
Abstract
The purpose of this study was to evaluate the time to diagnosis and management of hook of hamate fractures in an era of advanced imaging. We performed a retrospective study of 51 patients treated for hook of hamate fractures. Patients were sent a quickDASH questionnaire regarding the outcomes of their treatment. Hook of hamate fractures were diagnosed with advanced imaging at a median of 27 days. Clinical findings of hook of hamate tenderness had better sensitivity than carpal tunnel-view radiographs. Nonunion occurred in 24% of patients with non-operative treatment and did not occur in the operative group. Both treatment groups achieved good clinical results, with a grip strength of 80% compared with the non-injured hand and a median quickDASH score of 2. Advanced imaging improved the time to diagnosis and treatment compared to historical case series. Nonunion is common in patients treated non-operatively.
Introduction
Fractures of the hook of the hamate comprise 2–4% of all carpal fractures (Geissler, 2001). Hook fractures can result from a direct blow to the hook and its aetiology has been associated with batting sports (Bishop and Beckenbaugh, 1988). Diagnosis of a hook of hamate fracture is often missed at the first patient–clinician encounter (Stark et al., 1989; Walsh and Bishop, 2000). Common signs of hook of hamate fracture are pain in the palm aggravated by grasp, pain with deep palpation over the hook, pain with dorsoulnar deviation and painful flexion of the ring and small fingers caused by tendinitis of the finger flexors (Wright et al., 2010). Plain radiographs have low sensitivity and specificity for diagnosing these fractures (Scheufler et al., 2005).
Treatment of hook of hamate fractures is a matter of controversy. Many clinicians believe casting is likely to result in nonunion and therefore advocate surgical treatment for all patients (Scheufler et al., 2005). However, casting is still a common practice, especially for non-displaced fractures (Whalen et al., 1992). The most common surgical treatment is hook excision, but reduction and screw fixation has been reported to have comparable clinical results (Scheufler et al., 2005; Walsh and Bishop, 2000).
There are few articles examining the diagnosis of this fracture; present knowledge of outcomes of patients with hook of hamate fractures comes from two previously published reports (Bishop and Beckenbaugh, 1988; Stark et al., 1989). The purpose of this study was to evaluate the average time to diagnosis of this injury in an era of routine CT and MRI and to determine the patient-reported outcomes for operative and non-operative treatment of hook of hamate fractures.
Methods
Study population and design
The study is a retrospective case series of patients who were treated in our institution for hook of hamate fractures between 1998 to 2015.
After approval of our institutional review board, a dataset of patients with hook of hamate fractures was created with ACE software (Advanced Cohort Explorer, Rochester, MN, USA). The terms searched were ‘hook of hamate’ and ‘hamate hook fracture’ appearing in various combinations in the patient’s note; diagnosis of hamate fracture (ICD-9 code 814.08); and patients undergoing carpectomy (code 25210) or open treatment of carpal bone (code 25645) with ‘hamate’ in the note. These broad search terms yielded 541 patients, of whom 51were confirmed to have hook of hamate fractures according to chart and imaging review.
These 51 patients’ medical records were reviewed for demographics, hand dominance, injury mechanism and associated injuries. We recorded signs and symptoms at the time of first presentation, radiographic modalities employed and their yield, and the time elapsed between injury and diagnosis. Outcome measures assessed from charts included complications, fracture nonunion, pain, and wrist and fingers’ range of motion (ROM) and grip compared to the non-injured hand at latest follow-up. Since assessment of the patient was performed by different surgeons and at different intervals, we have broadly classified the ROM as full or limited according to the clinician impression at follow-up (Ryu et al., 1991).
A survey was sent to all patients. Thirty-six out of 51 responded (71%). Of the 15 patients who did not respond, one had died, one declined participation in the study, one failed to recall the fracture and 12 were lost to follow-up despite extensive attempts to locate them. The patient-rating survey included an assessment of current level of hand activity, presence of ongoing hand pain (using a visual analogue scale score [VAS]) and satisfaction with their surgical or non-surgical management. The patients were asked about complications arising from the fracture and were asked to complete the quickDASH (Disabilities of the Arm, Shoulder and Hand) score. The quickDASH questionnaire is a validated testing instrument to assess hand and arm function (Hudak et al., 1996).
