
Abstract
In this article, we review microsurgical reconstructive techniques available to treat thumb amputation at different levels based on our experience. We reference techniques used by other surgeons and identify the most suitable technique for different clinical situations. Indications and techniques for microsurgical partial or composite transfer of the great or second toe for thumb reconstruction are summarized. Different microsurgical transfer techniques suggest a great freedom of surgical choices. However, the choices are considerably restricted if all functional and cosmetic requirements are to be met. We recommend individualized surgical design and reconstruction because each case of thumb amputation is unique.
Keywords
Introduction
Function of the thumb is one of the most essential components of hand functionality. Loss of the thumb accounts for a loss of 50% in entire hand function. Over time, surgeons have tenaciously focused on thumb reconstruction by developing a variety of techniques for repair and reconstruction after amputation. In the late 19th century, the Austrian surgeon Nicoladoni introduced several original ideas, including the tubed pedicle flap and the toe-to-hand transfer to substitute for amputated parts of the thumb. In a 5-year-old child, he transferred the second toe to the hand as a pedicle flap (Huemer, 2005). Beginning in 1966, microvascular toe-to-thumb or toe-to-finger transfer came into clinical use and remains one of the important approaches for thumb reconstruction.
Arterial system and designs of toe transfer
The use of the dorsal arterial system of the toes (O’Brien et al., 1975), with a large artery (i.e. dorsalis pedis artery) and its long pedicle, considerably diminishes microsurgical difficulties, despite the great amount of anatomical variations of the first dorsal metatarsal artery and associated difficulties of surgical dissection (Steichen and Weiss, 1992) (Figures 1 and 2). The dorsal arterial system to the toes is used in almost all microsurgical transfers of toe tissues to the thumb.
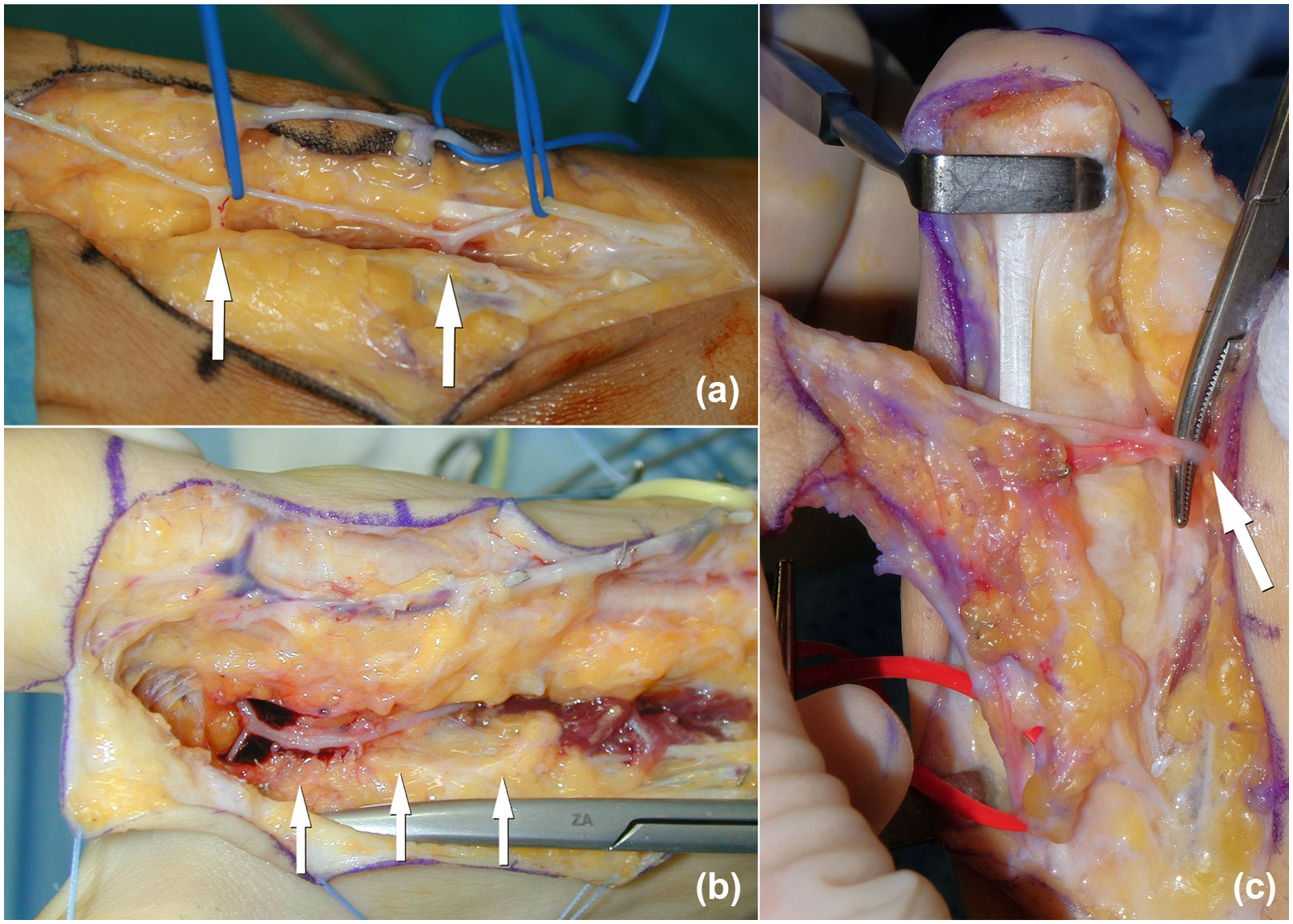
Variations of the first dorsal metatarsal artery. (a) Type IA: located dorsal to the interosseous muscle. (b) Type IB: located into the interosseous muscle. (c) Type IIB: deep to the interosseous muscle and the retrograde dissection is employed.
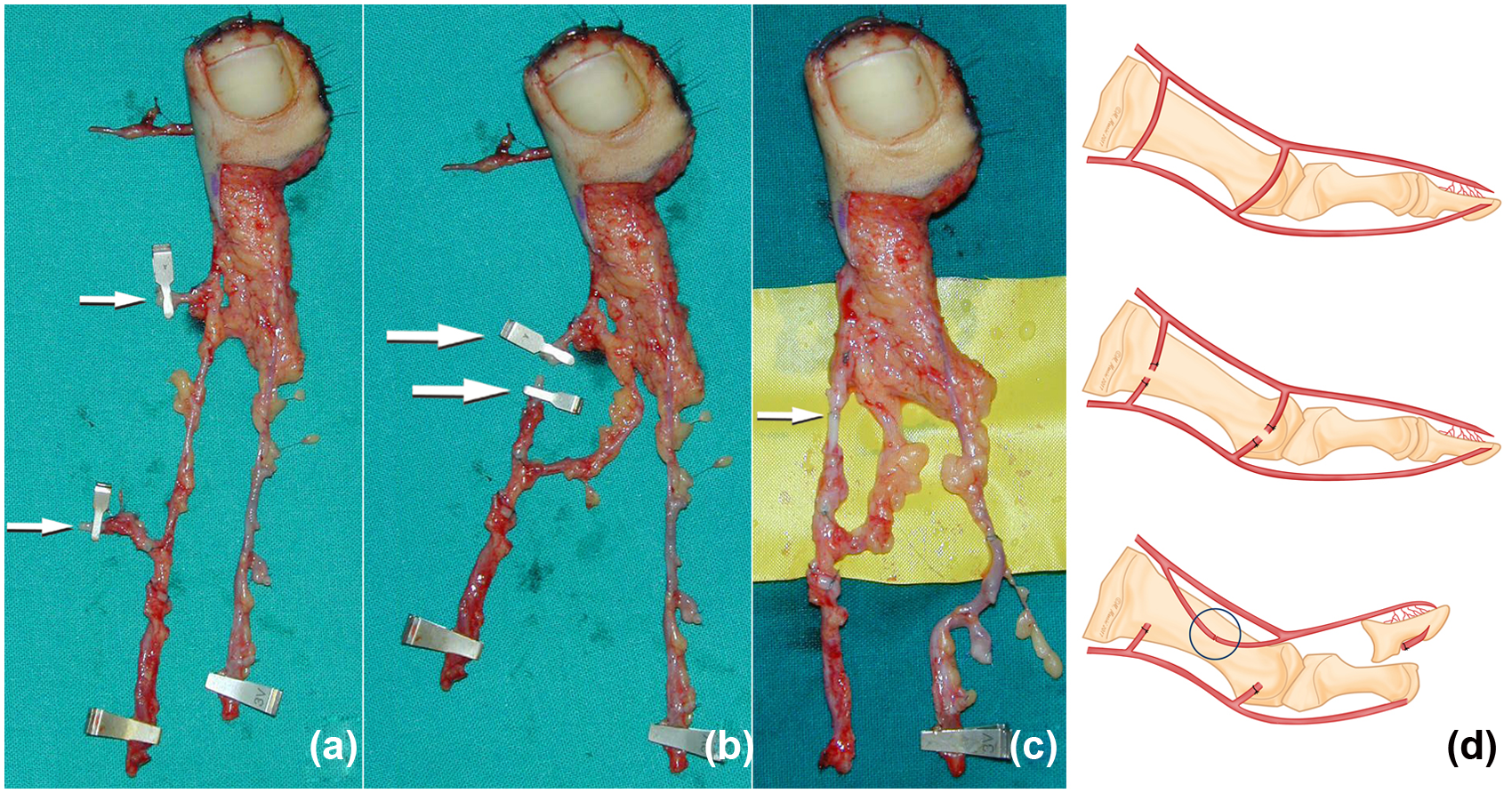
Variations of the first dorsal metatarsal artery. (a) Type IIA the first dorsal metatarsal artery is inadequate and the two communicating branches between the dorsal and the plantar system are dissected and ligated (arrows). (b) and (c) The two communicating branches are then mobilized and sutured, thus increasing the insufficient first dorsal metatarsal artery. (d) Summary of the vascular surgical procedure.
Morrison et al. (1980) introduced the wrap-around flap technique, which uses the boneless pulp of the great toe and its nail wrapped around a bone graft harvested from the iliac crest. The original technique was modified with harvesting the wrap-around flap together with a bone fragment of the distal phalanx (Morrison et al., 1984) (Figure 3). A drawback of the original and modified techniques is the absence of interphalangeal (IP) joint movement in the new thumb. Two approaches of importance preserve the IP function and reconstruct a thumb closer to normal. The trimmed toe technique (Figure 4) (Wei et al., 1988)) involves a longitudinal osteotomy to reduce the size of the great toe while preserving IP joint mobility. The twisted toe flaps technique (Figure 5) (Foucher et al., 1980) uses a portion of each of the great and the second toes. The flaps are based on a common dorsal arterial system to both toes and reduces the morbidity of the donor foot.
Wrap-around toe flap. (a), (b), (c) The distal portion of the distal phalanx is included in the flap. (d), (e) An iliac crest bone graft is placed between the two vascularized fragments to reduce the risk of graft absorption.
Trimmed great-toe flap. (a), (b), (c) This technique implicates reduction of both the bony and soft tissue components along the medial aspect of the transferred great toe. (d), (e) Final result of the transferred trimmed toe.
