
Abstract
The purpose of this study was to evaluate long-term outcomes of the free functioning gracilis transfer in children with traumatic total brachial plexus palsy. We used the free functioning gracilis transfer to reconstruct elbow flexion and prehension in 17 children with a mean age of 13.4 years (range 3–17) who were followed-up over a mean period of 6 years (range 2–16). The transferred gracilis delivered a stable elbow flexion with a useful power, as well as reconstructed active finger motion. In 3–11-year-old patients we noted a tendency towards developing a progressive flexion contracture of the elbow. The limb length discrepancy observed in our patients was not different from the brachial plexus palsy patients treated without the free functioning gracilis transfer. In conclusion, the free functioning gracilis transfer is a reliable reconstructive technique for reanimating upper extremity in children of all ages capable of delivering stable function over a long period of time.
Introduction
Over the past three decades, free functioning muscle transfer has become an established technique for reconstructing the upper extremity function, with the gracilis muscle becoming the number one choice in a reconstructive surgeon’s armamentarium (Fischer et al., 2013). In particular, cases of total brachial plexus palsy (BPP), failed primary reconstruction and delayed presentation have become indications for the free functioning gracilis transfer (FFGT) in adults to reconstruct elbow flexion (Barrie et al., 2004) and prehension (Dodakundi et al., 2013; Doi, 2008).
While the role of the FFGT in adult BPP patients has now been widely accepted, its use in paediatric patients remains a little controversial. There are several reasons for that. First, the functional outcome of the FFGT is heavily dependent on the postoperative physiotherapy. Regimens that are used last for several months and comprise complex and time-consuming exercises (Doi et al., 2008). Thus, even in adults, a careful patient selection needs to be carried out to ensure the patient is fully committed to the treatment. Depending on the age of the child and the stage of its mental development, the compliance poses a challenge, potentially leading to a failure of the procedure. Second, there is an uncertainty regarding a growth of the injured extremity and of the transferred muscle, which could lead to a deformity formation. A degree of growth retardation in the upper limb is observed in the paediatric patients with BPP per se (Bain et al., 2012), but does this change in the context of the FFGT? These are all very important issues, which could negate the long-term outcome and therefore must be carefully assessed. Finally, the technical aspects of the procedure need to be mentioned, although these might have been sufficiently mitigated by already published reports (Chim et al., 2014; Doi et al., 2011; El-Gammal et al., 2015; Kay et al., 2010).
In this study we present the senior author’s experience with the FFGT performed for BPP in children of various ages. The primary focus of the study is analysis of the elbow and finger function delivered by the FFGT and its longevity. Secondarily, we analysed growth disturbance of the injured extremity in comparison with paediatric BPP patients treated without the FFGT. In contrast with all the studies published thus far, we present a detailed analysis of all relevant parameters over substantial periods of time in an attempt to achieve the best possible long-term outcome of the FFGT in children.
Methods
Patients
We surveyed records of patients treated at our institution for traumatic total BPP, received a FFGT, were 17 years of age or younger and had at least 2 years of follow-up, to be included the study. The study was approved by our institutional review board with patients’ informed consent obtained. All the patients had preoperative clinical exam, Electromyography and Magnetic Resonance imaging of the brachial plexus to establish the extent of the injury. The findings were discussed with patients’ parents and patients (where possible). An option to undergo the FFGT was outlined with a detailed explanation of the procedure, postoperative course and likely outcomes. In case of an agreement, a treatment plan was formulated on a per-patient basis to include the FFGT, accompanied by nerve transfers depending on the availability of donor nerves. The main indication for the FFGT was reconstructing elbow flexion combined with finger function.
Surgical technique
The procedure used was reported previously (Doi et al., 2013). Upon plexus exploration if C5 or C6 lesions were postganglionic, they were used for shoulder and/or triceps neurotization. In cases of unavailability of these roots, the contralateral C7 root was transferred with vascularized ulnar nerve graft. These additional procedures were performed 1 month prior or at the time of the first FFGT. For the FFGT, the cephalic vein and thoracoacromial artery were identified through incision in the deltopectoral groove. Recipient site for the gracilis transfer was prepared by creating a subcutaneous tunnel on the anteromedial aspect of the arm, with additional incisions over the anterior cubital fossa and posterior or anterior aspect of the forearm. Tendons of extensor digitorum communis or flexor digitorum profundus were identified, divided and sutured together. A pulley for the transferred muscle was created at the elbow, under the brachioradialis and radial wrist extensors (Figure 1), or under the pronator teres (Figure 2). Through a transverse incision in the contralateral medial thigh, the gracilis myocutaneous flap was harvested with its nutrient vessels and motor nerve. The muscle flap was transferred onto the upper arm and inserted onto the acromion and lateral clavicle proximally, with the Pulvertaft weave into the extensor tendons distally (Figure 1).