Patients’ parameters and outcomes were compared between patients treated operatively and non-operatively. Thirty-seven patients were included in the non-operative group and were either treated with immobilization (34 patients, 27 with a short arm cast and seven with a splint) or without immobilization (three patients). Of the three patients with no immobilization, two had non-displaced fractures and were treated with ice and an elastic bandage. One patient was a college baseball player with a mildly displaced fracture. He had no acute pain and so immobilization was not carried out and he chose to finish the season. At the end of the baseball season, nonunion was detected and led to excision of the hook. Fourteen patients were included in the operative group and were either treated with hook of hamate excision (ten patients) or open reduction internal fixation (ORIF) of the hook to the hamate (four patients). Four patients from the non-operative group failed conservative management and were treated operatively at a later stage.
Surgical techniques were similar to those reported in the past (Bishop and Beckenbaugh, 1988; Devers et al., 2013; Scheufler et al., 2005; Stark et al., 1989). Excision of the hook of the hamate was carried out through a volar incision. Release of the Guyon canal was performed and the hook was removed sub-periosteally to avoid damage to the motor branch of the ulnar nerve. ORIF was performed through a volar incision in three patients and through a dorsal approach in one patient (Scheufler et al., 2012). The volar approach was identical to that described above. The motor branch of the ulnar nerve was identified, protected and released from the fracture site. The fracture site was cleaned with a dental pick and the fracture was reduced. A cannulated compression screw was inserted under fluoroscopic guidance. The screw was countersunk so that the deep motor branch of the ulnar nerve would rest on bone. Bone morphogenic protein was added in one patient. For the dorsal approach, the skin was opened over the hamate. The extensor tendons were retracted and capsule opened. A guidewire was inserted to the hamate and into the centre of the hook under fluoroscopic guidance. Drilling was performed and the fracture was fixed with one cannulated screw.
Statistical analysis