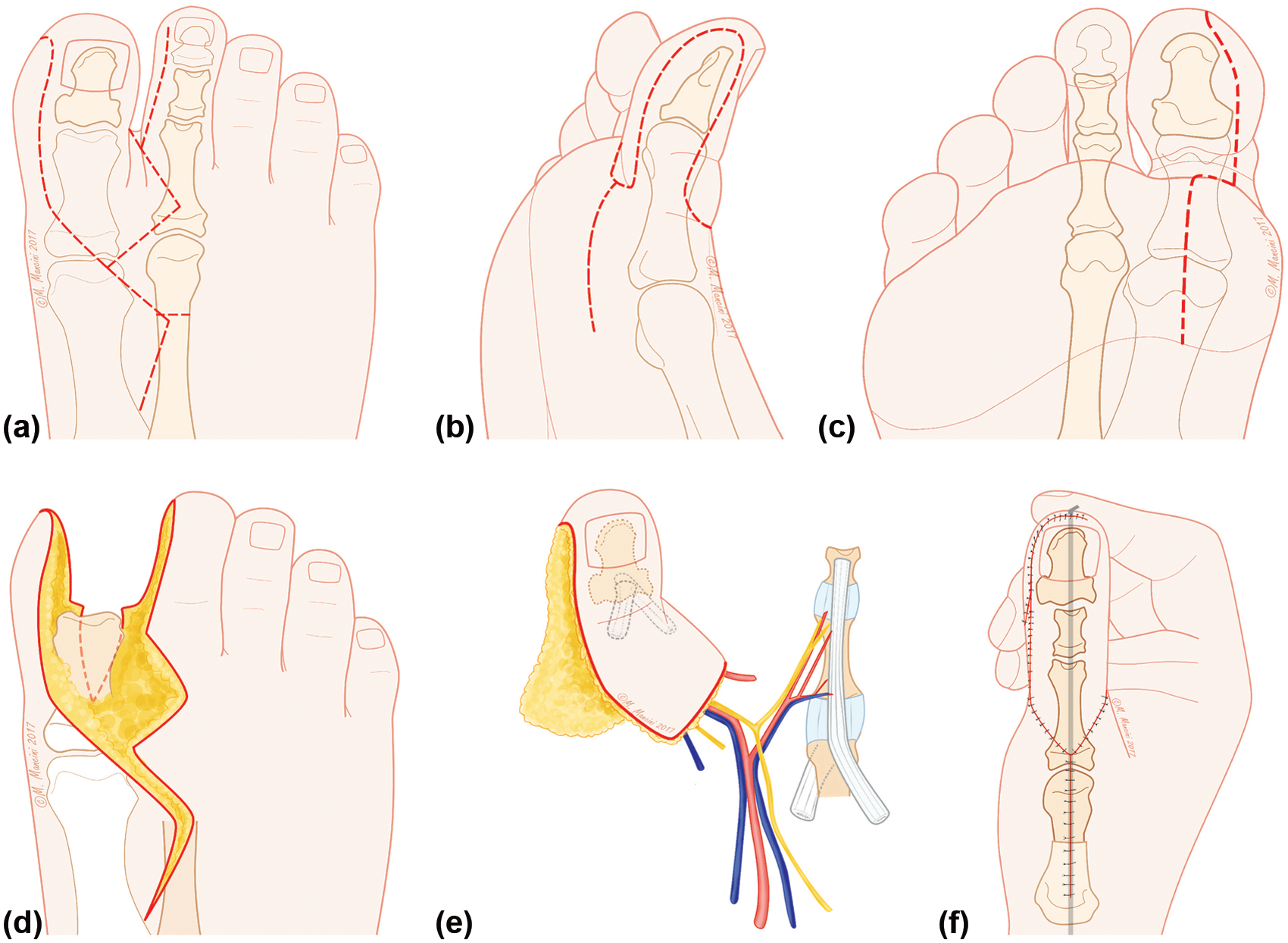
Twisted toe flaps. (a), (b), (c) Outline of the incision for harvesting the wrap-around toe-joint complex. (d), (e), (f) The thumb is reconstructed by wrapping the flap from the big toe around the second toe joint.
Goals of repair and reconstruction
The commonly used classification of thumb amputation is the Merle classification (Merle, 1991) (Figure 6) although several others are available (Leung, 1983; Lister, 1984; Morrison et al., 1984).
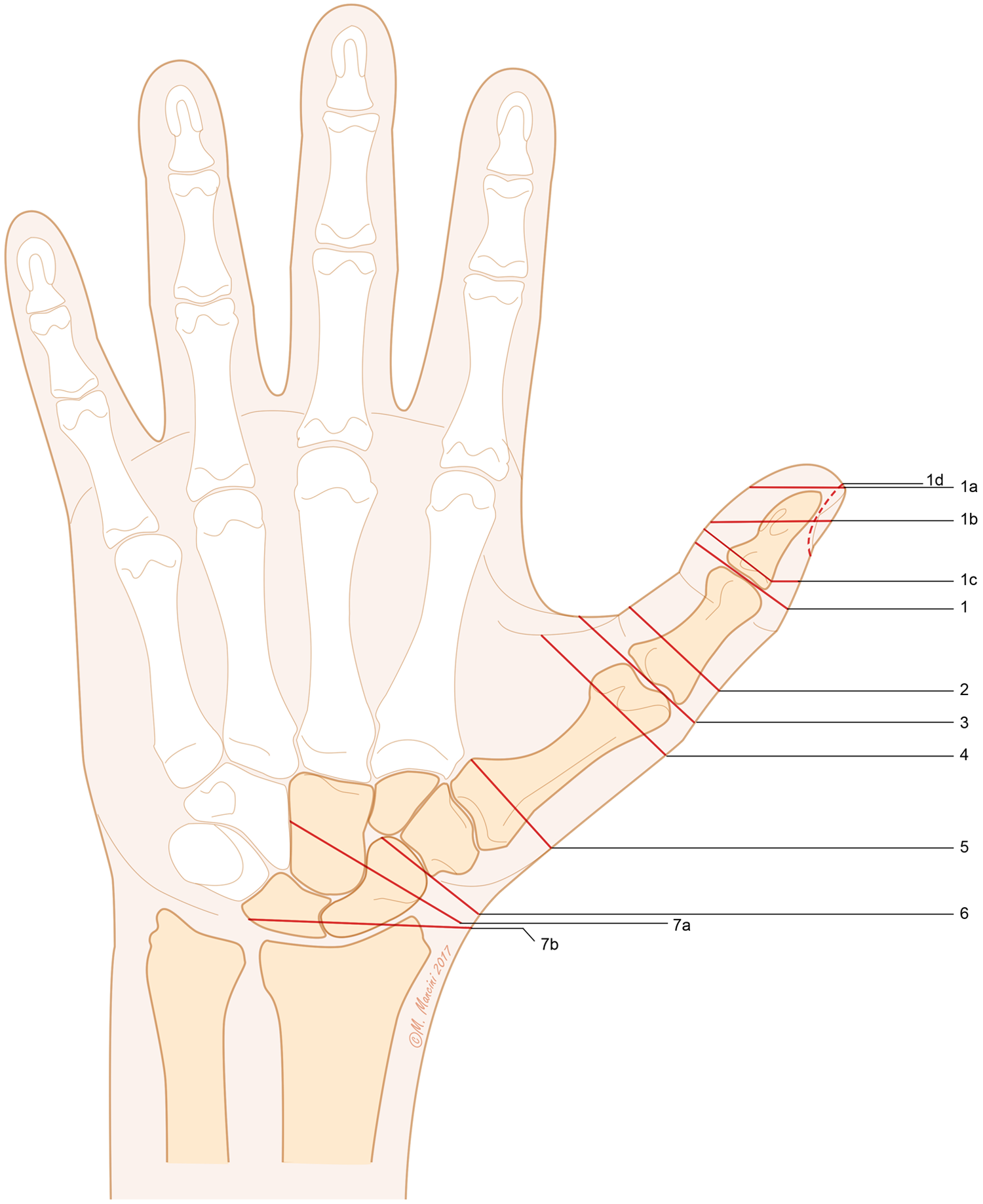
Merle’s classification of the thumb amputation level. Level 1 – amputation distal to IP joint. The amputation can be incomplete and may involve the pulp only (1a), the pulp and part of the nail (1b), the distal phalanx (1c), or only the nail (1d). Level 2 – amputation through the proximal phalanx with preservation of the metacarpophalangeal (MP) joint. Level 3 – amputation at the MP joint with integrity of the metacarpal head. Level 4 – amputation at the neck of the first metacarpal bone with preservation of the thenar muscles. Level 5 – amputation at the base of the first metacarpal bone with loss of the thenar muscles and integrity of the first carpometacarpal (CMC) joint. Level 6 – amputation at the first CMC joint. Level 7 – amputation at the wrist; 7a: trans-metacarpal and 7b: radio-carpal.
An ideal thumb repair or reconstruction should follow the reconstructive criteria suggested by Littler (1976): re-establish an opposable, sensate, stable thumb of adequate length while also considering strength and mobility. Morrison et al. (1980) introduced a novel reconstructive concept: aesthetically normal, since in aesthetic importance, the hand is second only to the face (Morrison, 1992). Considering the criteria of Littler (1976) and Morrison (1992) and our own experience, we believe that an optimal thumb reconstruction should meet three main objectives: restore thumb function, recreate its aesthetics, and minimize donor-site morbidity.
A decision on surgical methods used to achieve the above goals depends on the age, health condition, occupation, and functional demands explicitly expressed by the patient. The maximal age for complex thumb reconstruction is around 60 to 65 years old. Furthermore, a considerable number of patients in countries where open-toed shoes are worn regularly are reluctant to donate tissues from the foot (Graham et al., 2016; Sabapathy et al., 2003). Women often refuse the removal of their toes. The abnormal appearance of the donor site is a main reason why a patient rejects this option.
The patient should be thoroughly informed about the other options available: such as osteoplastic reconstruction (Cheema and Miller, 2009), pollicization (Ishida et al., 2006), osteo-cutaneous radial flap and phalangization (Graham et al., 2106; Jones et al., 2008; Muzzafar et al., 2005), and thumb lengthening (Heitmann and Levin, 2002). These methods offer a sufficiently long thumb with good function, although the result is not always aesthetically satisfactory.
Ideal indications for reconstruction
Irrespective of level of amputation after trauma, with tumour resection or as a result of congenital deficiency, partial or complete absence of the thumb can be an indication for microsurgical reconstruction (Table 1). However, most surgeons consider a thumb amputation with an intact metacarpophalangeal (MP) joint to be an ideal candidate for toe-to-thumb transfer (Graham et al., 2016; Heitmann and Levin, 2002; Waljee and Chung, 2013). Pollicization is reserved for patients with more proximal absence and without a stable carpometacarpal (CMC) joint (Heitmann and Levin, 2002).
