
Abstract
We carried out a systematic review to determine the incidence of infection for hand surgery done in settings other than the operating theatre. Databases were searched and a PRISMA chart created by three independent reviewers. From 1200 studies identified, 46 full text articles were reviewed and six were included (two Level 3 studies and four Level 4). In three studies there were no infections after surgery in an office, procedure room or emergency department. Two studies with a combined number of 1962 procedures reviewed carpal tunnel decompressions and reported identical infection rates of 0.4%. Although the current evidence is of poor quality, it suggests that some types of hand surgery may be done outside the operating theatre without increasing the risk of infection.
Introduction
Most hand operations can be carried out under local or regional anaesthesia as day case procedures, and the indications for this are continually expanding in order to streamline patient care, improve efficiency and save money. There is an assumption that infection control requires that all invasive surgical procedures should take place in an operating theatre (OT) with full sterility, although this is more expensive and less efficient than the alternatives, such as day-surgery theatre suites, general practice procedure rooms, outpatient clinic procedure rooms, emergency department minor operations theatres and surgeons’ offices (Dillon et al., 2009; Finn and Crook, 1998; Leblanc et al., 2007; Webb and Stothard, 2009). There are also variations on infection control guidelines for each location in respect of air conditioning systems, skin preparation and draping, surgical attire and restriction in movement of personnel.
The aim of this study was to systematically review published work to compare surgical site infection (SSI) in surgical procedures on the hand done in different locations.
Methods
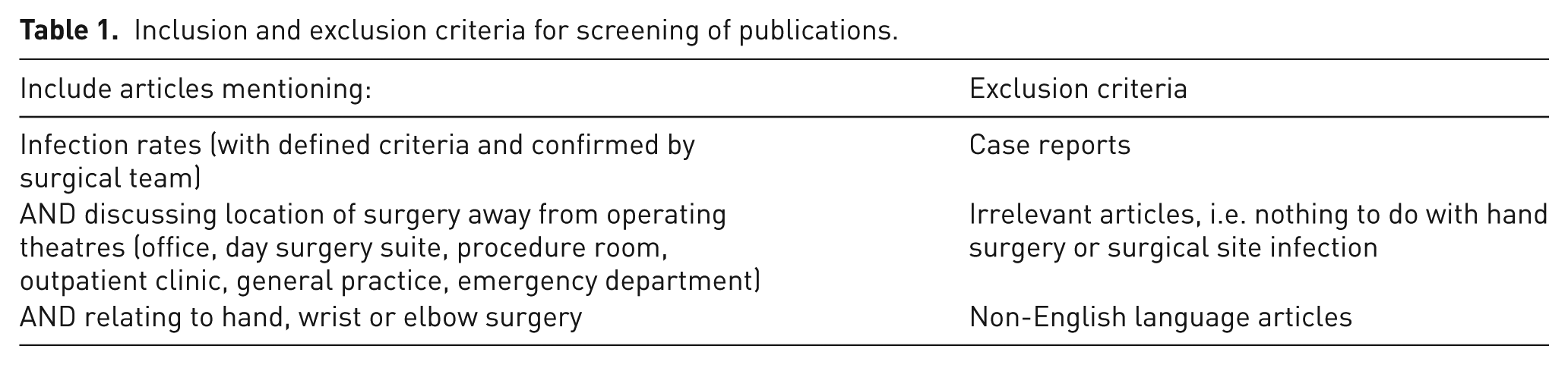
A strategy was designed for a sensitive, inclusive search of Medline, Embase and the Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases for all articles up to November 2015 (Appendices 1–3, available online). Further searches were done specifically looking for links between ‘field sterility’ and hand surgery (Appendix 4, available online). Titles and abstracts were screened by two independent reviewers (NAJ and SI), with arbitration provided by the senior author (DF) when required. Duplicates were removed and a shortlist created using the eligibility criteria highlighted in Table 1. Full texts of all shortlisted articles were then reviewed using the same criteria for final selection as in the systematic review. We included all levels of evidence apart from case reports, because the incidence of infection cannot be calculated from a single case. Data were independently extracted onto a proforma, and disagreements were resolved by consensus discussion between the reviewers and the arbitrator.
Inclusion and exclusion criteria for screening of publications.
