
Abstract

Dear Sir,
We present a case of necrotizing fasciitis in a single finger. A healthy 52-year-old female presented to our unit with considerable increasing pain, mottling, discolouration and mild local swelling affecting the distal aspect of her right index finger (Figure 1). These local symptoms were accompanied by ascending lymphangitis and nausea. She was otherwise systemically well and afebrile and had no co-morbidities. Three days earlier, she had sustained a ‘paper cut’ injury to the ulnar aspect of the digit while opening a cardboard box. To stem the blood flow, she immediately placed the affected digit in her mouth. Forty-eight hours later, she experienced increasing pain, swelling and stiffness affecting the digit. No skin wound was apparent at the time of presentation. Blood cultures were taken and she was started immediately on intravenous use of Co-Amoxiclav. The initial blood tests revealed profound leucopaenia of 0.9 × 109/L, a C-reactive protein level of 36.8 mg/L and a haemoglobin (Hb) level of 134 g/dL. Radiographs of the right hand and index finger did not show any bony injury or subcutaneous emphysema. A working diagnosis of an early felon or flexor sheath infection secondary to a traumatic wound was made, and she underwent surgical debridement within 2 h.
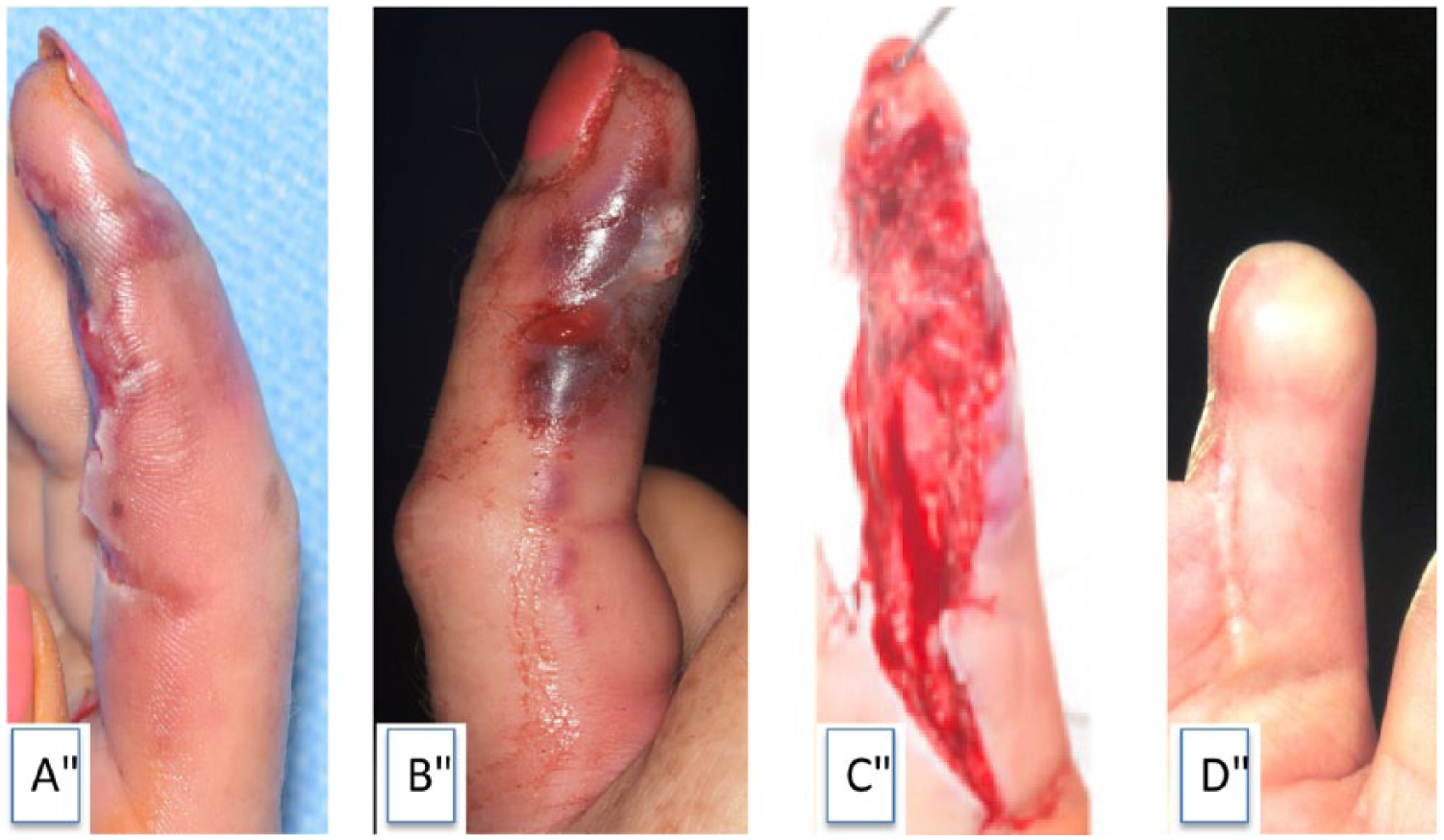
Clinical photograph of the affected digit: (A) at presentation, radial border of right index finger; (B) at presentation, ulnar border of right index finger; (C) after third debridement; and (D) the healed finger, following surgical shortening (terminalization) through the proximal phalanx.