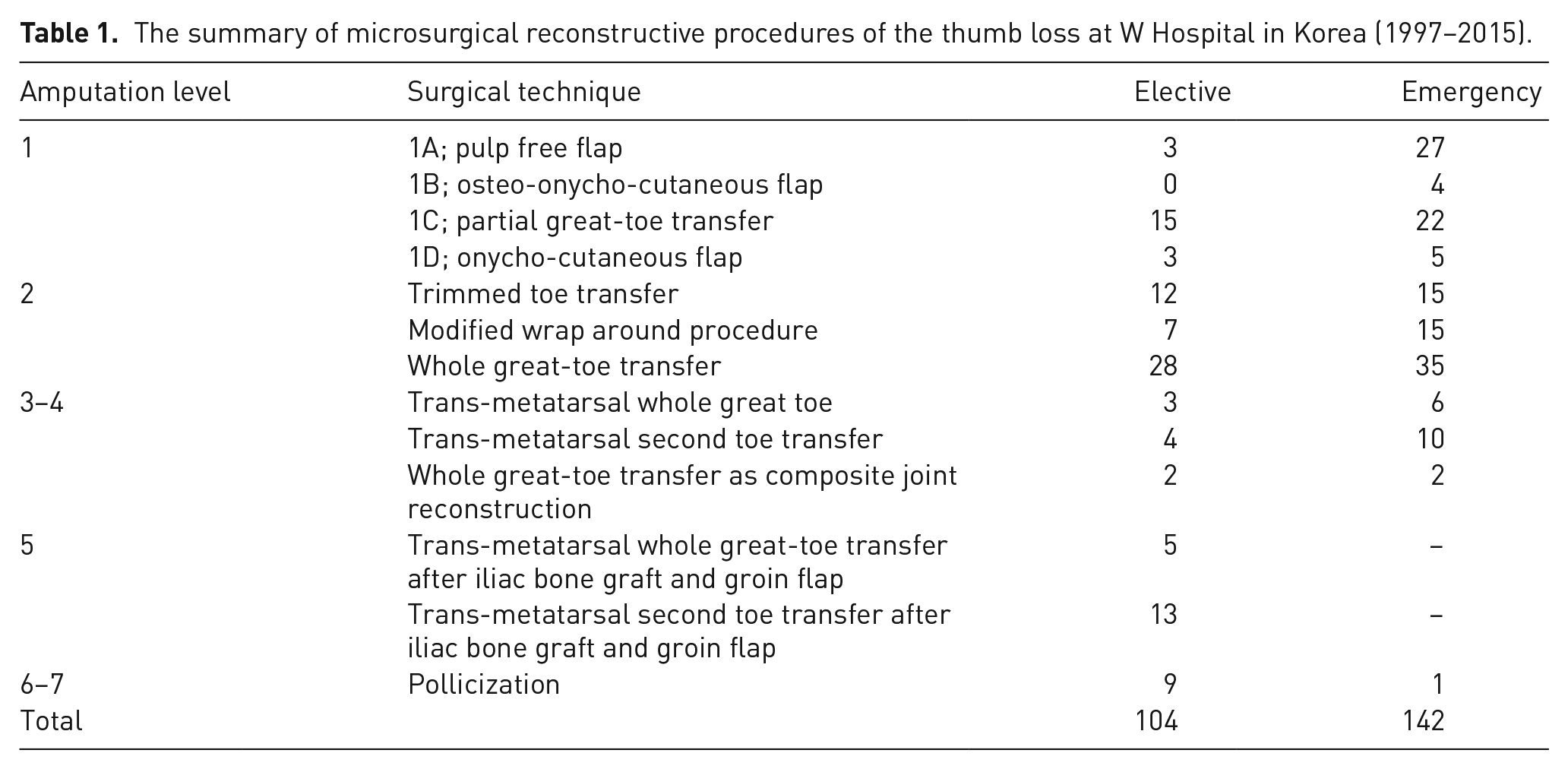
The summary of microsurgical reconstructive procedures of the thumb loss at W Hospital in Korea (1997–2015).
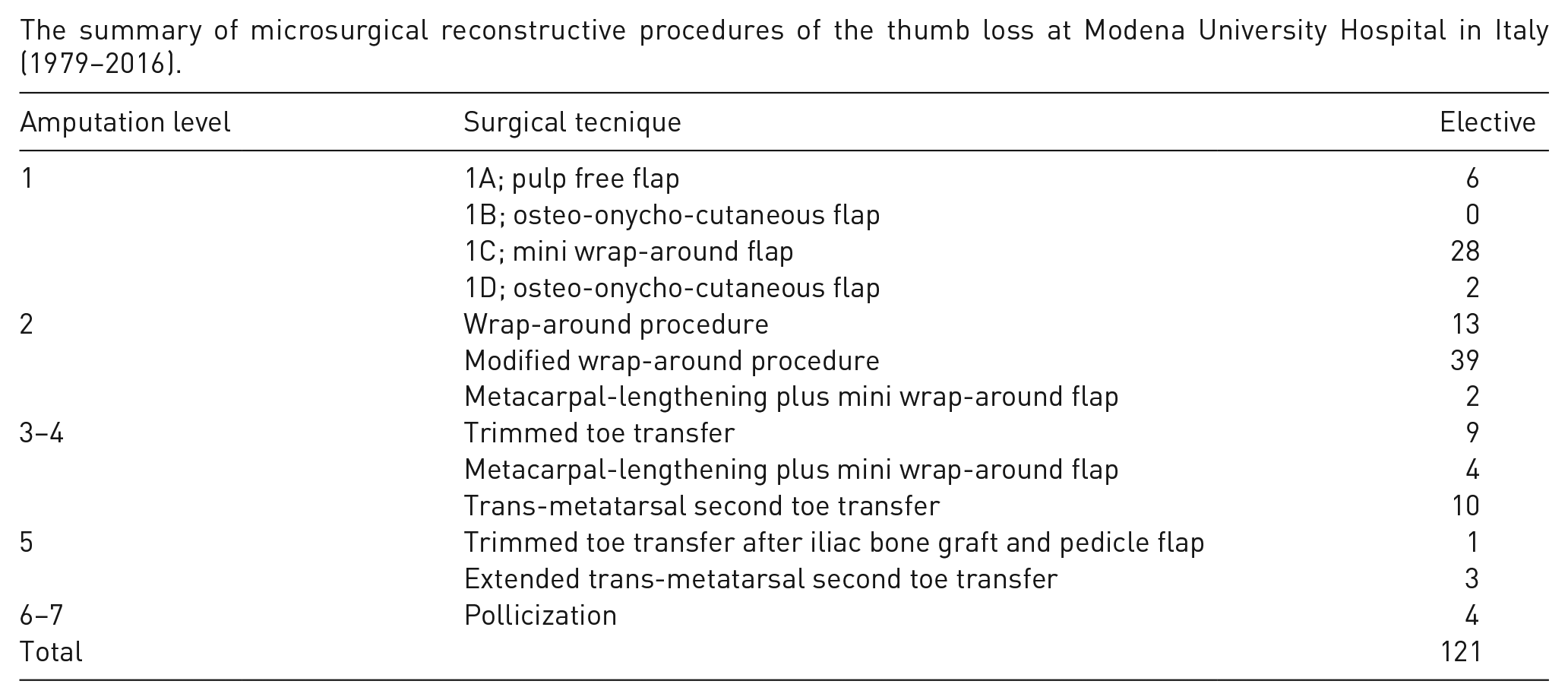
The summary of microsurgical reconstructive procedures of the thumb loss at Modena University Hospital in Italy (1979–2016).
For surgical planning, the patient needs to be evaluated pre-operatively regarding level of amputation, joint mobility, residual tendinous and thenar muscle functions, and overall sensibility. The patient should express a strong desire for reconstruction and be in sufficiently good physical condition to sustain prolonged anaesthesia. In addition, the patient must understand and accept the risks of operative failure, donor-site morbidity, and the functional limitations of the transferred toe.
Patients need to receive Doppler ultrasound to study donor and recipient vessels. Computed tomography angiography is not necessary unless there is a history of previous trauma or there are congenital anomalies in the foot. The skin of the thumb amputation stump needs to be soft and pliable, especially when there is injury to the first web space in order to avoid skin problems. In some patients, before performing a toe transfer, the surgeon needs to harvest a flap (Al-Qattan and Al-Qattan, 2016; Graham et al., 2016; Wei, 1998) to cover the thumb amputation site. The nail of the contralateral normal thumb should be accurately recorded along with the dimensions (length and circumference) of the great toe.
Distal thumb reconstruction
Thumb amputation distal to the IP joint does not cause any functional disability, and this level of amputation does not necessarily require microsurgical reconstruction. Depending on the patient’s lifestyle, customs, and cultural background, there may be a high demand for improved appearance and more refined function. In selected patients with strong motivation, the loss of nail, sensible pulp, or the fine pinch (nail-to-nail pinch) may be indications to transfer part of the distal phalanx of the great toe. This partial great-toe transfer offers a cosmetic reconstruction; moreover, the nail represents a cosmetic as well as a functional advantage (Wei et al., 1996). The cosmetic role of the thumbnail should not be underestimated. Some patients may have a functional reconstructed thumb, but they underuse and hide it if the nail is not present. The functions of the distal phalanx are not completely transferable to the remaining stump of the proximal phalanx. In fact, the terminal phalangeal segment constitutes the most vital part of the thumb: herein lie the pulp, nerve receptors, fingerprinted skin, and the nail (Morrison, 1992).
Many techniques are often similar (Adani et al., 1999; del Piñal et al., 2014; Woo and Seul, 1998; Woo et al., 1999). These methods all use a custom-made osteo-onycho-cutaneous flap. The methods we use are the mini wrap-around flap (Adani et al., 1999, 2005) and the great-toe partial-nail-preserving transfer (Woo and Seul, 1998). We harvest the bone, nail plate, nail matrix, and pulp from the medial aspect of the toe to achieve an appropriate circumference for the reconstructed thumb. A longitudinal osteotomy may be used to reduce the bone, leaving a medial flap of the distal great toe to allow donor site direct closure and ensure a good aesthetic result. The flap is based on the dorsal or plantar vascular system and is dissected along with the dorsal venous network and deep peroneal and digital nerves.