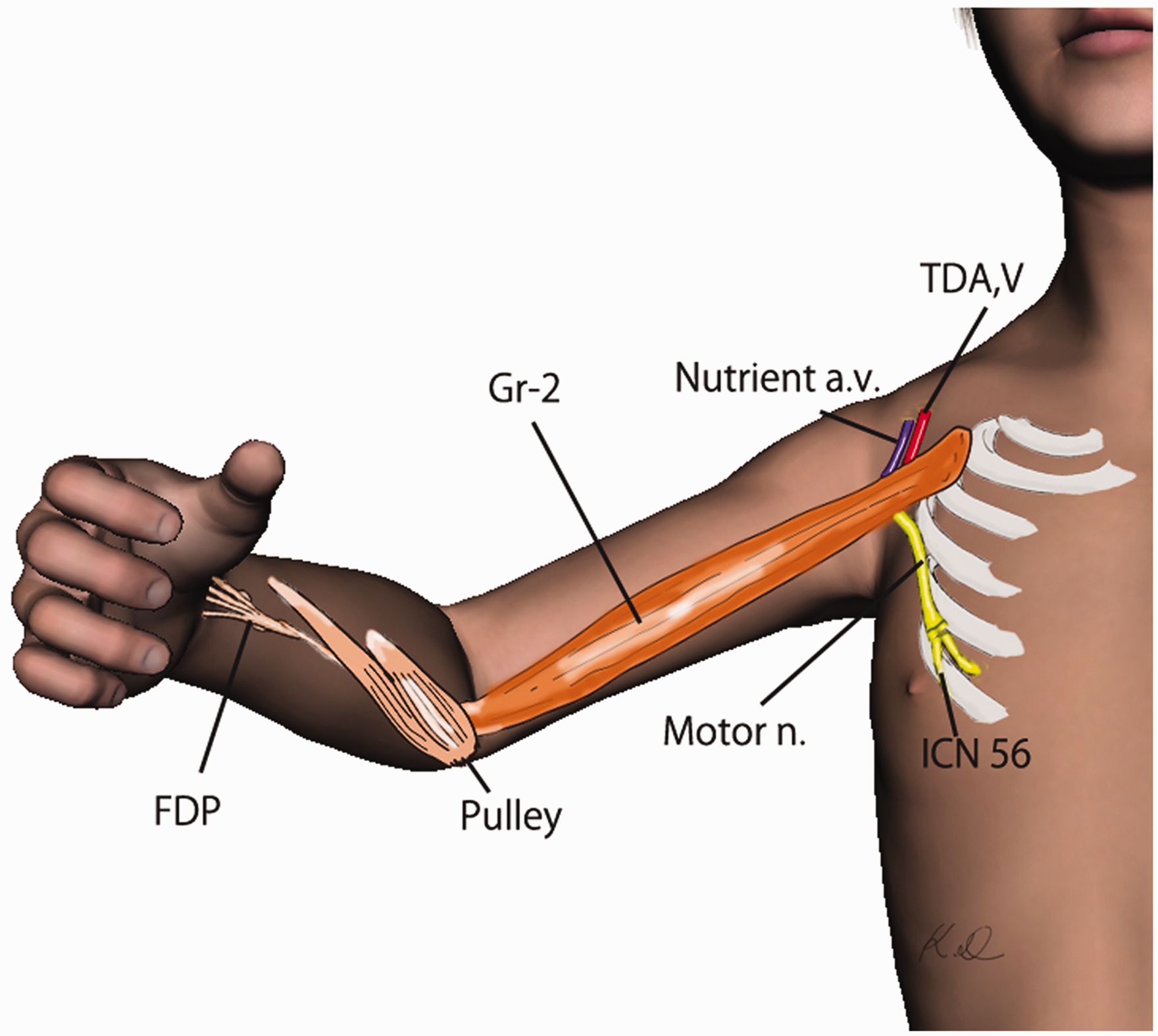
The surgical technique of Gracilis 1 free functioning muscle transfer for restoration of elbow flexion and finger extension. Gracilis 2 free functioning muscle transfer for restoration of elbow flexion and finger flexion.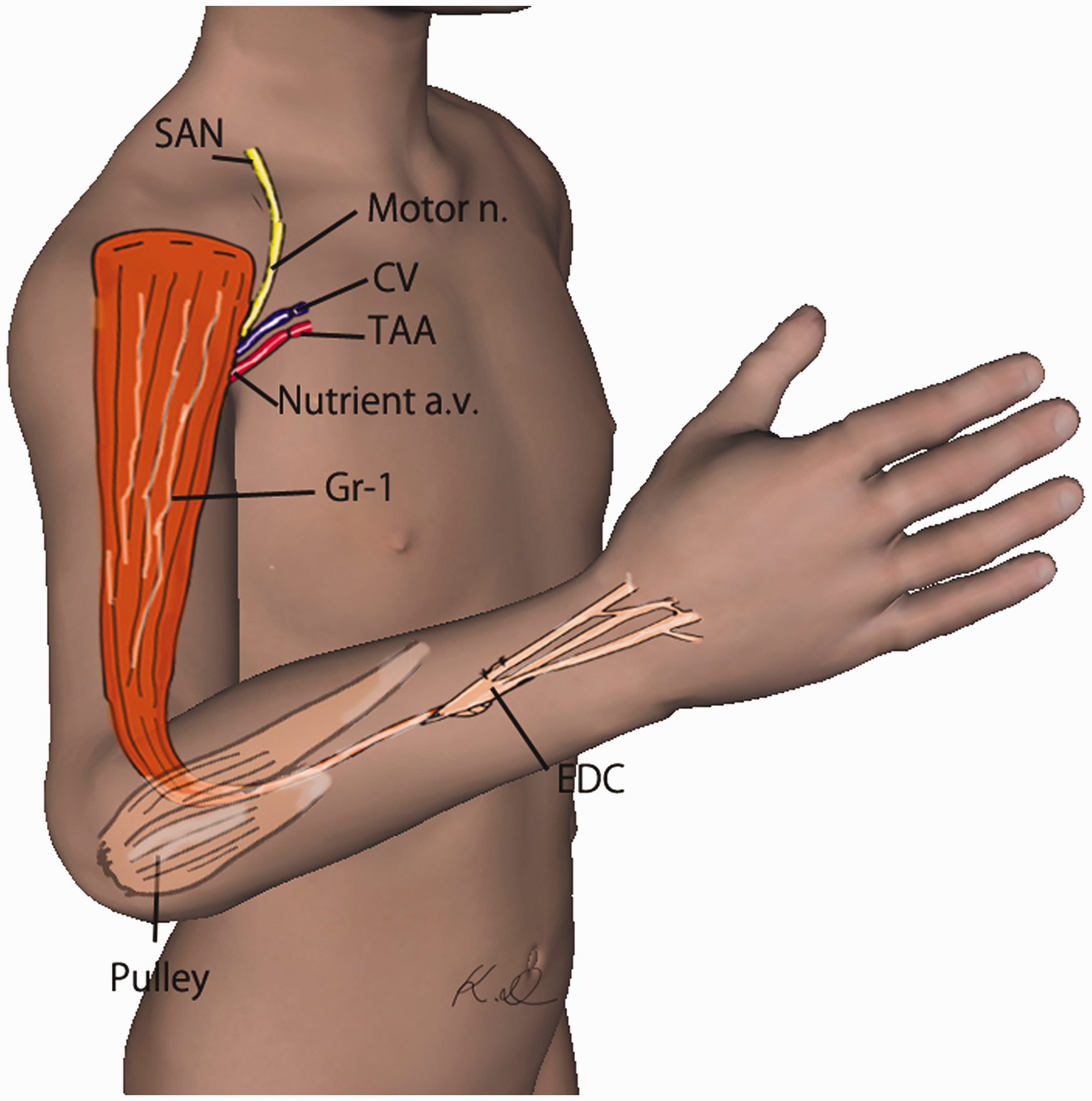
Thoracoacromial vessels and a spinal accessory nerve were used as donors, except for a case of a 17-year-old male where the spinal accessory nerve was injured and phrenic nerve was used instead. Postoperatively the upper limb was immobilized with the use of an arm brace and a cast keeping the shoulder in 30° of abduction, 30° of flexion and 60° of internal rotation, the elbow in 100° of flexion, the wrist in the neutral position and the fingers in forced flexion or extension for 8 weeks. Subsequently, a sling was used to prevent subluxation of the glenohumeral joint until the recovery of shoulder girdle muscles. The second gracilis transfer was performed a mean of 4.6 months after the first one (range 2–22 months). We did not perform the second FFGT earlier than 2 months after the first one and it depended on the progress of the physiotherapy (elbow initially held at 100° of flexion was gradually extended) as well as patients psychological recovery from the fist surgery and their life circumstances.