Patient characteristics and survey responses were reported descriptively using appropriate summary statistics including median and interquartile range (IQR) for continuous variables and count and percentage for categorical variables. T-tests or Wilcoxon rank sum tests were used to compare the operative and non-operative groups for continuous variables, and chi-square or Fisher’s exact tests were used for the categorical variables. To compare outcomes from the survey between those who had a surgery as their first treatment to those who did not, regression models (both unadjusted and adjusted for time since treatment) were used. The level of significance was set at p = 0.05.
Results
Demographics and diagnosis
Patient demographics, mechanism of injury and presenting symptoms comparing the non-operative and operative group for hook of hamate fracture.
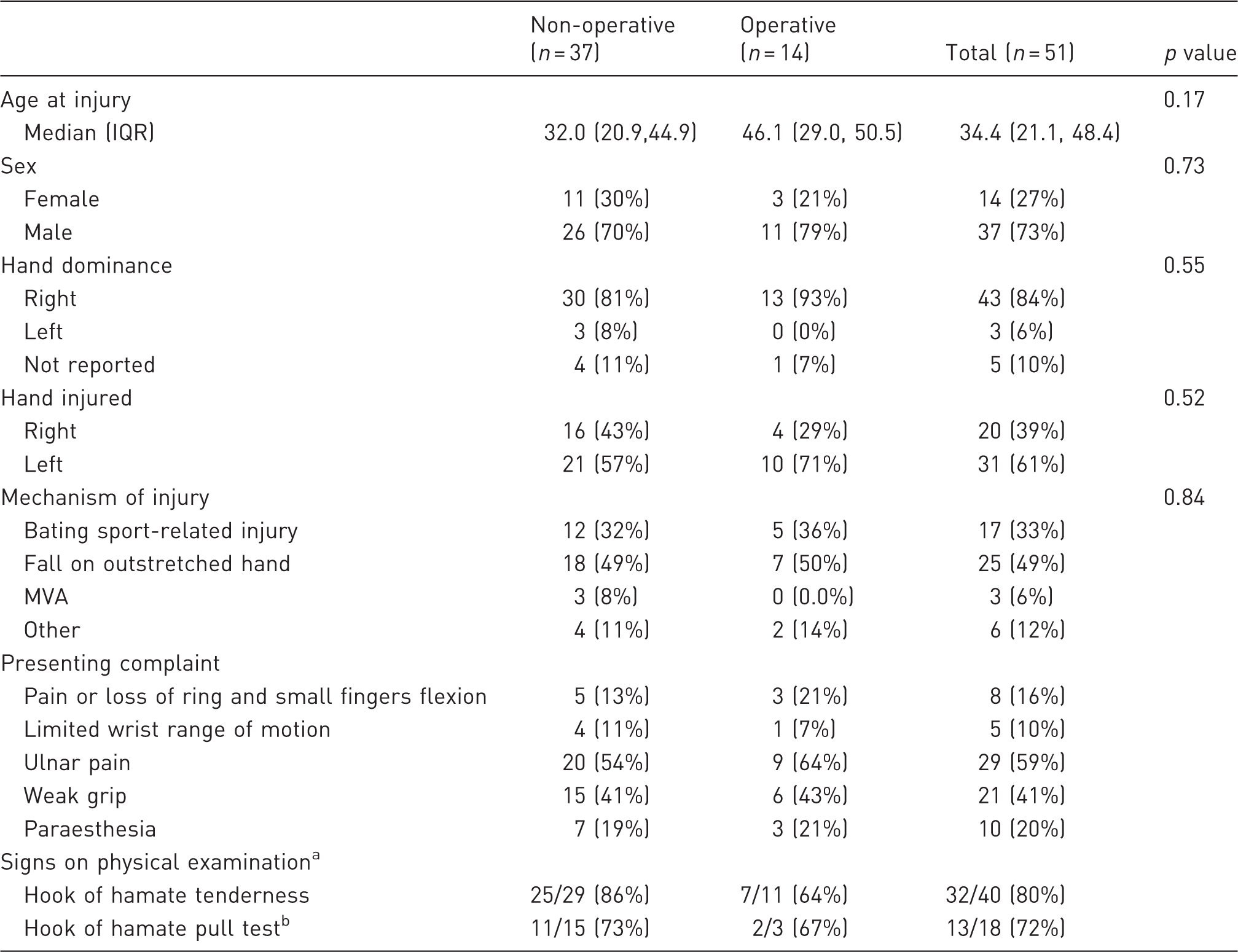
Expressed as a proportion of positives out of patients examined.
Wrist supination, ulnar deviation and small and ring finger flexion against resistance.
MVA: motor vehicle accident.
Associated hand injuries in patients with hook of hamate fractures (n = 51).
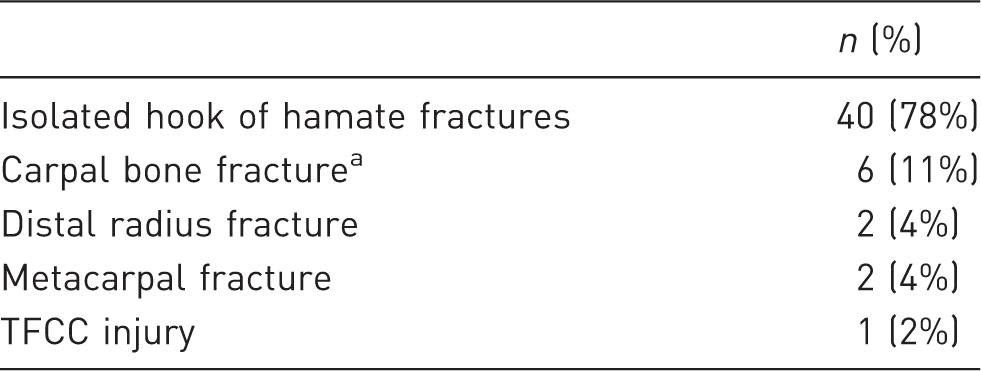
Trapezium, scaphoid and triquetrum.
TFCC: triangular fibrocartilage complex.
The most common sports related to hook of hamate injury were baseball (five patients, three of whom were professional players), hockey (six patients, two of whom were professional players) and golf (four patients, one of whom was a professional golfer). Golf injuries were all to the non-dominant hand, while other sports did not show any predilection for either dominant or non-dominant hand. Two hockey players, one baseball player and one golf player reported low grade discomfort that was exacerbated after batting or gripping the hockey stick or golf club, which might represent a stress fracture. Other mechanisms of injury included stress fractures from an extended use of crutches, a heavy object landing on the dorsum of the hand and punching a wall.
Median time from injury to diagnosis was 27 days (IQR 7.5–57.5 days). Patients were diagnosed at a median of one day after presentation to our referral centre. Ulnar wrist pain was the most common presenting complaint (29/51), yet complaints of general non-specific pain of the hand were noted in 15 of 51. Paraesthesia was common in the ulnar nerve distribution (8/10) but was also seen in the median nerve distribution (2/10). Hook of hamate tenderness was a common physical finding and was positive in 32 of the 40 patients (80%). Painful flexion of the ring and small digit while the wrist was supinated and in ulnar deviation, also known as hook of hamate pull test (Wright et al., 2010), was noted in 13 of the 18 patients who were noted to undergo the hamate pull test.