Results
Search results
The PRISMA flow chart shows the combined results from searching all three databases (Figure 1). There were 907 titles initially identified with the search strategies in Appendices 1–3, plus another 293 from Appendix 4. Based on the inclusion and exclusion criteria in Table 1, 46 articles were selected for full text review. It was unclear from most of the abstracts of these articles where the surgery had been done, hence the requirement for reviewing the full text. Only six articles fulfilled the criteria for analysis in the systematic review (Table 2). In five of these, operations were done in a minor procedures room (PR) away from a theatre suite (Denkler, 2005; Derkash et al., 1996; Leblanc et al., 2011; Starker and Eaton, 1995; Webb and Stothard, 2009). In the sixth, surgery was carried out in a day surgery suite separate from the main theatre suite (Hashemi and Blakeley, 2004).
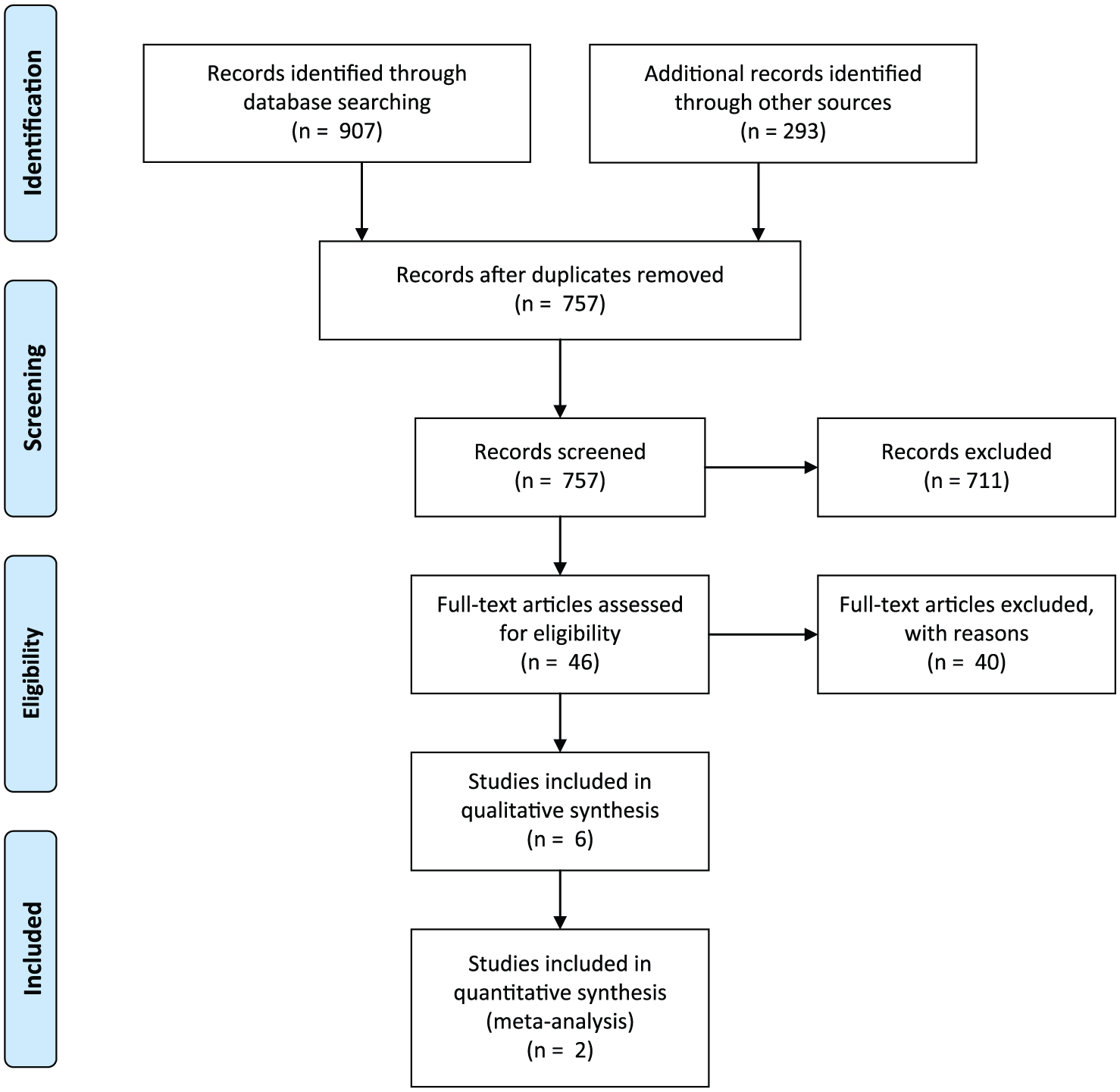
PRISMA flow diagram.