The second muscle flap was harvested from the ipsilateral thigh and proximally attached to the second and third ribs, with the thoracodorsal vessels and intercostal nerves (5+6 or 3+4) as the donors of choice (Figure 2).
Early passive mobilization was started 1 week after the procedure by a combination of the following manipulations done with the wrist kept in neutral. For the FFGT used to reconstruct finger extension the gracilis tendon was compressed at the elbow to extend the fingers. Then as the compression was released, the fingers were passively flexed, which introduced traction on the tendon with about 25 mm excursion of the repair site (Doi et al., 2008). Opposite finger movement was used if the FFGT was used to reconstruct finger flexion. The wrist tenodesis technique was also performed with the patient’s wrist forced passively into flexion and extension by the therapist. Surface EMG biofeedback was used after the EMG confirmation of reinnervation of the transferred muscle to facilitate establishing of separate activation patterns for the two transferred muscles.
The maximum elbow extension allowed was limited to –30° in order to overcome biomechanical disadvantage of the FFGT to flex the elbow from full extension. The wrist was long-term immobilized in the neutral position by a splint, which in a proportion of patients led to a contracture sufficient to stabilize the wrist. If the wrist remained unstable, wrist fusion was performed at a later date.
Outcome measures
The patients were assessed for early vascular complications and need for any salvage intervention. To evaluate early reinnervation of the transferred muscle, compliant patients had EMG studies from 3 months postoperatively and followed monthly until matured motor-unit-potentials were recorded. The long-term recovery of function was tested by active range of motion of shoulder, elbow and fingers, together with the British Medical Research Council (MRC) muscle power testing. All the patients had the Mallet score for shoulder and elbow function and Raimondi scores for hand function (Al-Qattan, 2003) assessed before the treatment and at the time of their last follow-up. Bowstringing of the gracilis tendon at the elbow was graded into: (0) no bowstring, (1) minimal only at maximal flexion, (2) apparent at flexion, (3) apparent at rest.
Patients older than 15 years of age were asked to fill the DASH questionnaire before and after the treatment.
Statistical analysis
The data was analysed separately for young (3∼11 years old) children and old (15–17 years old) children at three follow-up stages as explained below. Comparison between the two groups at each follow-up stage was done by Student t-test or Mann–Whitney test. Comparison among the three time points within each group was done by repeated measures one-way analysis of variance test, and for the non-parametric data Friedman test was used. A correlation between the elbow flexion/extension power ratio and elbow-extension range of motion was done by Spearman’s rank correlation test. The statistical significance level was set at p-value < 0.05. Power of post hoc analysis was set at 0.8.
Results
General results
Demographics of patients.