Hook of hamate fracture detection with different imaging modalities (n = 51).
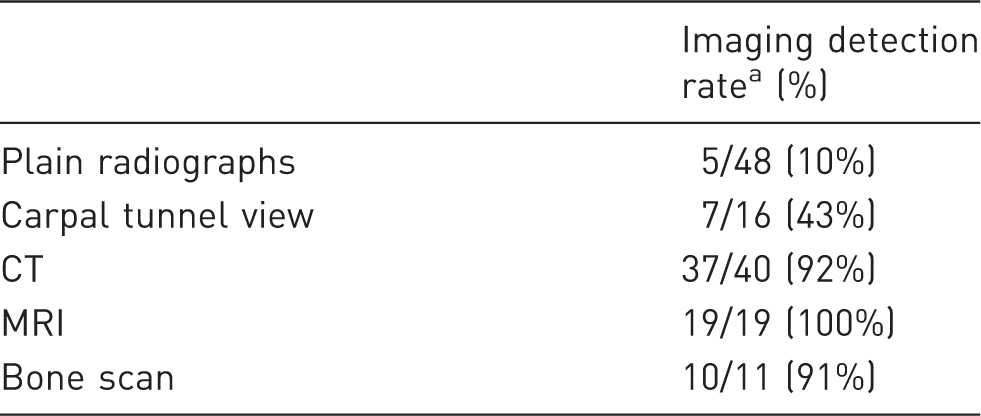
Number of positive imaging results/number of imaging performed.
Treatment and outcomes
The mean time from injury to last clinical follow-up or survey was 73 months (IQR 10.7–112.4 months). Four patients in the non-operative group failed conservative treatment and underwent subsequent excision. All patients were healthy adults, three of them were treated routinely with a cast. One baseball player, mentioned previously, chose to finish the season and had no form of immobilization. Median time from first non-operative treatment to excision in this group was 84 days (IQR 78–100.5 days). In all four cases, the surgery revealed a nonunion.
Outcomes at latest clinic follow-up comparing the non-operative and operative group for hook of hamate fracture.
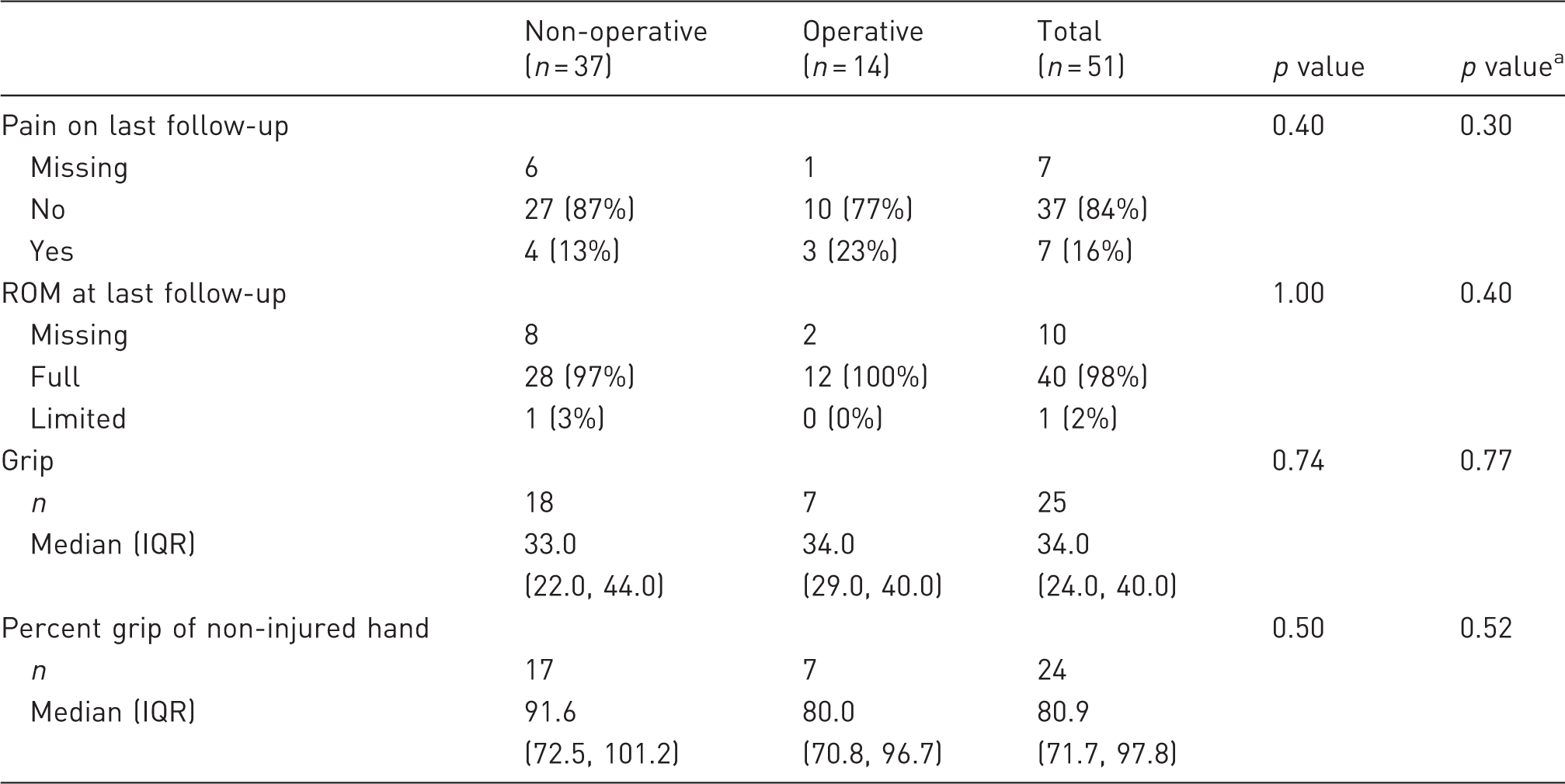
Adjusted for time since treatment.
Twenty-nine patients were assessed for fracture union with CT scans: all four patients who had ORIF and 25 patients who had non-operative treatment. Of the four patients treated with ORIF, all healed uneventfully and