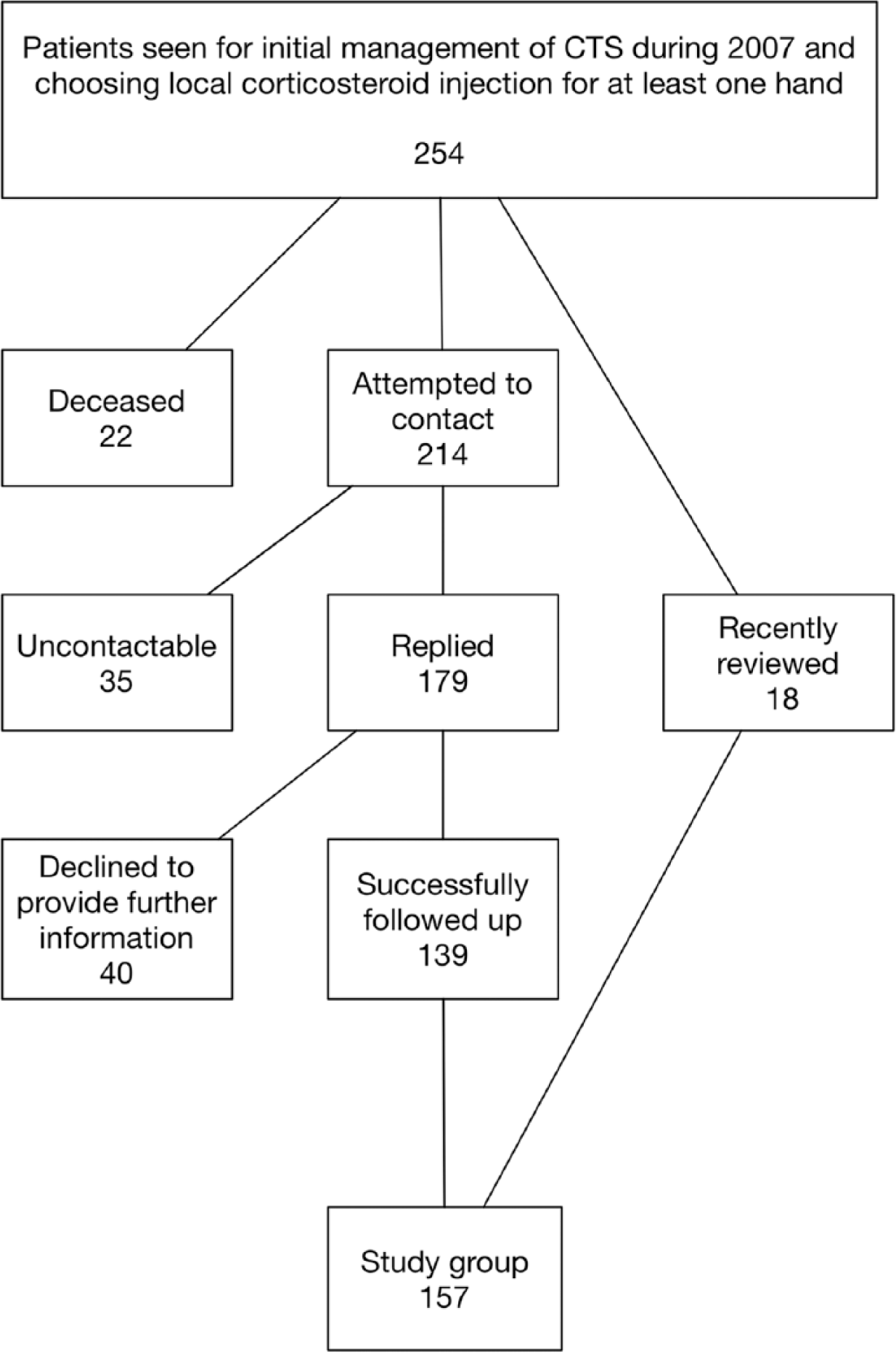
Flow diagram for study.
Demographic and baseline clinical data for the patient cohort is shown in Table 1 divided into three groups: dead patients; uncontactable patients and those who declined to provide up-to-date data; and patients with complete data. The patients who had died were significantly older at original presentation, with neurophysiologically more severe CTS. There were no significant differences in age, gender, neurophysiological results or symptom severity between the patients with complete follow-up and those who could not be contacted or declined to provide additional data. By coincidence, the age ranges for the two groups were identical.