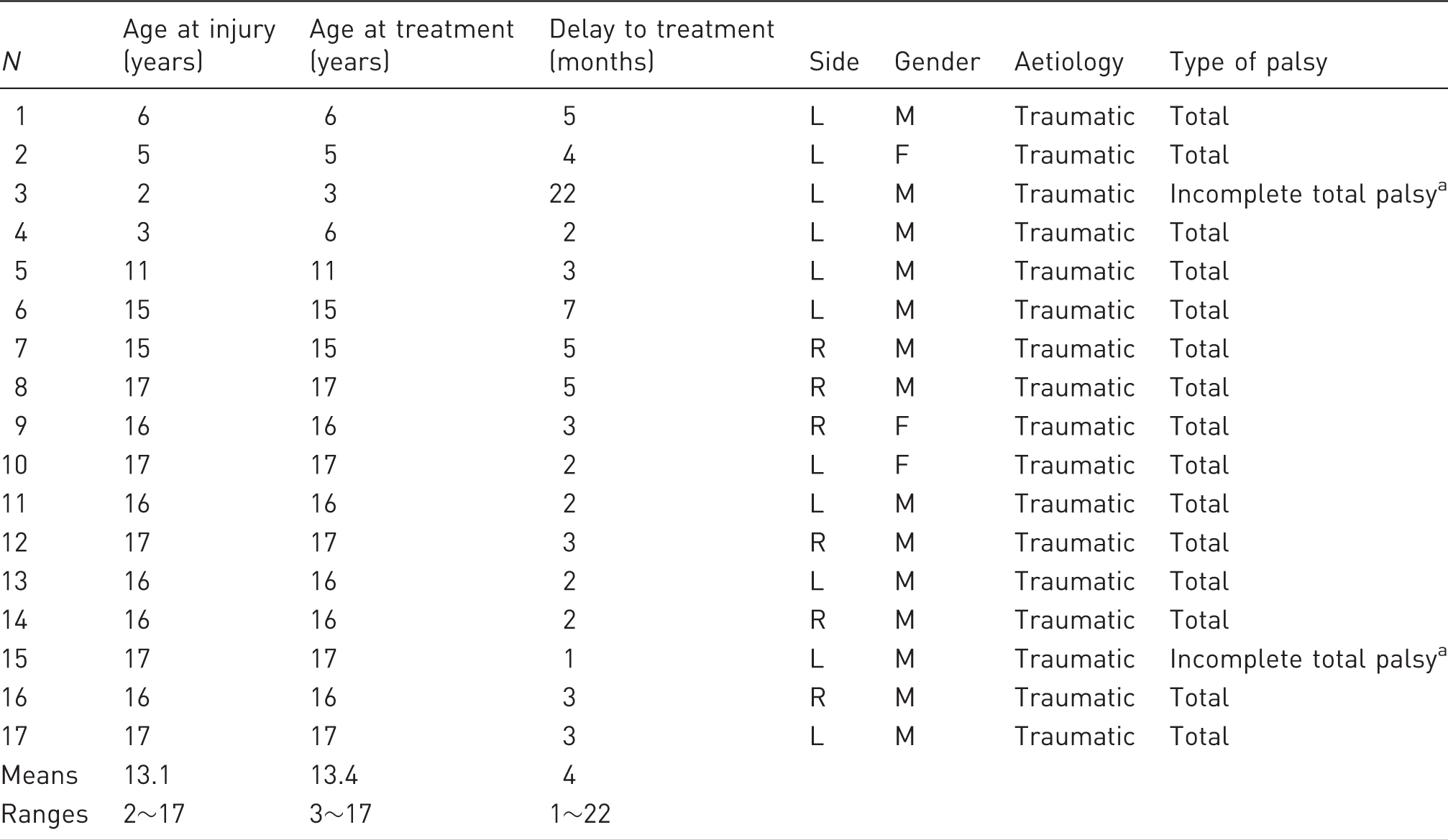
Explanation in the text.
Partial C5 root function recovery.
Summary of the operative procedures.
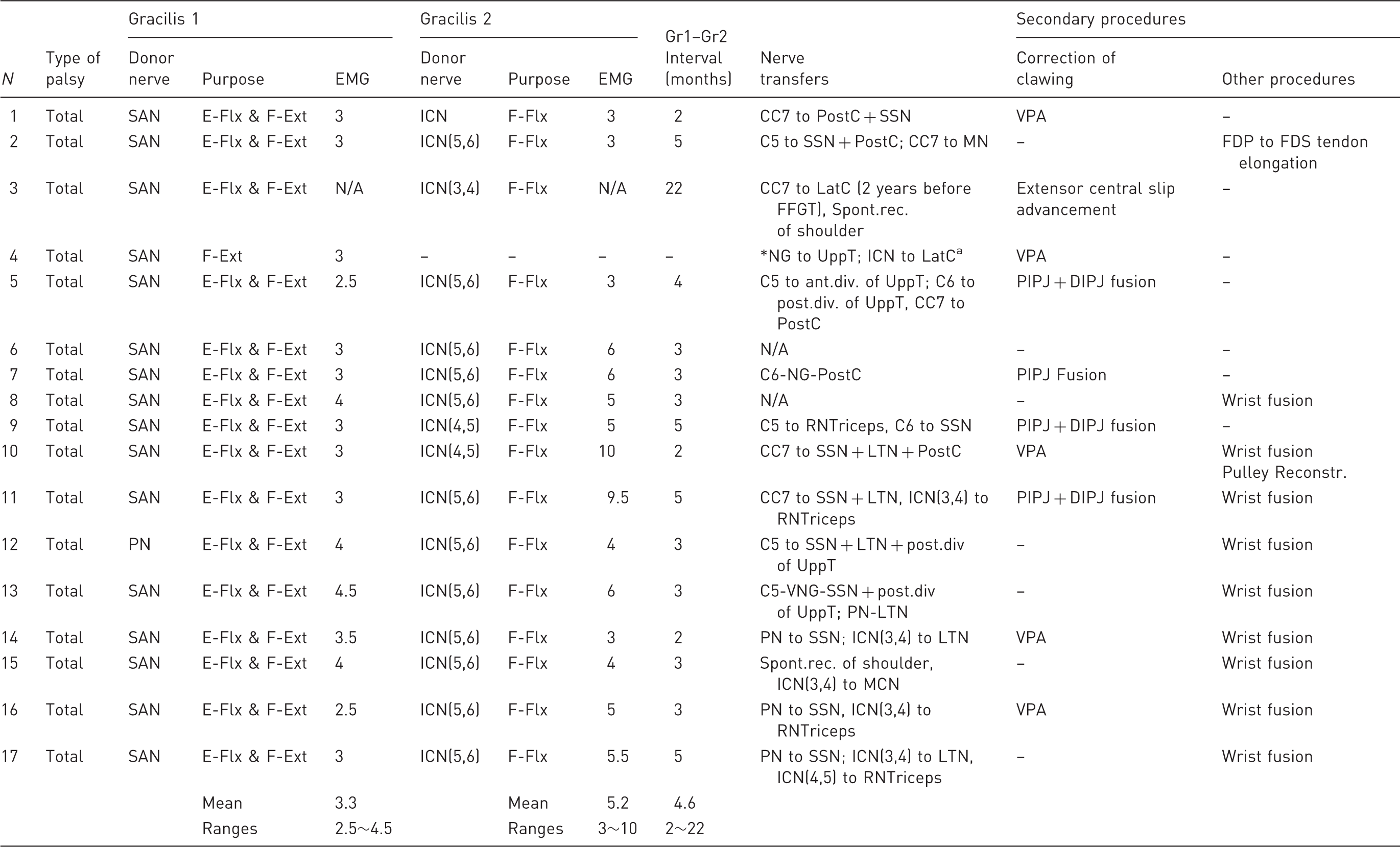
SAN: spinal accessory nerve; ICN: intercostal nerve; PN: phrenic nerve; E: elbow; W: wrist; F: fingers; Flx: flexion; Ext: extension; CC7: contralateral C7; UppT: upper trunk; PostC: posterior cord; LatC: lateral cord; MedC: medial cord; SSN: suprascapular nerve; LTN: long thoracic nerve; MCN: musculocutaneous nerve; RNTriceps: radial nerve branch to long head of triceps; NG: nerve graft; VNG: vascularized nerve graft; VPA: Zancolli's volar plate advancement; Spont.rec.: partial spontanneous recovery; N/A: not available or did not test; EMG: Reinnervation time after FFGT (months); m: months; Gr1: Gracilis 1; Gr2: Gracilis 2; FFGT: free functional gracilis transfer; FDP: flexor digitorum profundus tendon; FDS: flexor digiturum superficial tendon; PIPJ: proximal interphalangeal joint; DIPJ: distal interphalangeal joint.