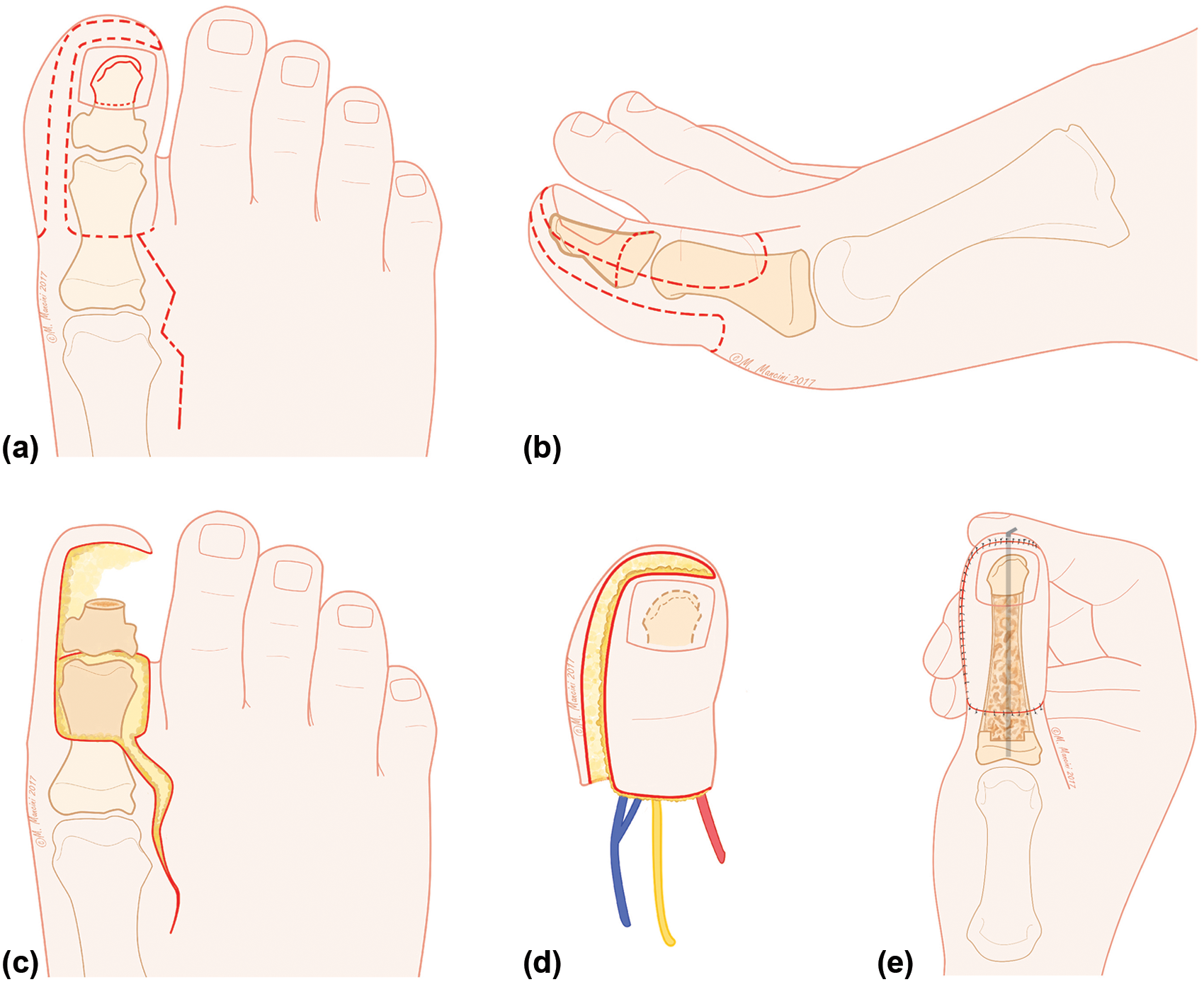
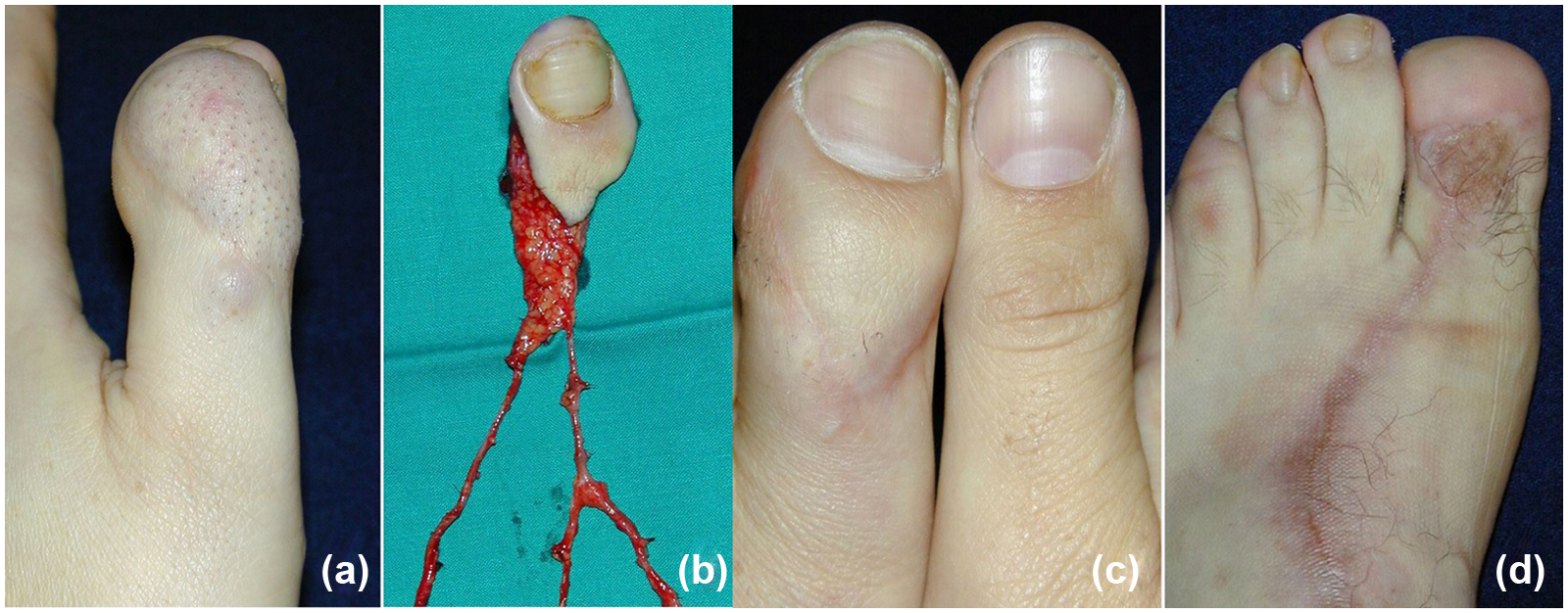
The partial-nail-preserving transfer of the great toe has the advantage of preserving some portions of the great toe’s nail after the flap is harvested (Woo and Seul, 1998). The results obtained with these techniques are good, both functionally and aesthetically; these techniques restore adequate thumb length, good pulp, and an appearance of the nail similar to the contralateral thumb (Figure 7). Kirschner (K)-wires are used for bony fixation. When the IP joint is present, the K-wires are left in situ for 5 to 6 weeks. Their removal is followed by range of motion exercises. When there are no articular structures of the IP joint, the K-wires are left until bony fusion is complete (Figure 8).
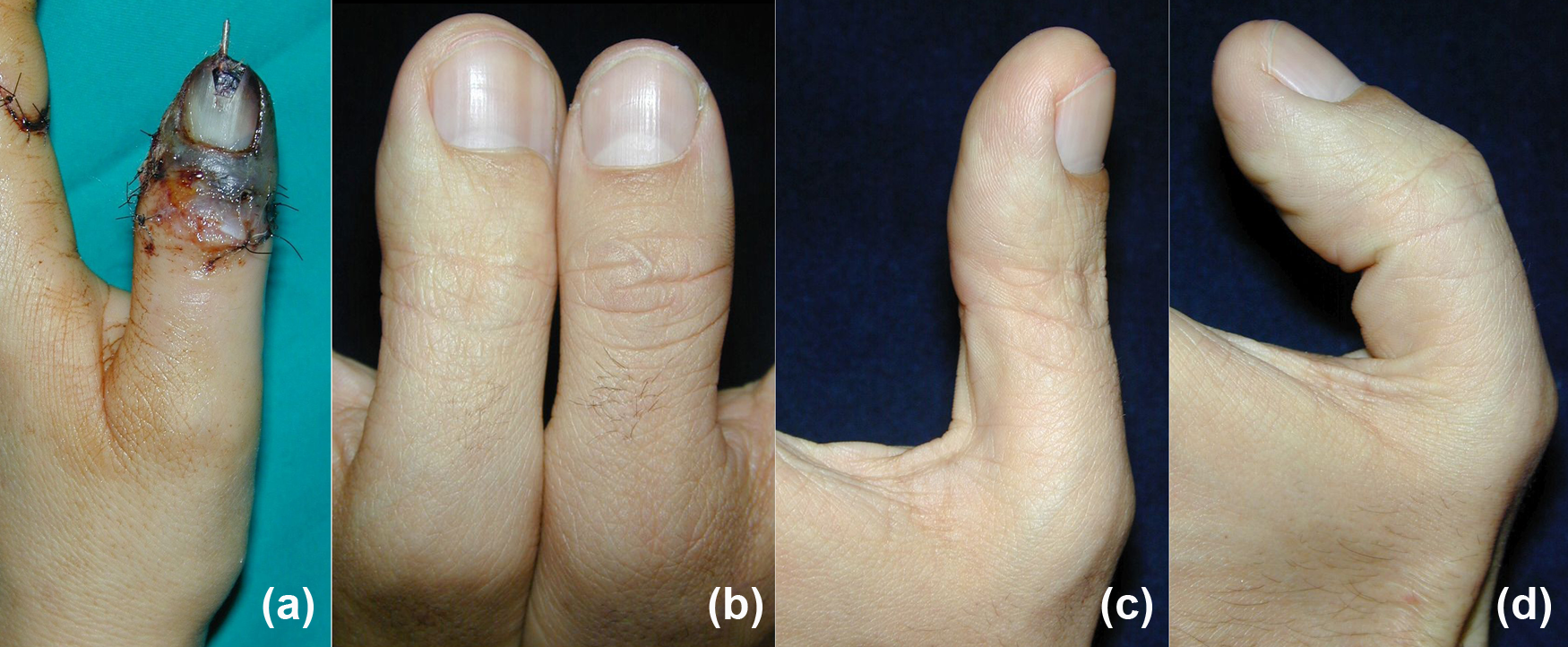
Mini wrap-around flap. (a) Distal thumb necrosis after failed replantation. (b), (c), (d) Thumb reconstruction is achieved by using a mini-wrap around flap (level 1c of Merle classification) preserving the IP joint. Appearance and function of the reconstructed thumb at follow-up.

Mini wrap-around flap plus dorsalis pedis skin flap. (a) A severe circular saw injury resulted in distal thumb necrosis (level 1 amputation), including dorsal skin over the MP joint. (b) Reconstruction employed a separate dorsalis pedis flap in continuity with a mini wrap-around flap. (c) Intraoperative result. Arthrodesis of the IP joint and provisional coverage with Integra Dermal Regeneration Template (Integra Life Sciences, Inc., Plainsboro, NY, USA) of residual dorsal skin defect. (d), (e), (f) Thumb appearance and donor site result at medium term follow-up.
Distal thumb reconstruction with a toe transfer is more for appearance than for function. For this reason, the partial great-toe transfer is harvested by retrograde dissection of a short neurovascular pedicle (Wei et al., 1995) to minimize surgical scar and the time required for the dissection of a lengthy vascular pedicle. Functional and aesthetic sequelae of the donor site should be minimized, and the insertion of the flexor hallucis longus tendon should not be violated (Barca et al., 1995).
Thumb amputation distal to the mid-portion of the proximal phalanx
Amputation proximal to the mid-portion of the proximal phalanx decreases hand span, which affects both pinch dexterity and large object grasp. The wrap-around technique (Morrison et al., 1980) is ideal for this situation. Their original procedure includes skin, nail, and pulp from the big toe, together with an iliac bone graft. The main advantages of this flap are its well-matched size in relation to the normal contralateral thumb and reduced donor-site morbidity. The most common complications are donor site morbidity and bone graft absorption (Steichen, 1991). Morrison et al. (1984) modified their original method by harvesting the flap together with a bone fragment distal to the distal phalanx. In this way, the bone graft harvested from the iliac crest is placed between two vascularized fragments to reduce risk of absorption and of fractures. The wrap-around flap is also ideal for degloving injuries of the thumb (Adani et al., 1998; Morrison, 1992) (Figure 9).