Demographic, clinical and neurophysiological characteristics of the patient cohort.
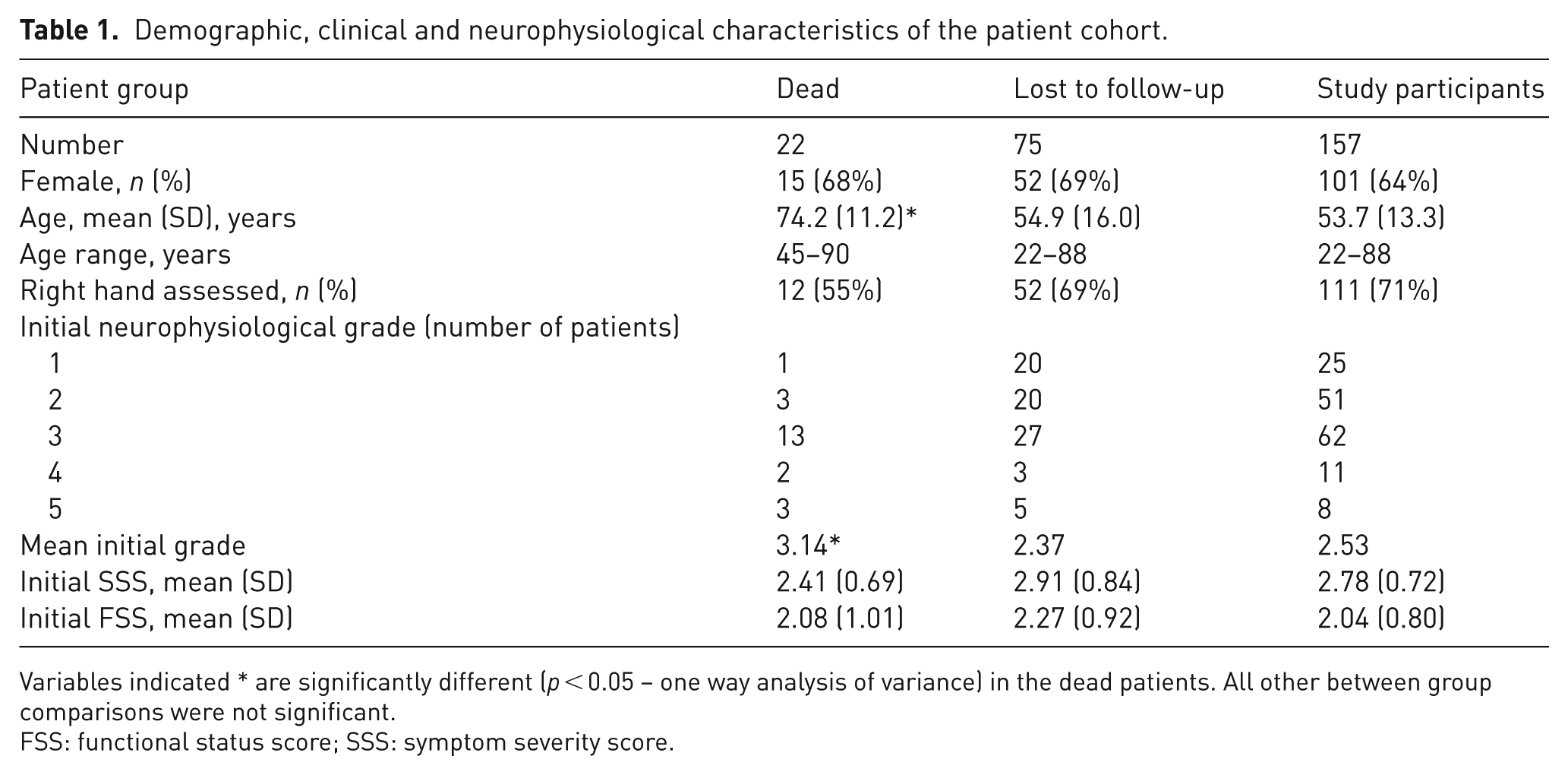
Variables indicated * are significantly different (p < 0.05 – one way analysis of variance) in the dead patients. All other between group comparisons were not significant.
FSS: functional status score; SSS: symptom severity score.