Procedure performed at other hospital.
We did not experience any vascular complications related to the muscle transfers. All transferred muscles got successfully reinnervated. The reinnervation was confirmed by EMG in 31 transfers, with the mean reinnervation time of 3.3 months (range 2.5–4.5) for gracilis 1 transfer and 5.2 months (range 3–10) for gracilis 2 transfer. The remaining two transferred muscles started visible contraction 4 and 5 months postoperatively.
Elbow function
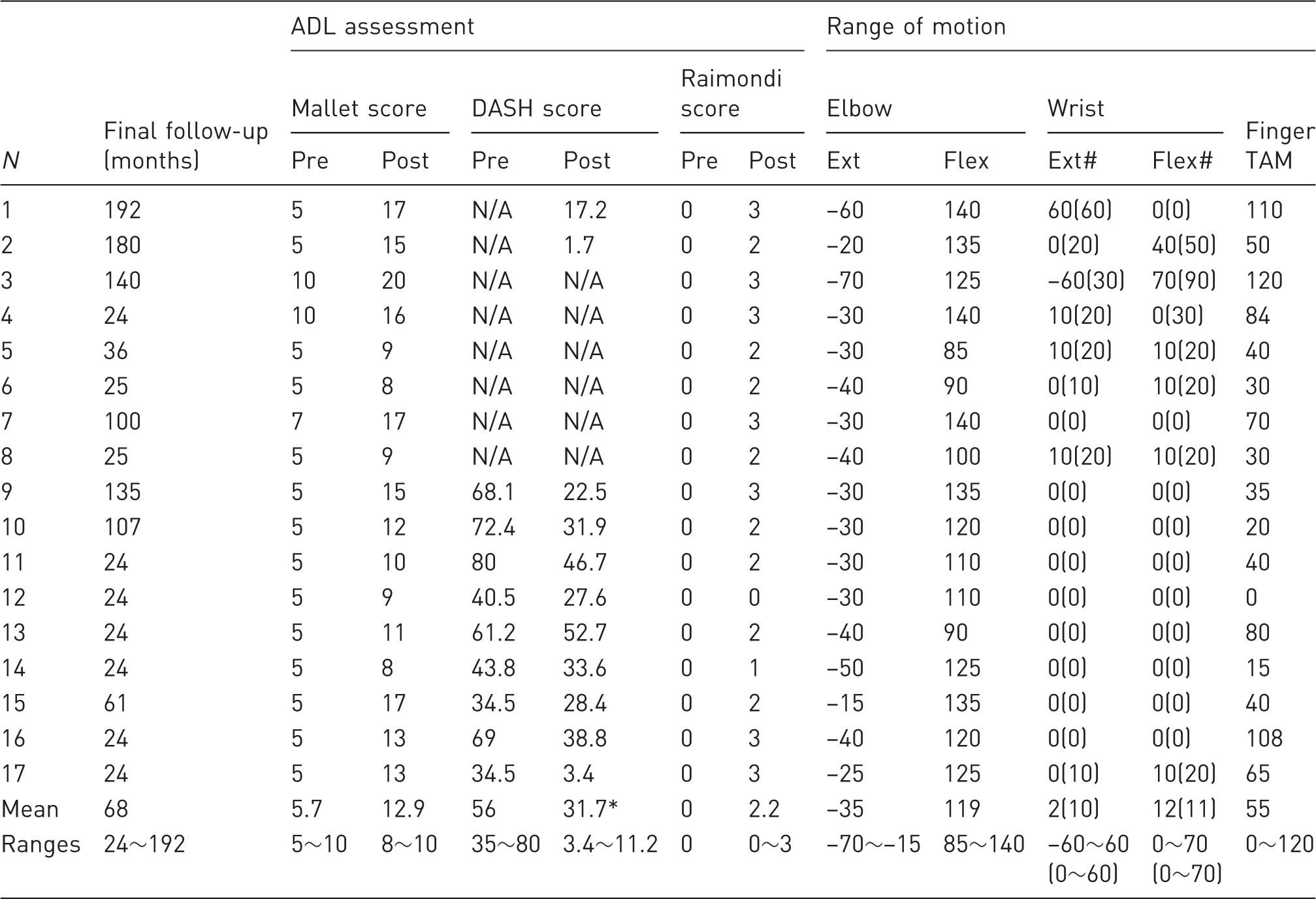
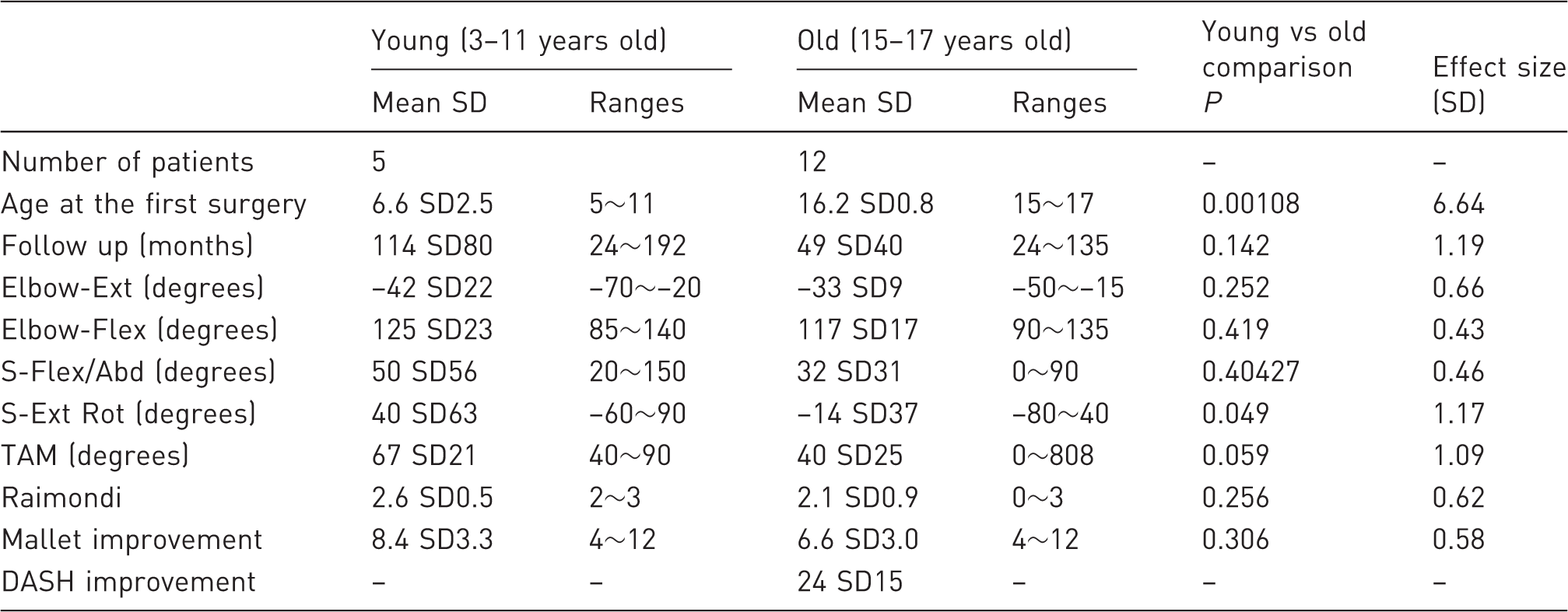
We have closely monitored this parameter over three follow-up stages: (1) early, 2 years after the surgery (mean 2.2 years); (2) mid-term, 5 years after the surgery (mean 5.2 years); and (3) long-term, 10 and more years after the surgery (mean 11.2 years postop with the longest follow-up of 16 years). Because of physiological differences related to the growth pace (Satake et al., 1993), we separately analysed the data for five young children (3–11 years old) and 12 old children (15–17 year old). On examining the elbow flexion, we found that all patients achieved more than 100° of elbow flexion and the range of motion was stable over the follow-up in both groups (Figure 3, upper part). However, a gradually increasing flexion contracture was found in two patients in the young group (Figure 3, lower part). There was no statistically significant difference in the elbow flexion and extension range of motion between the two groups at the final follow-up stages (detailed data in Table 3, summary Table 4).