achieved union (Figure 1). Of the 25 treated non-operatively, six patients developed a delayed union that was defined as no sign of healing progression on imaging performed at a minimum time of 93 days from injury. There was no association between delay in diagnosis and the development of nonunion in our study. The median time from injury to diagnosis of fracture in those patients that developed a nonunion was 1.5 days (IQR 0.3–8.8 days). Four of the six went on to surgical excision of the hook as described above. Confirmation of union on CT was lacking for 12 patients in the non-operative group, and the true occurrence of nonunion in this group thus might be even higher.
Axial CT of wrist demonstrating hook of hamate fracture after a golf injury (a). Follow-up CT eight months after ORIF shows complete fracture union (b).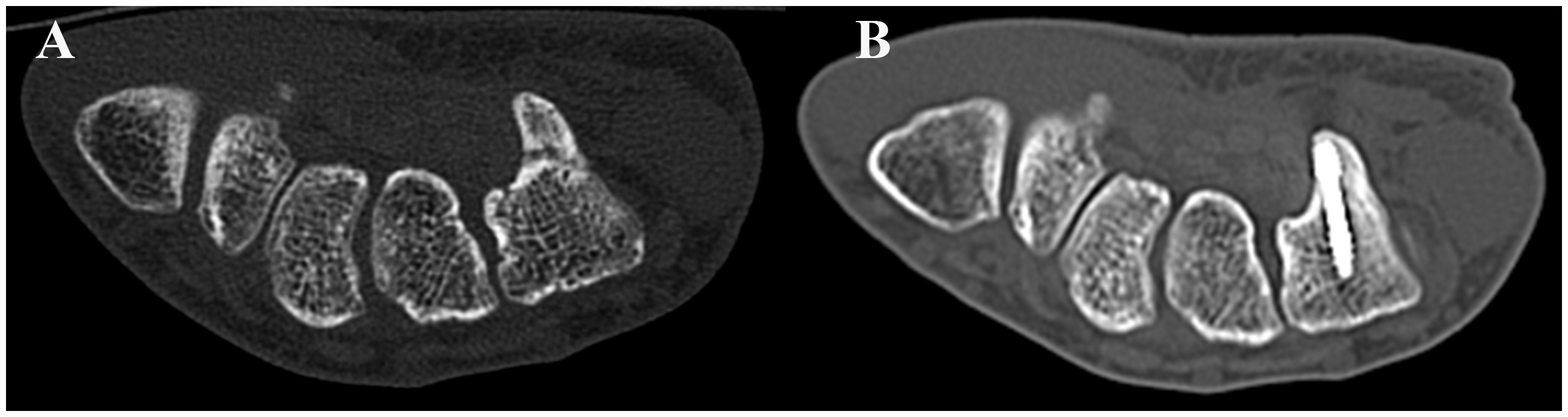
Other documented complications for the non-operative group were CRPS in two patients and carpal tunnel syndrome in one. In the operative group, chronic regional pain syndrome (CRPS) was documented for two patients after hook excision. No complications were documented for patients undergoing ORIF.