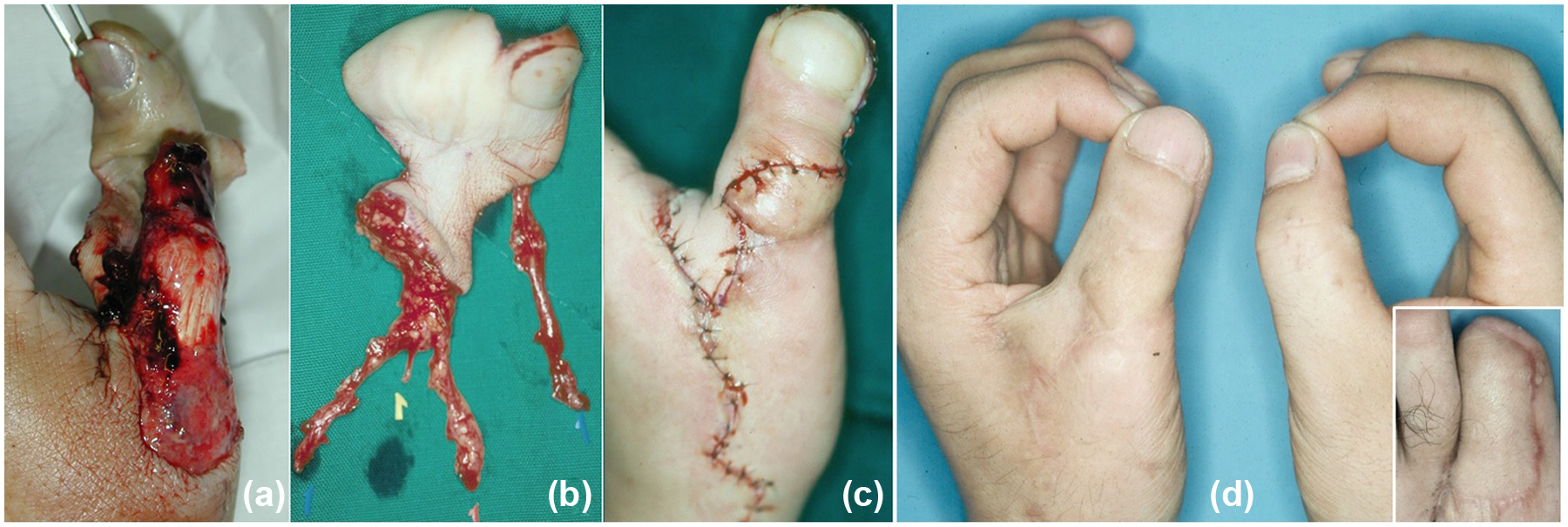
Wrap-around flap transfer. (a) Avulsion amputation. Replantation was not possible due to the avulsed vessels distally. (b) The wrap-around flap was harvested. (c) After the flap inset into the thumb defect. Notice the additional skin harvested from the first web space in the foot to prevent contracture of the web space in the hand. (d) Functional and cosmetic result compared with the contralateral thumb. Insert: donor site coverage.
The wrap-around flap, however, is not useful for thumb reconstruction in children because it does not offer any potential for growth (Morrison, 1992; Nikkhah et al., 2016). The drawbacks of this approach are that the reconstructed thumb has a limited range of motion, resorption of the bone graft may occur (Lee et al., 2000), and the donor site requires a cross-toe flap for closure (Hamilton et al., 1979).
Among the various techniques for great-toe transfers, the wrap-around procedure has had the highest complication rate, perhaps due to the complex nature of flaps used to preserve the ray of the great toe or insufficient soft tissue to cover the IP joint (Pan et al., 2011; Sosin et al., 2016). Furthermore, Barca et al. (1995) reported that patients with the wrap-around flap had an overload, sometimes asymptomatic, of the remaining metatarsal heads (usually the second and third).
Chinese surgeons (Pan et al., 2011; Shen et al., 2016) suggested a new modification of the wrap-around flap that preserves a plantar triangular flap of the great toe. They achieved an excellent contour and functional outcome of the new thumb (Figure 10) and reduced donor-site morbidity. The whole great toe can be transferred when the difference in nail width between the thumb and the great toe is less than 3 mm, in patients whose great toe is similar in size to the thumb (Figure 11).
Modified wrap-around flap. (a) Thumb amputation (level 2 amputation). (b) The toe flap includes the entire nail and dorsal skin preserving a plantar strip extending around the toe tip. (c) The grafted bone is placed between the distal phalanx of the great toe and the remaining base of the first phalanx. (d) Intraoperative result. (e), (f) Final result.
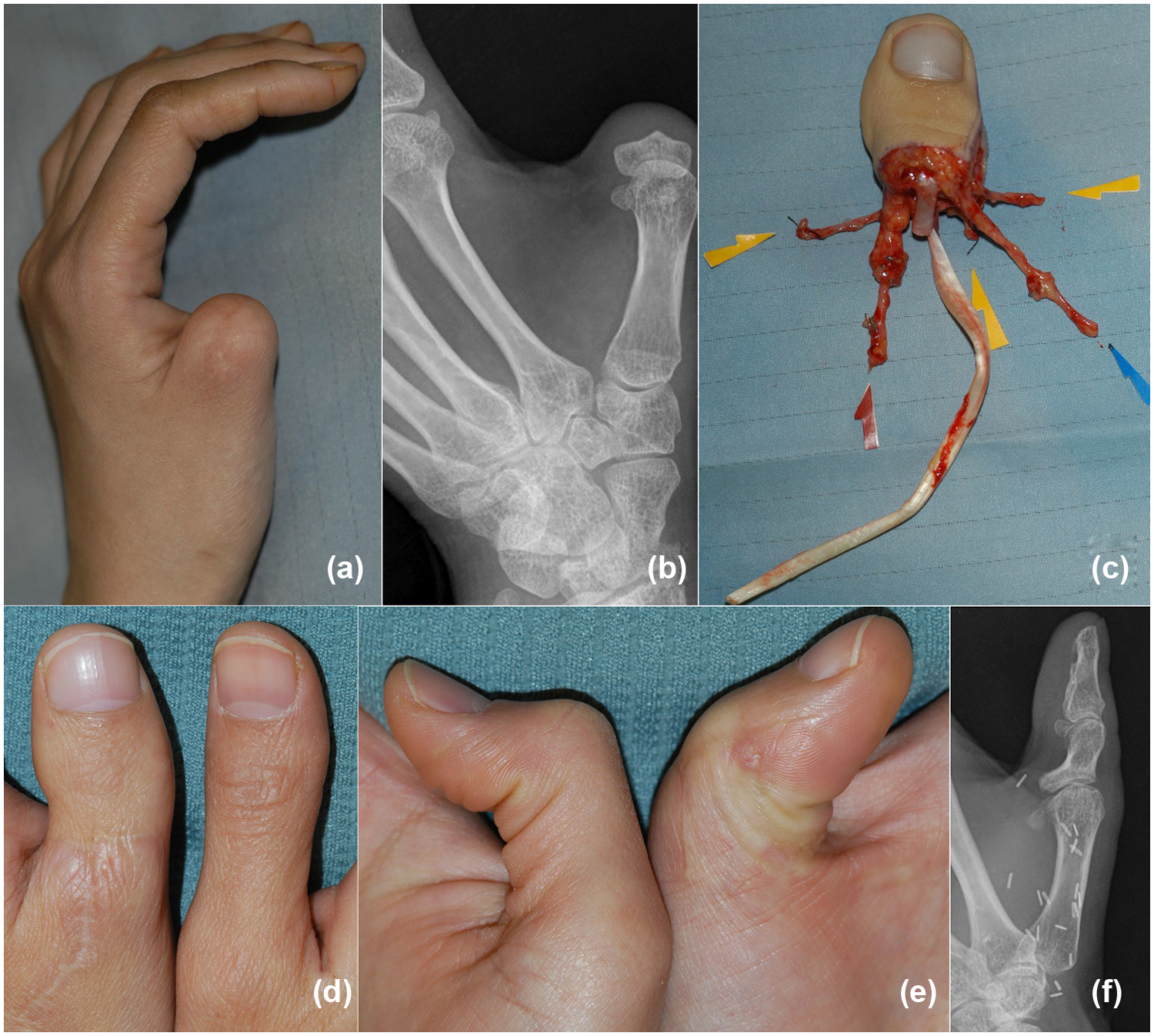
Whole great toe-to-thumb transfer. (a), (b) Previous amputation of the thumb at the base of the proximal phalanx (level 2 amputation). (c) The whole great toe is harvested with a long flexor pollicis longus tendon from the wrist. (d), (e), (f) Clinical and radiographic results.
The Trimmed great-toe transfer by Wei et al. (1988) and Upton and Mutimer (1988) reduced both the bony and soft tissues on the medial aspect of the great toe to create a more natural looking thumb. They achieved this by performing a longitudinal osteotomy on the medial aspect of the distal and proximal phalanges. The periosteum and medial collateral ligament of the IP joint of the great toe are harvested, as well as the proximally based flap. A simple repair of the periosteum, medial collateral ligament, and joint capsule can achieve the stability of the IP joint (Figure 12). In exchange for a better appearance, there is some loss of motion in the IP joint. The proximal remaining strip of the medial skin flap can be used to help close the donor defect, which is often quite tight. These modified procedures offer the aesthetic advantages of wrap-around flaps, while avoiding bone graft resorption and pulp mobility. To minimize the complications, at least 1 to 1.5 cm of the proximal phalanx in the great toe should be preserved.
Surgical technique of a trimmed great toe. (a) Elevation of the medial skin flap. (b) Periosteum and medial collateral ligament of the IP joint are raised. (c) Longitudinal osteotomy is performed with an oscillating saw. (d) Repair of the joint flap. (e) Final aspect of the trimmed great toe before in-setting into the hand.
Modified twisted-toe flap techniques are also available for reconstruction (Foucher et al., 1980; Iglesias et al., 1995; Tsai and Aziz, 1991). These techniques combine the wrap-around flap technique with the vascularized joint transfer or neurovascular cutaneous flap and osteo-tendinous flap based on the single vascular pedicle. These procedures restore a more normal looking thumb, while preserving the epiphyses for future growth with reduced donor site morbidity. The modified twisted-toe technique by Kempny et al. (2013) reconstructs a very natural appearing thumb with good stability and strength, together with a ‘new great toe’ for the donor foot. To maintain an intact skeleton of the great toe, Zhang et al. (2016) suggested reconstructing a thumb amputated at the proximal phalanx with an iliac bone graft plus a dorsal toenail flap to repair the dorsal defect and a dorsalis pedis flap to resurface the palmar defect. Despite the many advantages, however, these techniques are not popular among surgeons, because their procedures are more complicated and time-consuming than single-toe harvesting procedures.
Thumb amputation at the MP joint
Reconstruction for thumb amputations at the MP joint level is more complex. If the metacarpal head is intact, the whole great toe with its metatarso-phalangeal ligaments can be transferred, which may restore function of the thumb MP joint (Buncke and Valauri, 1988; Buncke et al., 2007). Its major drawback is that the great toe size is approximately 20% larger than the thumb in all dimensions and is sometimes extremely bulky. Debulking appears necessary because the great toe, once transferred, naturally reduces its size and becomes more thumb-like in appearance (Valauri and Buncke, 1989). The great-toe transfer includes tendons, bones, joints, and innervated skin that, in many instances, restore the attributes of the lost thumb: ‘great toes make great thumbs’ (Buncke and Valauri, 1988).
However, many patients do not accept the harvesting of the entire great toe because of an unbalanced and unacceptable appearance of the donor foot, especially if part of the metatarsal head is also transferred. This may also alter foot function.