Time course of active elbow flexion and extension for three young patients (Cases 1,2,3) and three old patients (Cases 7,9,10,1), who completed all three periods of the follow-up. Differences in the range of elbow motion among the follow-up stages within the groups were compared by the repeated measure analysis of variance. Significant differences were not detected in the elbow extension (young, p = 0.282; old, p = 0.444) and flexion (young, p = 0.694; old, p = 0.420) among three stages. Long-term outcomes. Flx: flexion; Ext: extension; : active (passive) range of motion; TAM: total active finger motion; N/A: not available or did not test; Raimondi: Raimondi’s Hand Function Assessment Score; Mallet: Mallet’s score; DASH: disabilities of arm, shoulder and hand disability score; ADL: activity in daily living. Comparison of long-term functional outcomes between young and old children. TAM: total active finger motion; Ext: extension; Flex: flexion; S: shoulder; Abd: abduction; Ext Rot: external rotation; Raimondi: Raimondi’s Hand Function Assessment Score, Mallet-Mallet’s Score; DASH: disabilities of arm, shoulder and hand disability score. Data presented is based on values at the final follow-up as outlined in Table 3, not at the stage 3.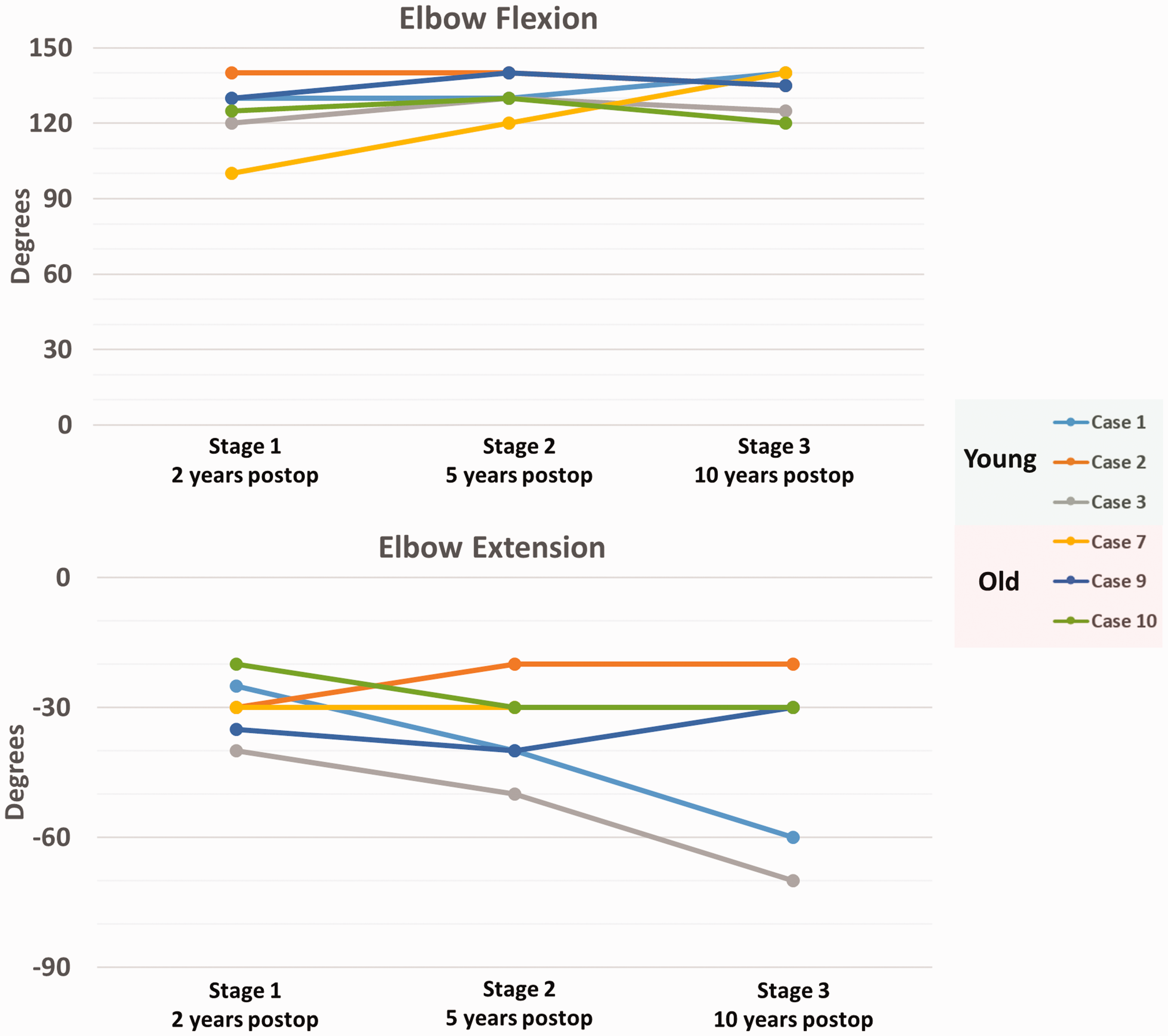