Articles selected from systematic review for analysis.
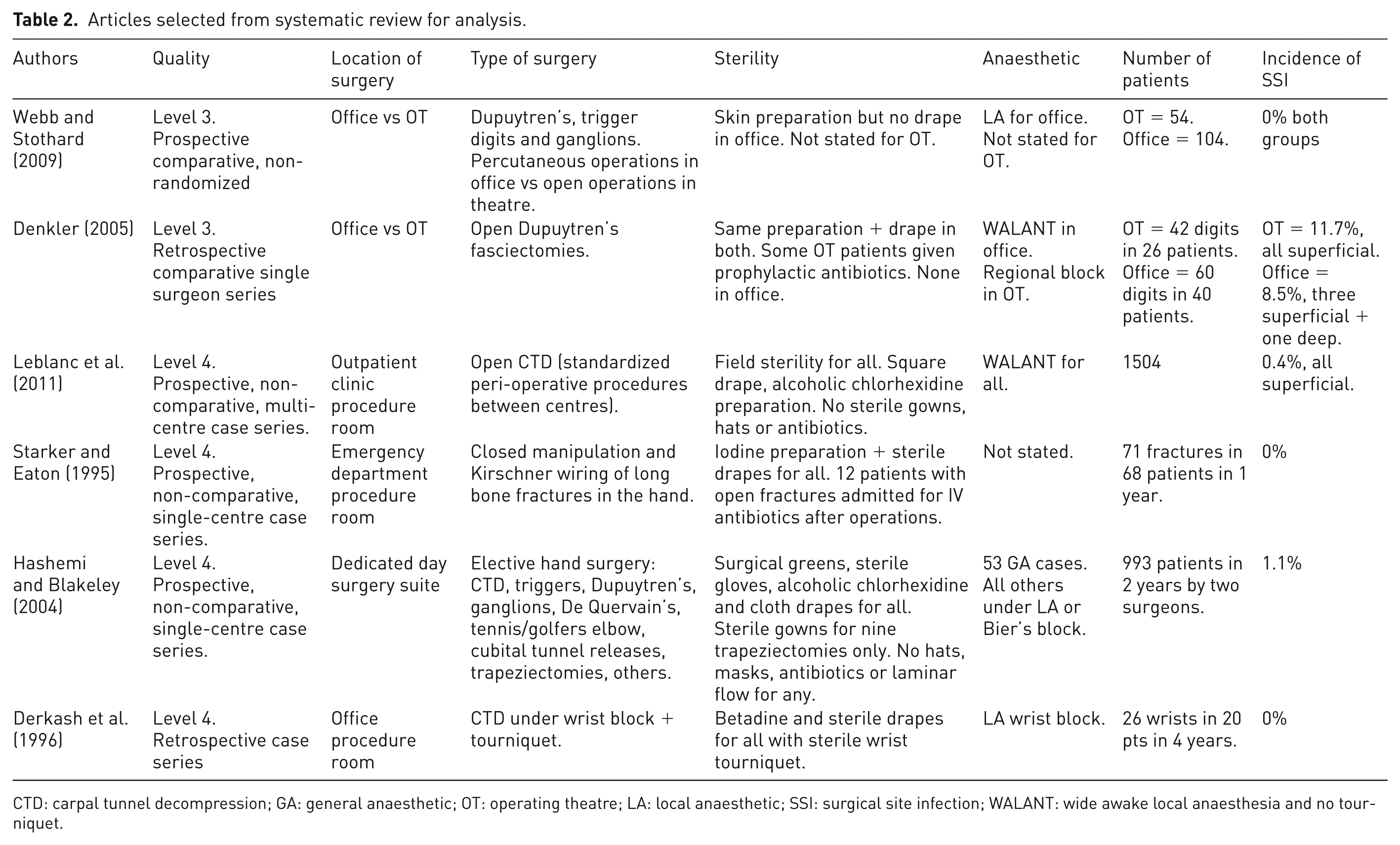
CTD: carpal tunnel decompression; GA: general anaesthetic; OT: operating theatre; LA: local anaesthetic; SSI: surgical site infection; WALANT: wide awake local anaesthesia and no tourniquet.
