
Abstract

Dear Sir,
A 4-month-old boy was referred to our paediatric upper limb outpatient clinic with a right-sided hand malformation. He had been born preterm with a gestational age of 30 weeks. On examination the hand was narrow, with 60° abduction of the little finger. Radiographs revealed a congenital metacarpal synostosis with a narrow palm and convergence of the fifth metacarpal head towards the fourth. The synostosis was classified as type C1 according to Liu et al. (Figure 1) (Foucher et al., 2001; Liu et al., 2014). An associated congenital unilateral radial head dislocation was additionally found. No family history was noted and the child was otherwise healthy. The patient was reviewed regularly until the age of 2 years and surgical correction was repeatedly recommended. The parents declined surgery despite the fact that the little finger remained abducted in the resting position. The patient did not come for further follow-up evaluation until the age of 14.5 years, shortly before he sustained an injury during sports activity. Comparison of the radiographs obtained before the trauma (Figure 2(a)) – possibly due to developing symptoms – with those after the trauma revealed that the patient had sustained a diaphyseal metacarpal fracture of the fourth metacarpal (Figure 2(b) and (c)). The fifth metacarpal was hardly visible as it was superimposed over the fourth metacarpal, mimicking cases with congenitally absent fifth metacarpals (Eren et al., 2012). However, it was evident that the short fifth metacarpal had caused a pathological fracture due to chronic pressure of its head towards the fourth metacarpal shaft (Figure 2(b) and (c)). The intraoperative findings confirmed our impression, as the base of the proximal phalanx was situated directly on the shaft of the adjacent metacarpal. The fracture was then reduced and fixed with a straight 2.3 mm four-hole plate system (Stryker®, Freiburg, Germany). The postoperative course remained uneventful and the patient was satisfied with the final result. In general, as before the injury, the patient did not complain of any functional deficit and has declined further surgical reconstruction.
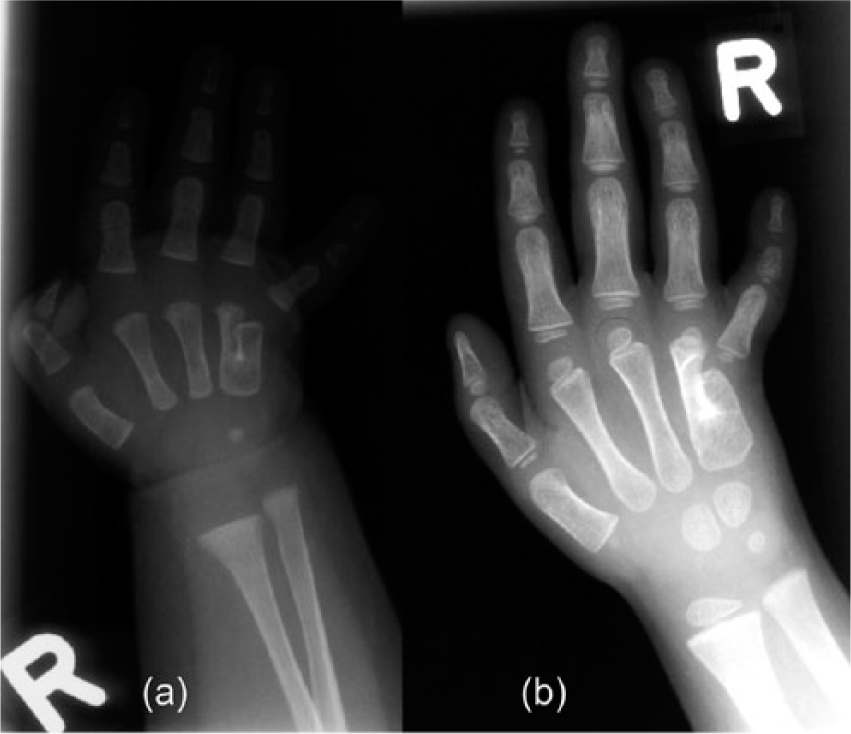
Radiographs at (a) 4 months and (b) 5 years of age show a congenital metacarpal synostosis type ‘k’ according to Foucher et al. (2001) and type C1 according to Liu et al. (2014). Note the progressive scalloping of the fourth metacarpal shaft, which can typically be found in this type.