The transferred gracilis muscles delivered a useful elbow flexion strength with three patients reaching MRC grade 3, 12 patients grade 4 and two patients reaching grade 4+. The power grade was achieved during the early follow-up stage and did not change during the course of the follow-up, however, the power of elbow extension recovered later than that of elbow flexion.
Next, we hypothesized a correlation between the elbow extension power and flexion contracture degree. We detected negative correlation between the two variables in the old group (p = 0.018, correlation coefficient = 0.679, Figure 4) but not in the young group (p = 0.11). Importantly, there was no correlation between the elbow flexion power and degree of elbow flexion contracture in both groups.
Correlation between the triceps power and elbow flexion contracture in the group of 14–17 year olds. The positive correlation was found with the p of 0.018 and Spearman’s rank correlation coefficient of 0.679.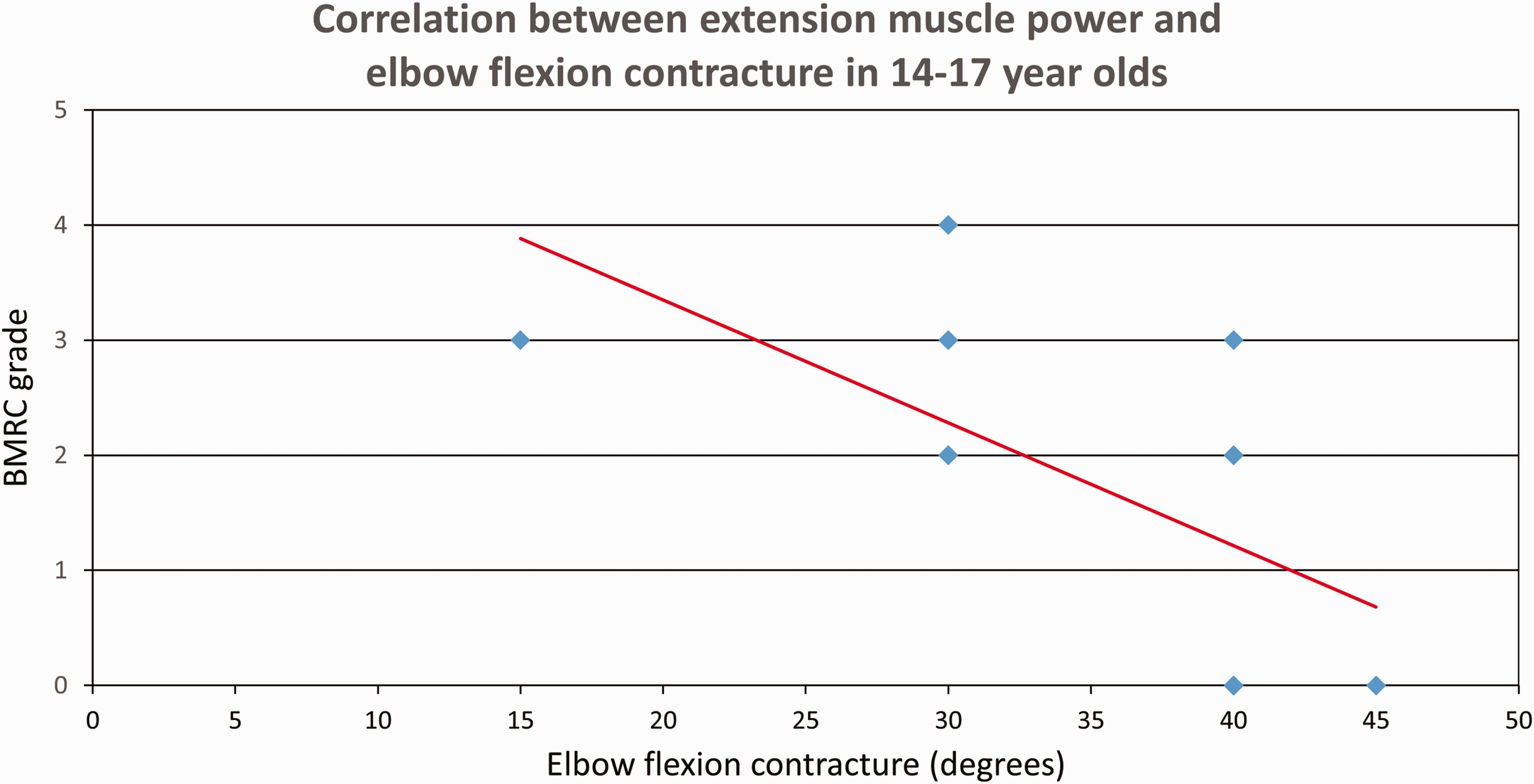
Three patients developed prominent bowstringing of the gracilis at the elbow, one underwent pulley reconstruction using long wrist extensor tendon and one elongation of the gracilis tendon. There was no statistically significant correlation between bowstringing grading and elbow flexion contracture (Spearman, γ = –0.166, p = 0.194).