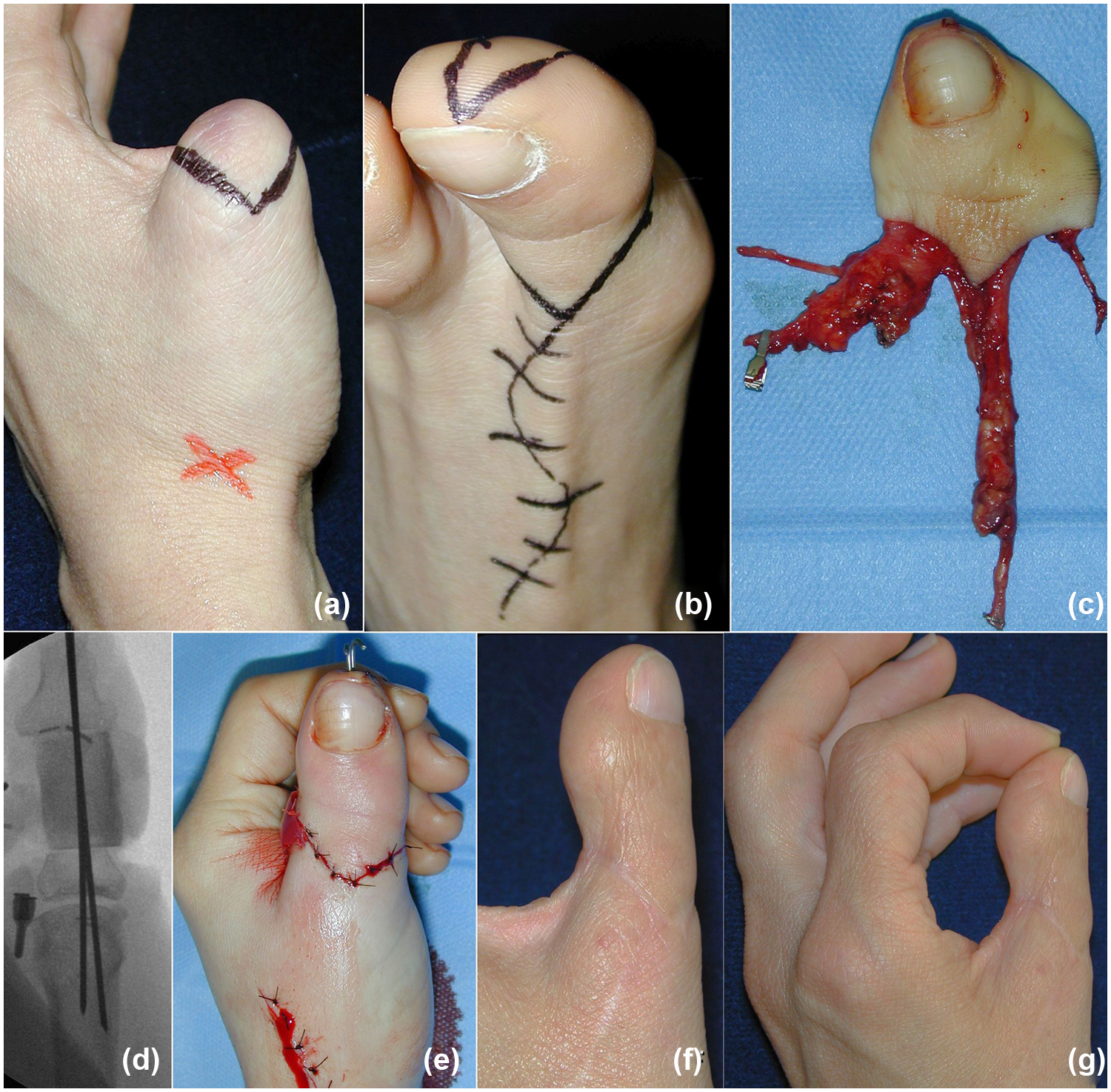
The trimmed toe technique (Wei et al., 1988, 1994) combines the best parts of the total toe transfer and wrap-around procedures. MP joint arthrodesis is frequently performed to ensure stability and pinch to the new thumb. Preservation of 1 cm of the proximal phalanx improves the appearance and push-off of the donor foot (Wei et al., 1994). The residual medial great-toe skin flap is employed to cover the first metatarsal head with an acceptable donor site result. Secondary aesthetic revision techniques include pulp-plasty and bony contouring (Wallace and Wei, 2010; Wei et al., 1996) (Figure 13). The donor sites of great toe and trimmed great-toe transfers are aesthetically unpleasing and are frequently unacceptable for the patient.

Trimmed great toe. (a) Thumb amputation through the MP joint (level 3 amputation). (b), (c), (d) Final functional result with arthrodesis of the MP joint. (e) Donor site result. (f) Aesthetic revision at 1-year follow-up with Wei pulp-plasty.
To solve this problem, we combined two surgical procedures, metacarpal lengthening and mini wrap-around flap from the great toe, to improve the donor site appearance while maintaining the same aesthetic results for the thumb (Adani et al., 2013). Our method uses the Matev technique (Heitmann and Levin, 2002) to lengthen the stump with a lengthening device (Orthofix M-100, Orthofix srl, Verona, Italy). A longitudinal dorsoradial incision is made over the metacarpal and pairs of 2.5 mm pins are inserted. The osteotomy is done subperiosteally and fixed with K-wires. The osteotomy is distracted 0.5 cm to ensure proper movement of the bone fragments and then closed leaving a bone gap of about 0.2–0.3 cm. The average distraction is 0.5 mm per day or every other day, depending on patient’s discomfort. Distraction is continued for an average of 2 months. To achieve bone consolidation, the fixator is left in place for an average of 4 months. After a suitable length is obtained, the mini wrap-around flap is performed to replace the missing nail and pulp tissue (Figure 14). This procedure does not need an iliac bone graft and avoids problems of fracture and bony absorption. Disadvantages include longer overall treatment time and no restoration of MP or IP joint motion. The CMC joint of the thumb is therefore responsible for all the movements of the reconstructed thumb.
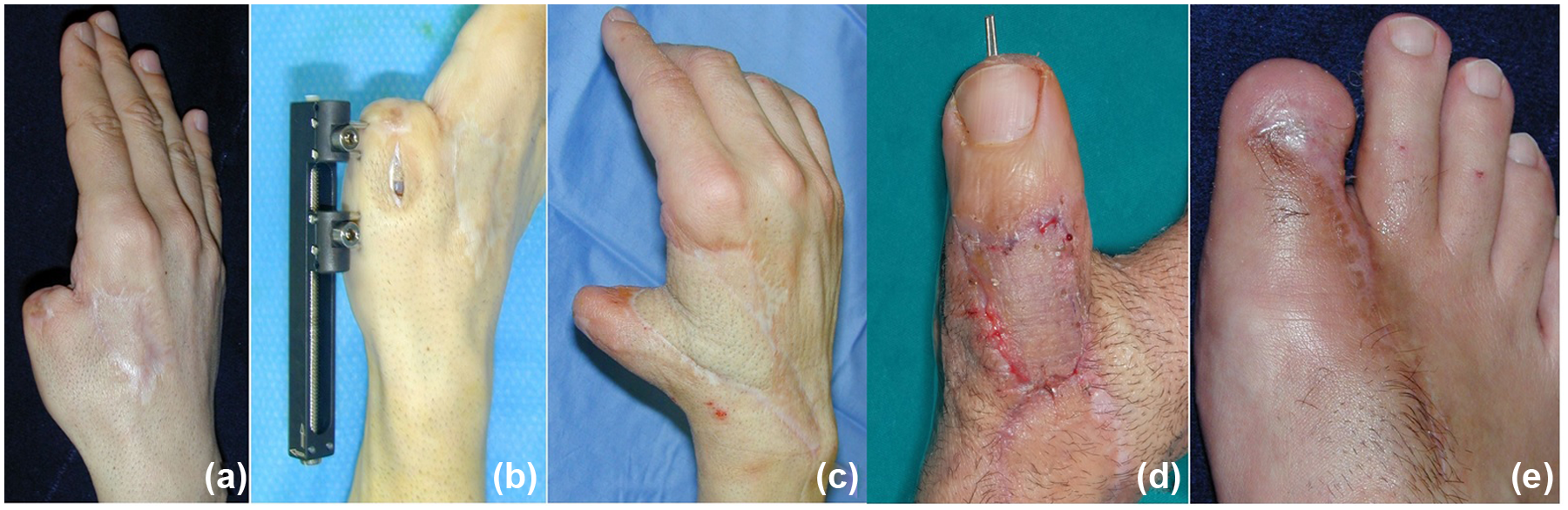
Metacarpal lengthening plus mini wrap-around flap. (a) The thumb amputation through the MP joint (level 3 amputation) with severe retraction of the first web space. (b) Distraction callotasis was applied with a lengthener (Orthofix). (c) The first web space was opened with a posterior interosseous flap. Three months after the initial surgical procedure, a mini wrap-around was transferred for distal thumb reconstruction. (d), (e) Aspect of the new thumb and the donor site result 1 month after the microsurgical procedure.
Thumb amputation through the metacarpal
A thumb amputation through the metacarpal can be reconstructed with a trans-metatarsal transfer of the great toe or second toe. The range of motion in the metatarsophalangeal (MTP) joint of the great toe and second toe is mainly extension. This should be corrected by an angled osteotomy of the metatarsal head, followed by a shortening of the plantar plate, with conversion of hyperextension of the MTP joint to flexion of the joint (Figure 15). We do not recommend the trans-metatarsal transfer of the great toe. In case of disarticulation at the MCP joint, the sacrifice of the MTP joint causes major donor site morbidity (Barca et al., 1995). Preservation of the entire length of the first metatarsal is just as important as the reconstruction of the thumb.
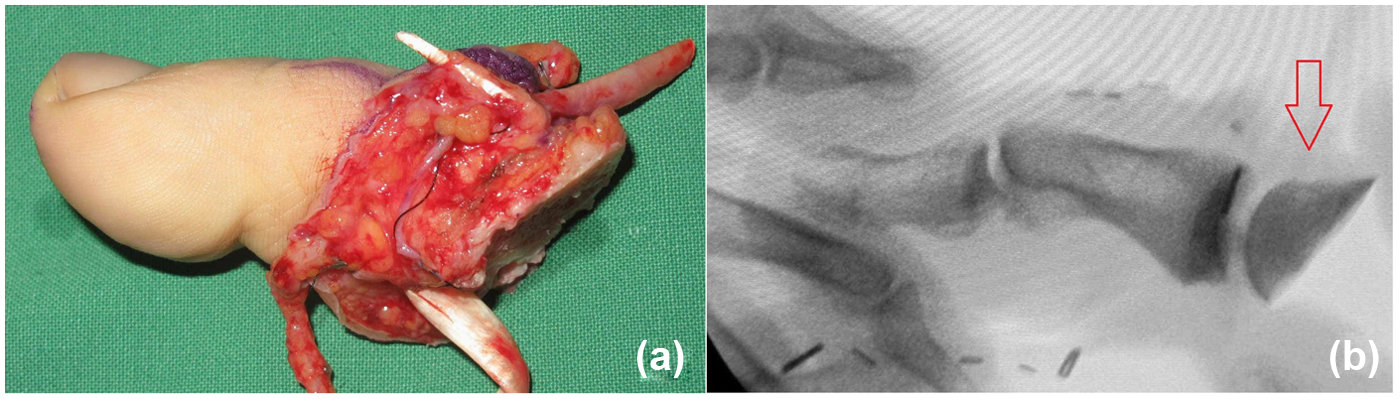
Surgical technique of extended great-toe transfer. (a) Oblique osteotomy at metatarsal head of the great toe converts hyperextension of the MTP joint into flexion of this joint. (b) The direction of osteotomy in X-ray films (arrow).