Quality of studies (Table 2)
Two studies were Level 3 non-randomized, comparative studies, one retrospective (Denkler, 2005) and one prospective (Webb and Stothard, 2009), both comparing operations in an office PR with operations in an OT. Neither study was methodologically sound and both were open to selection bias. One did not compare similar procedures, as open procedures in an OT were compared with percutaneous procedures in a PR for the same conditions (Webb and Stothard, 2009). As a result, a meta-analysis could not be done.
The remaining four studies were Level 4 case series; three prospective (Hashemi and Blakeley, 2004; Leblanc et al., 2011; Starker and Eaton, 1995) and one retrospective (Derkash et al., 1996). The three prospective series benefited from large numbers and clear methodology. The methodology of the retrospective study was not explained and it contained a very small number of patients, too small to reflect an accurate incidence of SSI.
Type of surgery, sterility and anaesthesia (Table 2)
Starker and Eaton (1995) studied closed manipulations and Kirschner (K)-wiring of long bone hand fractures in an Emergency Department PR. They used iodine skin preparation and sterile drapes for all procedures, but did not state the methods of anaesthesia. The other studies looked at elective soft tissue hand procedures, although Hashemi and Blakeley (2004) included trapeziectomies.
Leblanc et al. (2011) used wide awake local anaesthesia and no tourniquet (WALANT) for 1504 carpal tunnel decompressions with a standardized procedure protocol across all centres involved. Denkler (2005) compared open Dupuytren’s fasciectomies carried out under WALANT in an office PR with the same procedure by the same surgeon under regional blockade with a tourniquet in an OT. All operations in the other studies were also done under local anaesthesia apart from a small cohort in the study of Hashemi and Blakeley (2004) who had a general anaesthetic, although further details were not provided.
Webb and Stothard (2009) compared 104 percutaneous office procedures under local anaesthesia (needle fasciotomy for Dupuytren’s disease, needle release of trigger finger or aspiration and injection of ganglia) with 54 open procedures in an OT (Dupuytren’s fasciectomy, open trigger release or open excision of ganglia). They did not state how the OT patients were anaesthetized or the methods of skin preparation.
SSIs and confounding factors (Table 2)
Three of the six studies reported no SSIs (Derkash et al., 1996; Starker and Eaton, 1995; Webb and Stothard, 2009). In the study of Starker and Eaton (1995) on emergency K-wiring, the K-wires were left proud of the skin. A confounding factor was that 12 of the 68 patients were admitted post-operatively for intravenous antibiotics for 2–3 days as the fractures were either open, or there were traumatic wounds close to the wires.
Webb and Stothard (2009) reported no SSIs in the 104 percutaneous office procedures, and also reported 0% infection for the 54 open OT procedures. Details of these OT procedures in regards to sterility, anaesthesia and confounding factors were not stated. Derkash et al. (1996) also reported 0% infection in 26 carpal tunnel decompressions in a 4-year period. Although the treatment was standardized throughout, the power of the study was not adequate to accurately establish infection rates.
Hashemi and Blakeley (2004) reported a 1.1% incidence of SSIs from 993 patients having different elective operations that they were able to follow-up for a minimum of 6 weeks. Although the procedures were all done in a day surgery theatre rather than a PR as in the other studies, the surgeons did not wear sterile gowns or masks for any of the cases apart from the nine trapeziectomies. They also stated they did not use laminar flow or give prophylactic antibiotics for any case. They used alcoholic chlorhexidene, sterile drapes and sterile gloves for all cases.
Leblanc et al. (2011) presented a multicentre series of 1504 carpal tunnel decompressions done under WALANT and in a sterile field. SSIs occurred in 0.4%. The study of Hashemi and Blakeley (2004) had a subgroup of 458 patients with carpal tunnel decompression, with exactly the same percentage of SSIs. They used local anaesthesia but provided no further details regarding tourniquet use.
Denkler (2005) reported an unusually high number of SSIs in both groups in his study on open Dupuytren’s fasciectomies: 11.7% for those done in an OT and 8.5% for those done in the office. The difference was not statistically significant, but the study was under-powered for detecting a difference in SSIs. The procedure was standardized in both locations with the same surgeon. Some of the OT group received prophylactic antibiotics, although the numbers were not recorded. Patients in each group were well matched for numbers of smokers, diabetics patients and revision cases. A small and similar proportion of patients in each group had a Penrose drain inserted subcutaneously as decided by the surgeon. One of these patients suffered a deep infection, but none of the other patients with drains became infected. The unusually high number of infections was unexplained.