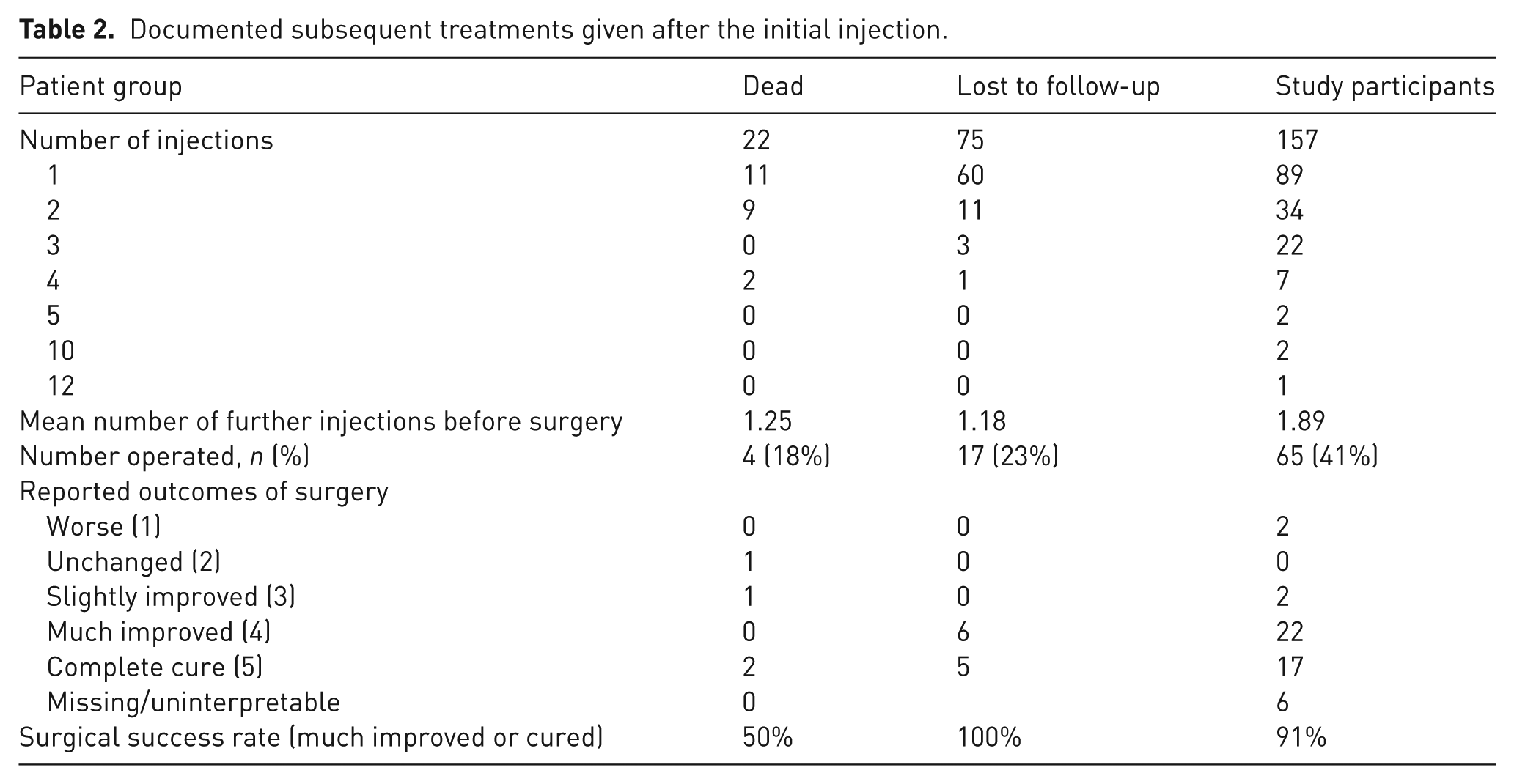
The subsequent treatments and recorded overall results of surgery for the operated patients for these groups are presented in Table 2, but it should be noted that the data for the first two groups is necessarily incomplete. As far as we have been able to ascertain, 86 patients of the original cohort (34%) were treated with surgical decompression by 2015. A total of 265 subsequent steroid injections were administered during the study period: 54 patients had two injections overall; 25 had three injections; ten had four injections; two had five injections; and one patient had 12.
Documented subsequent treatments given after the initial injection.