Amputation through the shaft of the metacarpal can be reconstructed in a two-stage procedure. The first stage harvests a tricortical iliac bone graft to lengthen the metacarpal along with soft tissue coverage with a groin flap or a reversed posterior interosseous island flap (Wei, 1998). Three to 6 months later, a trans-metatarsal second-toe transfer provides some motion for the new thumb’s MCP joint. When the patient desires to preserve the MTP joint of the great toe, the great-toe transfer can be harvested at the level of the proximal phalanx. In this case, the new thumb presents only two joints without an MCP joint. When opting for the most suitable surgical procedure, the patient’s aesthetic and functional expectations for the new thumb, as well as morbidity and appearance of the donor sites, should be carefully considered.
Selection of the trans-metatarsal second toe transfer is mostly dependent on personal or cultural preferences, although post-operative appearance and strength is not as satisfactory as with a great-toe transfer (Graham et al., 2016). However, this is our favoured technique for this level of amputation.
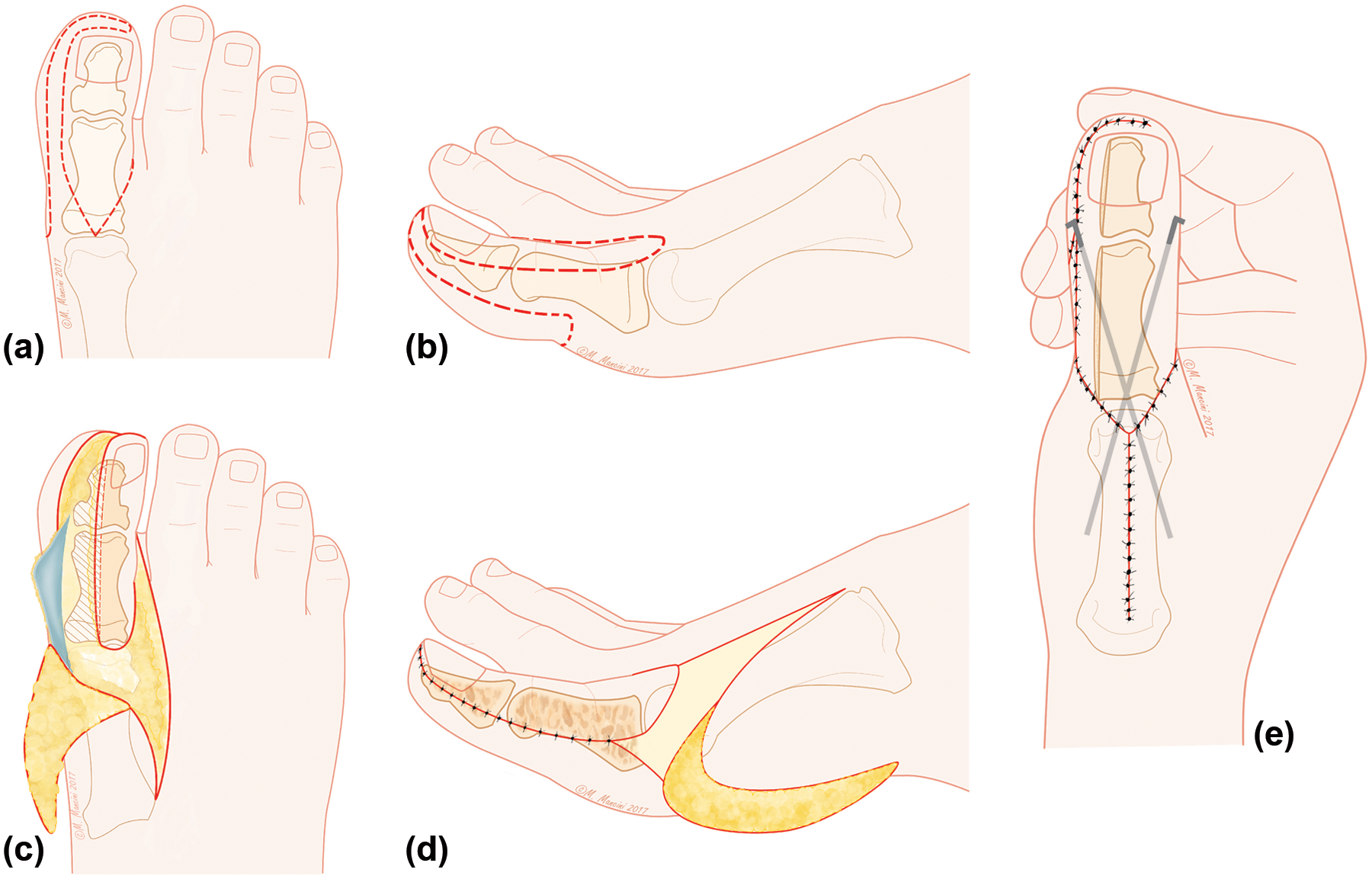
In complex defects of the thumb or with unstable soft tissue around the thenar area, a preliminary flap is necessary to provide redundant soft tissue. A combined dorsalis pedis flap with trans-metatarsal second-toe transfer is also an option when opting for a single-staged reconstruction. When the second toe is harvested, a V-shaped incision is made on both the dorsal and plantar aspects of the foot (Figure 16). This provides adequate skin coverage for both donor and recipient sites. In case of insufficient soft tissue coverage, the metatarsal bone should be harvested with the interosseous muscle. A skin graft is always necessary to cover the metatarsal. Regarding donor site closure, the intermetatarsal ligaments between the first and third toe should be repaired. In the second-toe-to-thumb transfer, a modified technique reduces donor site morbidity while providing an improved appearance of the new thumb (Zhao et al., 2010). This technique includes the harvesting of a flap from the lateral side of the great toe and inserting it into the volar aspect of the second toe to give more bulk. Skin excisions are then performed on each side of the tip to reduce the bulbous appearance. An eponichial flap increases the apparent lengthening of the nail (del Piñal et al., 2007).
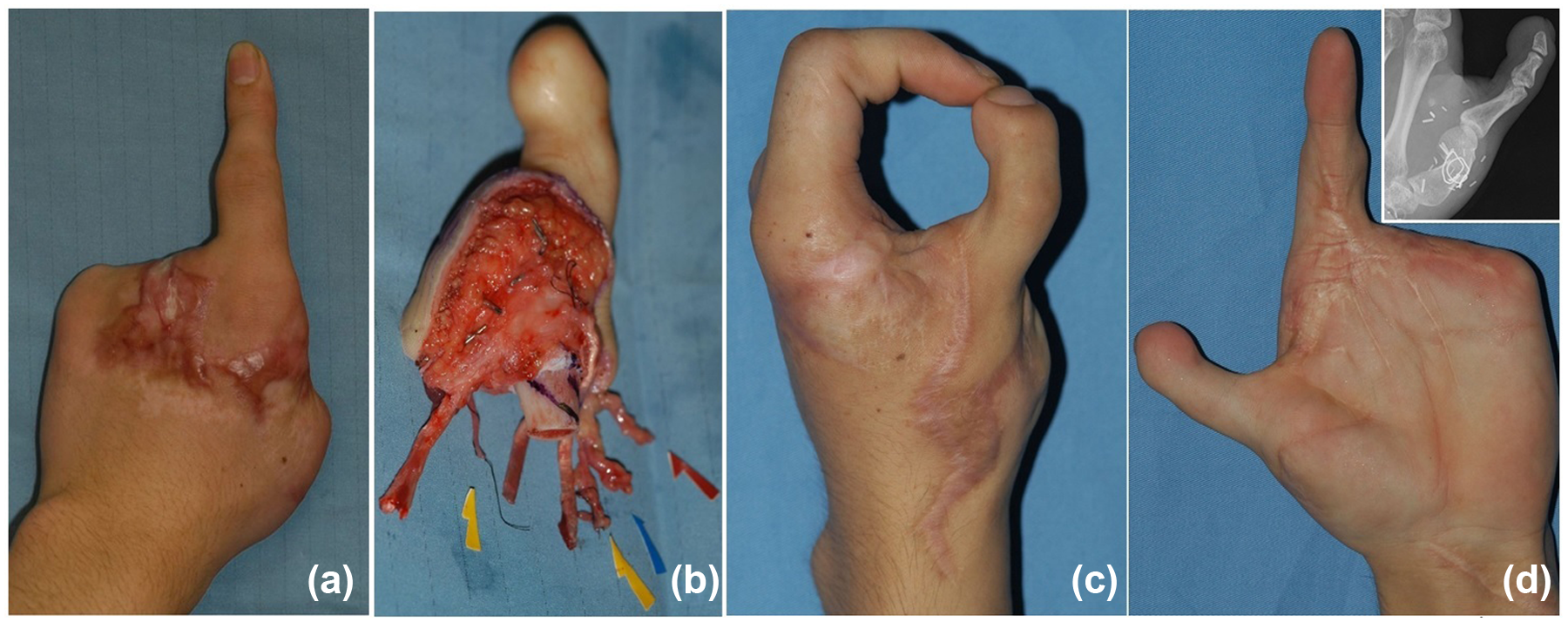
Whole second toe-to-thumb transfer. (a) Crush amputation of the hand except the index finger. The thumb was amputated at the metacarpal neck (level 4 amputation). (b) As the patient refused trans-metatarsal transfer of the great toe, ipsilateral second toe transfer was employed. (c) Thumb to index pinch after surgery. (d) Thumb extension. Insert: radiographic results.
When the thenar muscles are not well preserved, the reconstructed thumb may not achieve satisfactory opposition. Osteosynthesis with 30° to 60° pronation of the proximal phalangeal base of the transferred toe to the first metacarpal stump is the traditional method for restoring opposition. Primary opponensplasty in toe transfers provides active opposition and a greatly improved tripod pinch in comparison with static opposition with osteosynthesis (Lin et al., 2012). The flexor digitorum superficialis tendon from the middle or ring finger can be used as donor, with its pivot point at the insertion of the flexor carpi ulnaris and using a loop of this tendon as a pulley.
Amputation of the thumb through the proximal portion of the metacarpal or through the CMC joint is very disabling. Pollicization is the most promising method of reconstruction (Al-Qattan, 2016). The presence of thenar muscle function is critical to obtain satisfactory results in pollicization (Ishida et al., 2006).