Discussion
OTs have strict infection control guidelines for environmental cleaning and disinfection, sterilization of instruments, air handling and personnel management. Despite this, infections affect 2%–15% of all surgical patients and SSIs contribute to perioperative morbidity, poor surgical outcomes and total healthcare expenditure (Castella et al., 2006; Umscheid et al., 2011; Yezli et al., 2014).
In 1979, 10% of all surgical procedures in the USA were done as outpatient procedures compared with 80% in 2006, a quarter of them being done in the surgeon’s office (Horton et al., 2006). This major change has been driven by demands for convenience, efficiency and privacy. Although surgeons in the UK National Health Service (NHS) appear to be more cautious in adopting these efficiency savings, there is a moral imperative to maximize efficiency in any healthcare system.
The hand is similar to the face in that it is blessed with a rich blood supply. Hand surgeons ‘… are privileged to operate in an anatomic region that is less vulnerable to infection than most sites of the body’ (Calkins, 1998). Many hand surgeons believe that full theatre sterility is unnecessary for most procedures and they can safely be carried out elsewhere, especially if done under local anaesthesia. The common goal of ‘office-based surgery’ is to streamline patient pathways even more, so that day-case surgery is akin to a visit to one’s dentist. However, there is a wide spectrum of definitions of ‘office-based procedures’, from those done in a full theatre suite adjacent to a clinic, to procedures done on an examination couch within the clinic or office itself.
Ambulatory Surgery Centres pre-dated office-based surgery in the USA and were a highly regulated method of freeing up surgical time in main hospital OTs (Schaefer et al., 2010, Vila et al., 2003). The switch to less well regulated ‘office-based’ surgery has led to several problems and litigation in the USA, although none of this has been related to procedures under local anaesthesia (Clayman and Caffee, 2006; Clayman and Seagle, 2006; Hausman et al., 2008; Liberman, 2001; Quattrone, 2000).
When considering SSIs after operations in different locations, it is important to define the attributes of each location for air conditioning systems, cleaning practices and regulations about the movement of personnel (Ayliffe, 1991; Flanagan et al., 2011). Various terms for the location of operations have been used in studies, such as OT, day-surgery suite, office, PR or emergency department. Unfortunately, there is no standardization between studies regarding the sterility attributes of each room, making comparisons impossible.
The UK Department of Health guidelines for air conditioning systems in various clinical areas state that 25 air changes per hour (ACPH) are required in an OT ‘for sterility’, 15 ACPH are required in a day surgery suites and OT anaesthetic rooms ‘to control anaesthetic gases’ and 10 ACPH are required in a clinic PR or plaster room ‘to control odours’ (Department of Health Estates and Facilities Division, 2007; Department of Health NHS Estates, 2004). For comparison, the US guidelines state that both OTs and day-surgery centres must have 15 ACPH (American Institute of Architects, 1996, Mangram et al., 1999). No guidance is offered as to which procedures can be safely carried out in each area, and no clinical evidence for these policies is referenced within these documents, only further guidelines.
The six studies we analysed reported very low infection rates after elective and trauma hand procedures outside a main OT environment. The quality of evidence was low throughout and the studies were too heterogeneous, with too many confounding factors, to allow many comparisons between them.
The quality of evidence provided from these six studies is not sufficient to change surgeons’ practices or satisfy infection control organizations that a global change of practice is required. However, infection rates are undoubtedly low, even when operating outside the main OT environment. Infection control regulations that are applied in other orthopaedic and plastic surgery procedures may not necessarily be required for surgical procedures on the hand. There is debate about whether sterile gowns, hats and masks are required, although surgeons may prefer to wear these to protect themselves from splashes of blood and body fluids. It is important that any changes in practice remain properly regulated and with an SSI surveillance programme implemented (Calkins, 1998; Castella et al., 2006; Gastmeier et al., 2002; Horton et al., 2006; Mangram et al., 1999).
This review should prompt further research in this area, with better quality studies including randomized controlled trials. As infection rates are low, trials would need to be large enough to have sufficient power to detect a difference, which may require multi-centre trials. In the meantime, clinicians operating outside a main OT environment should audit SSIs and better define any potential confounding factors, such as air conditioning, skin preparation and draping, surgical attire and the use of prophylactic antibiotics (Haley et al., 1985). With this information, meaningful comparisons may be made and guidelines for safe, efficient and cost-effective practice produced.
Footnotes
Acknowledgements
We would like to acknowledge and thank Neal Thurley, our trust librarian, for helping to design the literature search strategies for the three databases.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.