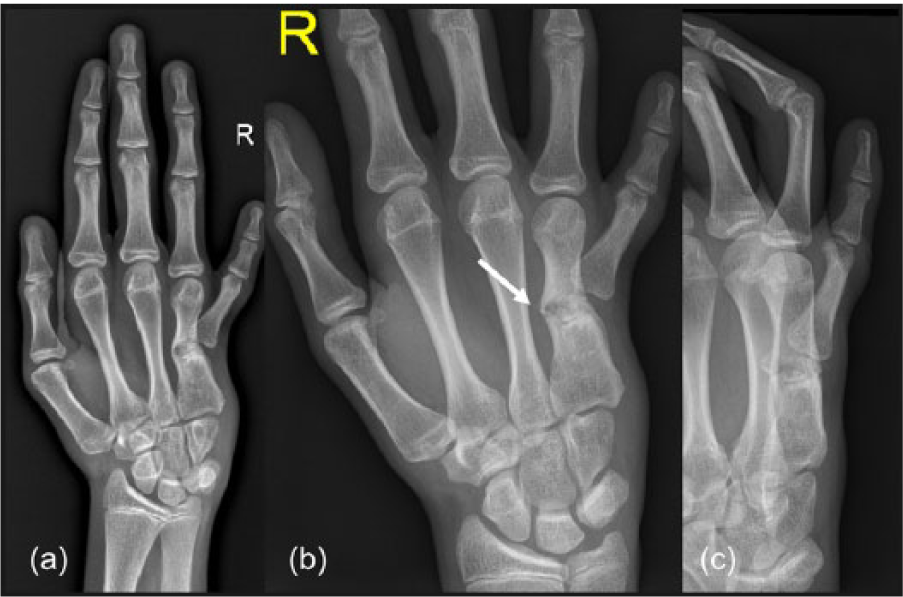
Follow-up radiographs at the age of almost 15 years demonstrate (a) increased relative shortening of the little finger, complete ‘ingrowth’ of the fifth metacarpal into its adjacent bone, leading to a marked axial deviation of the fourth metacarpal shaft (b) and (c). A minor sports injury resulted in a pathological fracture of the weakened bone (arrow).
Very few reports have previously described cases with a so-called congenital aplasia of the fifth metacarpal bone. Buckwalter et al. described seven cases with partial or complete absence of this bone; the radiological appearance of one (case ‘GC’ in their report) closely resembled that of our patient’s pre-injury radiographs (Buckwalter et al., 1981). The authors stated that there, the fifth metacarpal head was joined to the fourth metacarpal, which in turn ‘carried’ the little finger. Another case report presented a similar radiographic formation including a pseudo-joint between the little finger and the fourth metacarpal (Eren et al., 2012). However, in light of the radiographic changes in our case from shortly after birth to the latest radiographs, it seems likely that both these cases were rather metacarpal synostoses of the same classification as ours, which presented later as ‘absent’ metacarpals. We believe that the short, fused fifth metacarpal has progressively grown into the fourth metacarpal, making it difficult to distinguish between these two bones. One hint for the ‘masked’ entity of a congenital metacarpal synostosis could be the very broad base of the fourth metacarpal.
This case example emphasizes the need for surgical reconstruction in childhood in cases with a congenital metacarpal synostosis. Besides cosmetic aspects of a narrow palm and a markedly abducted little finger, the irregular growth plate of the fifth metacarpal head in severe cases may lead to abnormal growth into the adjacent metacarpal shaft. This may cause progressive bone weakening followed by a pathological fracture.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.