Dorsal skin
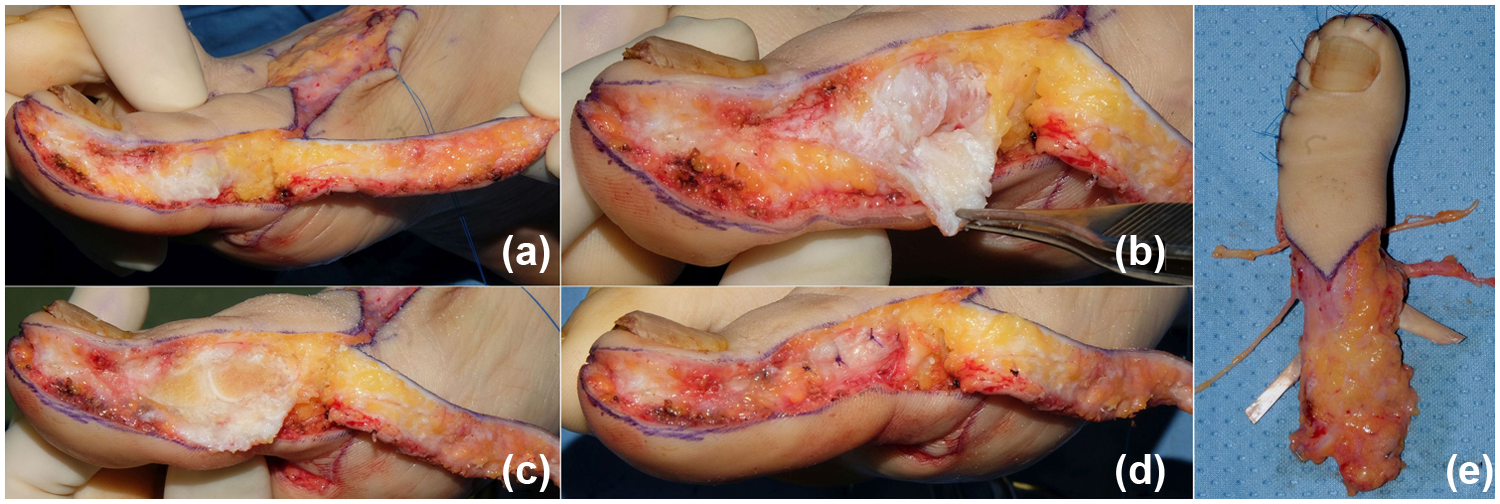
Covering dorsal thumb defects with an intact volar surface can be a challenging issue, particularly when multiple tissues are involved simultaneously. A custom-made free composite flap harvested from the dorsum of the foot represents a good aesthetic procedure. The technique is based on the classical partial toe transfer technique (Foucher et al., 1991; Woo et al., 1999). The defect area in the recipient site is outlined; the nail complex, including nail bed, hyponychium, lateral folds, nail matrix, and adjacent skin, is harvested including the dorsal skin. The distal three-quarters of the toe phalanx is harvested in the cases requiring bone reconstruction. Osteotomy of the toe distal phalanx may be performed to reduce its bulk. This reconstruction is a one-stage technique that maintains thumb length and provides vascularized bone and nail. The cosmetic result is satisfactory because the quality of the skin and nail on the dorsum of the great toe is similar to the natural thumb (Figure 17).
Custom free vascularized partial toe transfer. (a) Dorsal thumb defect covered with unpleasant abdominal flap. (b) Osteo-onycho-cutaneous flap harvested from the dorsum of great toe. (c), (d) Aesthetic result compared with the contralateral thumb along with the donor site result.
Role of emergency reconstruction
Emergency toe-to-hand transfer combines immediate flap coverage of the tissue defect with thumb reconstruction when replantation of the amputated thumb is impossible or has failed. One of the authors (S.H.W.) performed emergency transfers in 142 (58%) out of the 246 patients with toe-to-thumb transfers. Woo et al. (2004) consider many advantages of such emergency transfer over the elective procedures, including single-stage reconstruction, shortened convalescence, early return to work, and socioeconomic efficiency. Yim et al. (2004) and Woo et al. (2006) reported no noteworthy difference in the success rates, frequency of complications, or ultimate functional results of the emergency toe-to-thumb transfer versus elective surgeries. However, the economic and therapeutic advantages should be weighed against the risks associated with this approach (Ray et al., 2009). An immediate great toe-to-thumb transfer is also an option when thumb amputation is required to satisfy adequate oncologic margins (Kovachevich et al., 2016).
A major disadvantage of emergency toe transfer is the lack of personal relationship between the patient and the surgeon, whereas the duration of difficulty and discomfort in performing daily activities of those patients with an amputated thumb is limited in an emergency reconstruction. Also, the patient’s subjective satisfaction with the post-operative function and appearance might decrease because emergency reconstruction does not allow the patient, who is comforted by the sight of a reconstructed hand, to mourn the loss of their digits before the toe transfer. In addition, surgeons should have a higher level of expertise of microsurgery; we suggest that surgeons should be at least level 3 expertise (Tang, 2009; Tang and Giddins, 2016). Post-operative infections and flap failure can occur if the contaminated wound or traumatized tissue are not completely and thoroughly debrided. Therefore debridement should be aggressive, resembling the resection of suspected tissue in cancer extirpation. Before making the final decision on emergency toe transfer, the patients should be informed and fully understand the entire procedure and the most probable post-operative functional results.
Complications of toe-to-thumb transfer
The most disastrous complication of a toe-to-thumb transfer is flap failure. The incidence of flap failure was reported in 0% to 7% of overall cases (Buncke et al., 1991; Graham et al., 2016; Gu et al., 1993). Recently, Lin et al. (2015) demonstrated that the overall success rate of toe-to-hand transfer in 363 cases was 98%. Consequently, the diameter or anatomical location of the first dorsal metatarsal artery is no longer the main causative factor of the circulatory crisis resulting in flap failure. Such situations are reversible and can be solved by careful pre-operative assessment, using refined microsurgical suture techniques, and retrograde dissection of the first dorsal metatarsal artery (Spanio et al., 2005, Wei et al., 1995). Iatrogenic trauma of the vessel during dissection or drilling may cause vessel spasm or late thrombosis. Wound infection induces an inflammatory response and the release of inflammatory mediators that can damage blood vessels and result in vasospasm or the formation of thrombi. Previous injury and surgical procedures cause tissue fibrosis and adhesions. Post-operative wound infection is associated with an increased risk of re-exploration (Lin et al., 2015).
Operative failure is mainly due to failure to recognize and appropriately treat vascular compromise. Re-exploration should be carried out whenever vascular insufficiency is suspected or does not improve after bedside management. Most vascular compromise is caused by arterial insufficiency within 72 hours following surgery. During re-exploration, transfer of vascular structures from the adjacent finger may be an alternative means of creating a fresh recipient for arterial and venous structures rather than insisting on the revision of the previous recipient vessels (Ozkan et al., 2006). To prevent vascular complications of the toe-to-hand transfer, meticulous dissection and ligation of the branch vessels, complete anastomosis of the vessels, and post-operative intensive monitoring of the transferred toe are mandatory.
Donor site complications are categorized as wound dehiscence, infection, necrosis, scarring or callosity, and pain or discomfort. The complications and donor site morbidity have historically been underestimated. Sosin et al. (2016) showed that the overall rate of donor site complications after toe-to-hand transfer was 22% in great-toe transfers and 15% in second-toe transfers. Transfer of the great toe alters the biomechanics of weight distribution and gait. Great-toe transfer appears to have a higher morbidity rate, but a lower re-operation incidence when compared with second-toe transfer. With second-toe transfers, almost no patients complain about the donor site morbidity.
Rehabilitation and authors’ outcomes
The goals of rehabilitation are to increase the range of motion, facilitate sensory restoration, and improve the coordination and dexterity of the reconstructed hand. An aggressive rehabilitation programme is likely to decrease the incidence and number of secondary procedures for tendon adhesions or joint stiffness. Exercise programmes should avoid deterioration of wound condition, bone fixation, or tendon suture.
Our rehabilitation protocol consists of fabricating a custom-made forearm-based dorso-radial protective thumb orthosis 5 to 7 days post-operatively. The wrist is immobilized in neutral and the thumb is abducted (with no tension on the repaired structures). The MP and IP joints are slightly flexed about 15° if both flexor and extensor tendons are involved. This position favours the repaired flexor tendon because of its higher incidence of repair failure, and subsequent surgical exploration would be more complicated. Protected gentle active motion starts 5 to 7 days and no later than 14 days post-operatively. The motion starts at the wrist and thumb CMC joint with gradual and gentle passive and active motion of the MP and IP joints within 4 weeks post-operatively. Exercises are always carried out in a painless manner and avoiding excessive tension on repaired tendons, blood vessels, and nerves. After 6 weeks, neuromuscular electrical stimulation, blocking, and selective joint exercises are employed. After 2 months, light resisted and dynamic orthotic management are introduced and progressed according to bone consolidation and pain tolerance. Also, our rehabilitation team starts sensory re-integration using graded motor imagery, laterality recognition, and mirror therapy as early as the second therapy session to minimize long-term loss of function due to central and peripheral nerve system inactivity.
Ma et al. (1996) suggested a five-stage aggressive motor and sensory rehabilitation programme. During the first 3 days, oedema control and prevention of joint stiffness are important. On the fourth day, gentle passive and assisted active exercise of the farthest joint from the bone fixation should begin, keeping the wrist in a neutral position inside the splint. After 1 to 2 weeks, the wrist is moved through its full range, while keeping other joints immobilized. The patient is permitted to walk on the heel of the donor foot. From the third week, the joints near the bone fixation site should be moved as much as possible. Gentle active exercise is then added, and a dynamic splint is used to increase the range of motion while not jeopardizing bone healing. After the stitches are removed, scar massage and compression taping can begin. In the fifth to sixth week, when the tendons are healed, blocking flexion and extension exercises are initiated. Rehabilitation then aims at simulating daily and vocational activities.
Early sensory re-education after toe-to-thumb transfer intends to facilitate the perception of touch sub-modalities and correct mislocalization. Training is initiated when the patient can perceive 30-cps vibrations from a tuning fork with the reconstructed thumb pulp. A late phase sensory re-education focuses on size and shape discrimination and on object identification. The late phase sensory re-education is differentiation of objects by texture, size, and shape. Aggressive delayed sensory re-education can improve two-point discrimination of the tip (Wei and Ma, 1995). Buncke et al. (1991) reported rather disappointing sensory and motor function after great toe-to-thumb transfer with one or more of the following: static two-point discrimination over 15 mm, pinch strength less than 5 pounds, IP joint motion less than 15°, or first web space contracture.
Our preferred choices for reconstruction of thumbs at various levels of amputation are summarized in Table 1. We stress that surgeons should attempt to minimize donor site morbidity. The indication of toe transfer is strictly confined to the most eligible candidates. Dissection of the vascular pedicle should be atraumatic to avoid recalcitrant vasospasm. Post-operatively, in instances of suspected vascular compromise, early re-exploration in the operation room should be performed. As with replantation surgery, firm bone fixation, strong tendon repair, and meticulous nerve repair facilitate early post-operative rehabilitation and better recovery. Secondary procedures, including pulp-plasty, scar revision, or tenolysis, results in better improvement of the function and appearance.
Between 1979 and 2016 and at two hospitals, we reconstructed 367 amputated thumbs with various methods of toe-to-thumb transfer (Table 1). The success incidence of elective and emergency operations was 98% (102 out of 104 cases) and 98% (139 of 142 cases) in the patients of Korea (S.H.W.), respectively. The success rate in of the patients of Italy (R.A.) of elective cases (no cases in emergency were performed) was 93% (112 out of 121 cases). The incidence of re-exploration caused by vascular insufficiency or hematoma formation within 5 days was 10% (37 out of 367 cases). The outcomes of these procedures have been reported in our previous original reports (Adani et al., 1999, 2005, 2013; Woo et al., 1999, 2004, 2006). Our experience confirmed, as reported (Chung and Wei, 2000; Graham et al., 2016), that thumb amputation results in substantial impact on quality of life, ability to work, and psychosocial functioning. Pinch and grip strength were restored up to 70%–75% of the contralateral hand. Static two-point discrimination returned to 10 mm. No major differences were noted regarding survival, grip strength, pinch strength, and recovery of the sensibility considering the different techniques employed. Patient satisfaction with the donor and recipient site was high, and the majority of patients returned to their pre-injury occupations.
Footnotes
Acknowledgements
The authors thank Dr Landi Antonio for permission to include the cases he performed in the Hand Surgery Department in Modena, Italy. We thank Marisa Mancini for the illustrations for this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.