Fully completed Boston questionnaires are available for 128 (81%) of the study participant group. The remainder either returned only a partly completed Boston questionnaire or failed to return it. The baseline and final mean scores and the mean change in scores are summarized in Table 3. The mean recent SSS and FSS scores are significantly lower in the operated group than in the group only treated with injection, but both groups show a significant improvement from baseline in both subscales, with a difference in the final mean scores of 0.54 units for the SSS and 0.39 units for the FSS in favour of the surgically treated group. In a multivariate analysis, significant predictors of final SSS were age, the number of injections given (more injections being correlated with more severe symptoms) and having had a CTR. Significant predictors of final FSS were the number of injections given, having had a CTR and the initial FSS at presentation. Gender and starting neurophysiological grade were not significant predictors of either the final SSS or final FSS. The only significant predictor of change in SSS in a multivariate model was having had a CTR (p < 0.0001); while for change in FSS, both having had a CTR (p < 0.0001) and the number of injections given (p = 0.04) were independently significant predictors.
Comparison of SSS/FSS of operated and non-operated patients in the study group (only patients with complete initial and final scores).

FSS: functional status score; MWU: Mann-Whitney U test; SSS: symptom severity score.
No patients reported any serious complications arising from corticosteroid injection during the study period, nor were there any instances of acute exacerbation of CTS after injection.
Discussion
Observational studies of ordinary patients over an 8-year period are difficult. Inevitably some patients have died, moved away or developed other pathology over that time, which makes it impossible to achieve 100% follow-up. Nevertheless, we believe that this study provides the best available estimate of the proportion of patients originally presenting with mild to moderate CTS who will eventually need surgery, despite initial management with splinting and local steroid injection. The findings are in keeping with the only other similar previous study (Jenkins et al., 2012).
Only a limited number of patients were able to complete an up-to-date SSS/FSS during 2014–2015. Nonetheless, these results suggest that patients who had been treated only by injection had, on average, slightly more symptoms than those who had eventually had surgery. The difference however is less than the minimal clinically important difference, which has been estimated at approximately 1.0 units for the SSS and 0.7 units for the FSS (Kim et al., 2011; Ozyurekoglu et al., 2006; Rodrigues et al., 2015).
In the group for which we had full baseline and follow-up data, patients who opted for CTR during the 8-year period were significantly more likely to be female and older (Table 3), but progression to surgery was not linked to baseline neurophysiological or clinical severity.
The group of 22 dead patients is significantly different, tending to be older, with more severe CTS. Only four of these patients, to our knowledge, had carpal tunnel decompression before death. Advanced age might be considered a further factor favouring initial treatment with a steroid injection and splinting. The effectiveness of a steroid injection in CTS in the elderly has not been specifically documented and should be the subject of further study.
The study population is drawn from patients presenting in general practice and referred for direct access nerve conduction studies in an area where it is routine to investigate all such patients at presentation. It is thus representative of all patients with CTS presenting to medical attention, rather than the selected population who are referred to surgical clinics. All of the cases had documented CTS with both a consistent clinical history and abnormal nerve conduction studies.
There are limitations to this study. A total of 38% of the patients were either lost to follow-up, had died or declined to provide fully up-to-date information on their current clinical status. Therefore the data from the cohort that we were able to follow-up completely may not be truly representative. However, we do have some information regarding the other patients, derived from their existing records, demonstrating that 23% of this group are also known to have had surgery so far, and it is likely that some of them have had injections or surgery that we do not know about. The demographic and clinical characteristics, and the CTS severity of the group who could not be followed-up but are still alive, are similar to those of the study group. There is little reason to believe that the overall rate of surgery in this group would have been much higher than that in the active study participants. Even if it is assumed that all of these patients have in fact had surgery, the overall rate of surgery after 8 years of follow-up would be 140/232 = 60%.
Overall, our best estimate of the proportion of patients requiring surgery within 8 years of initial injection for CTS is 41%. We therefore conclude that a significant proportion, perhaps the majority, of patients who initially present with mild to moderate CTS will not require surgery to obtain adequate symptom relief over an 8-year period, though many of them will require multiple injections during that time. A formal prospective study will be required to determine the relative cost effectiveness of a strategy of serial corticosteroid injections compared with early surgery for CTS.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was given by the UK National Research Ethics Service, Bloomsbury.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.