Main survey outcomes compared between the non-operative and operative group for hook of hamate fracture.
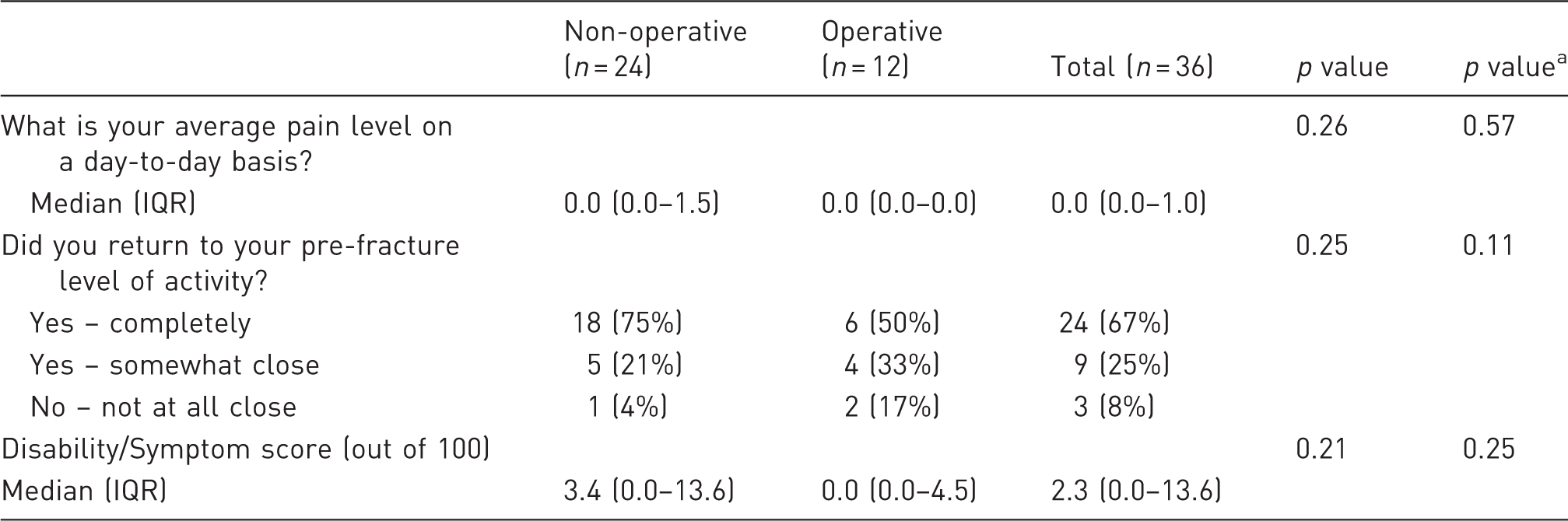
Adjusted for time since treatment.
Discussion
The diagnosis of a hook of hamate fracture can be difficult, as patient complaints may be non-specific and standard radiographs have low sensitivity in identifying the injury. The largest case series previously reported are those of Bishop and Beckenbaugh and Stark et al., both done in the 1980s. Bishop et al. reported a mean delay from injury to diagnosis of ten months, while Stark et al. reported a mean delay of six months. Patients in our cohort were diagnosed within a median of 27 days from injury. Surgeon education and early use of CT and MRI are the most probable causes of this decreased time to diagnosis (Egawa and Asai, 1983). Additionally, 57% of the patients in our cohort were originally seen by a hand surgeon, which could account for the shortened time to diagnosis. It has been recommended to obtain carpal tunnel-view radiographs to aid in the diagnosis of this fracture; however, our study showed that carpal tunnel radiographs had a detection rate of only 43%, which is low compared to other imaging modalities (Kato et al., 2000). MRI would appear to be the best imaging modality, as CT can fail to detect subtle non-displaced fractures; MRI should be performed whenever clinical suspicion is high and other imaging modalities are ineffective in detecting the fracture. CT should still be considered the first-line imaging modality due to its wide availability, low cost and high rate of detection of displaced fractures.