Despite surgery, antibiotic treatment and increasing doses of pain-killers, her pain increased. The leucopaenia persisted, while the C-reactive protein increased to 210 mg/L and Hb levels decreased to 87 g/dL. She deteriorated systemically, becoming hypotensive and septicaemic, requiring inotropic support in the intensive care unit with Granulocyte-colony stimulating factor administration. The clinical picture was more in keeping with necrotizing soft tissue infection. This was confirmed by microbiology cultures, which grew invasive beta haemolytic Group A Streptococcus pyogenes and a positive Gram stain. Histopathology confirmed a diagnosis of necrotizing fasciitis, with necrosis of the tendon sheath, a weak polymorphonuclear cell infiltrate, bacteria on Gram stain, oedema of the reticular dermis and necrosis of the subcutaneous fat. Turbid fluid was present in the flexor sheath, with necrotic tissue, blistering and thrombosis of distal ulnar digital artery and subcutaneous vessels on the dorsum of the distal half of the finger. Antibiotic treatment was changed to Benzylpenicillin and Clindamycin. She underwent further debridements on Day 2 and Day 3, post-admission. The finger was surgically shortened (terminalized) through the head of the proximal phalanx due to the extent of necrotic tissue. Recovery thereafter was uneventful.
Necrotizing fasciitis of fingers is usually fast spreading, affecting the subcutaneous tissue, superficial fascia and skin. A paucity of typical signs early in the disease history and an unusual presentation make its diagnosis challenging. Through a search of the literature, we found no case reports describing necrotizing infection being limited to a single digit.
While today necrotizing infection remains relatively uncommon, a low threshold of suspicion must be maintained due to the rapid nature of its progress and significant associated morbidity and mortality. Common signs include severe pain that is disproportionate to clinical findings, local erythema, blistering, skin colour changes, subcutaneous crepitus, cutaneous anaesthesia and systemic changes such as hypotension, shock, tachycardia and an altered mental status (Hakkareinen et al., 2014). While various scores have been described in order to facilitate a probability of diagnosis, surgical debridement is key in establishing the diagnosis, assessing the extent and in managing it. Often, serial debridements are needed and definitive wound closure should be delayed until after confirmed clearance of infection. In the absence of timely aggressive management with broad spectrum antimicrobials and prompt surgery, systemic toxicity sets in rapidly with possible ensuing death (Taviloglu and Yanar, 2007). Antimicrobial infusion is commenced immediately after blood samples and tissue samples for microbiological examination, culture, Gram staining and histology have been collected. The choice of antibiotics is discussed with the microbiology team before implementation and later modified accordingly. The management of necrotizing fasciitis requires a multidisciplinary approach. While various risk factors have been elucidated, many cases occur in fit and well healthy individuals. In our patient, inoculation of the epidermal break she sustained by oral cavity streptococci, at the time of injury, might be a cause.
A low threshold for the suspicion of necrotizing infection should be maintained in patients presenting with atypical signs of infection, and any patient presenting with fulminant infection and leucopaenia necessitates aggressive treatment and investigation. Pain disproportionate to the apparent severity of the lesion should alert the clinicians to the possible diagnosis of necrotizing fasciitis.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
Both verbal and written informed consent were obtained from the patient for the publication of this case report together with the accompanying images.