Despite improvements in imaging technology, physical examination remains the cornerstone of early detection and diagnosis. Our study’s findings reaffirm that ulnar-sided pain, ulnar paraesthesia, weak grip and loss of motion in the ring and small finger are all common complaints of patients with hook fractures (Walsh and Bishop, 2000). Physical findings of hook of hamate tenderness and a painful hook of hamate pull test (Wright et al., 2010) were positive in 80% and 72% of patients, respectively.
Mechanism of injury in our cohort was reported through direct and indirect impact. While previous case series reported mainly batting sport-related injuries, the main mechanism reported in our cohort was a fall on an outstretched hand, which might imply a different study population from previous reports. The indirect injury resulted from the force of the ring and small finger flexor tendons against the hook while the wrist was ulnarly deviated (Stark et al., 1977). In our cohort, golf injuries occurred only in the non-dominant hand, consistent with previous studies (Egawa and Asai, 1983; Stark et al. 1977). This mechanism has been previously described by Stark and is apparently due to the fact that the club rests on the hook of the non-dominant hand. This results in fracture when the club strikes the ground (Stark et al., 1977). This injury is preventable if the club is adjusted so as to not lie on the hook and extend beyond the hypothenar border (Walsh and Bishop, 2000).
Nonunion of the fracture is common and may be related to the poor blood supply to the hook compared to the hamate (Failla, 1993; Panagis et al., 1983). Some clinicians believe that nonunion is the natural course of this fracture rather than a complication (Devers et al. 2013; Scheufler et al., 2005) because of the poor blood supply and motion at the fracture site (Failla, 1993). Our findings suggest a high incidence of nonunion for fractures treated without surgery (6/25) while there were no cases of nonunion for patients treated with ORIF (4/4). The fractures that went on to nonunion were diagnosed in a timely fashion. These findings contradict Failla et al. and Whalen et al., who both claimed that timely diagnosis and immobilization ultimately leads to fracture union, while late diagnosis is the main culprit of nonunion. Management of the nonunion with hook excision generated excellent results in our cohort; thus, if the patient is against early surgery, it would be reasonable to treat a patient with casting alone, but the surgeon should educate them on the risks of nonunion and how nonunion can be managed. In contrast, in professional athletes, for whom early return to sports is important, early excision might provide the quickest recovery.
This study has several limitations. First, it is a relatively small retrospective study, thus limiting the ability to identify significant outcome differences between groups. Furthermore, for statistical analysis purposes, we grouped surgical repair as one treatment group that includes different procedures with different indications. Second, the survey results are subject to recall bias. Additionally, pain and quickDASH scores were obtained at a single time point, which did not allow for changes in these values to be followed over time. Longer follow-up times are needed to detect complications such as flexor tendon irritation. Third, the fractures were assessed by many surgeons and lacked standardized diagnosis and treatment techniques. Lastly, our study was prone to referral-centre bias that might skew the true demographics of this rare injury and might underestimate the incidence of complications. Despite these weaknesses, our study has a long follow-up and represents one of the largest cohorts of this rare injury and is the largest performed with contemporary imaging modalities. Additionally, the survey had a high response rate and utilized validated patient outcome measures to evaluate patient function.
In conclusion, we have reported the largest group of patients diagnosed with hook of hamate fracture in the era of routine CT and MRI. Time to diagnosis of hook of hamate fracture has improved with the use of contemporary imaging modalities. Nonunion was the most common complication of patients treated without surgery and persisted despite early diagnosis and immobilization of the fracture. None of the patients who underwent ORIF had nonunion. Patient outcomes were good to excellent regardless of the treatment chosen, with minimal pain and good hand functionality. Since late treatment of nonunion with hook excision achieved excellent results, we endorse the approach of close patient follow-up and ad hoc treatment of nonunion in patients who do not desire immediate surgery.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Moran is a consultant for Integra.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Mayo Clinic Orthopedic Research Review Committee (ORCC) Small Grant Program. The funding source was not involved in writing or collection, analysis and interpretation of data for this study.
Ethical Committee approval
This study was approved be the Mayo Clinic Institutional Review Board (15-009055).