Finger function
Time course of the total amplitude of active finger motion (TAM) is shown in Figure 5, in detail in Table 3. The TAM in the young group reached its peak at stage 2 and decreased thereafter, however, still maintaining satisfactory motion at the stage 3. In contrast, the TAM of the old group initially recovered only lower values that were stable over the follow-up period.
Time course of the total active finger motion (TAM) in young and old groups at the three follow-up stages. Explanation in the text.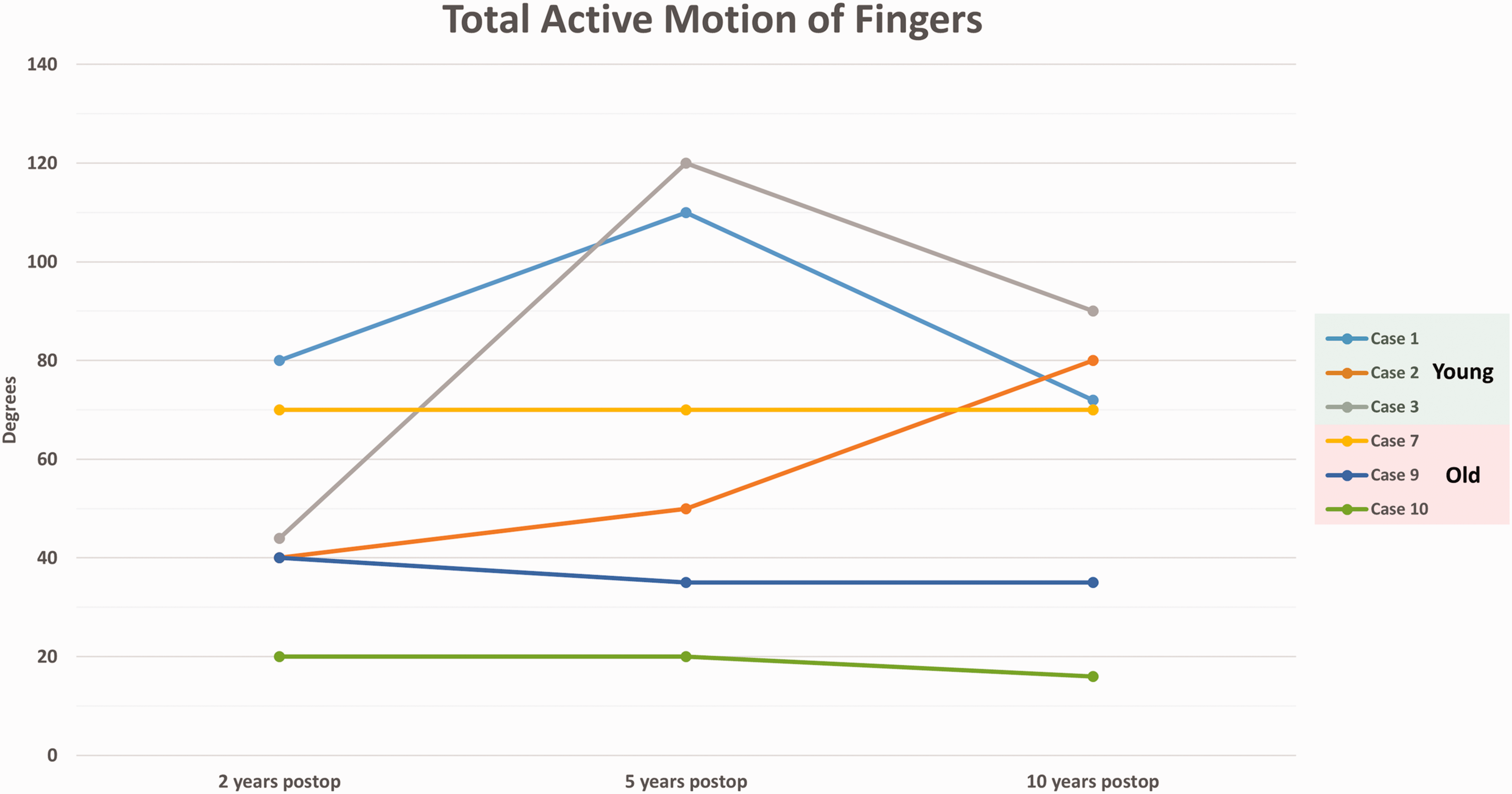
At the stage 2, there was a statistically significant difference in the TAM between the young and old groups (p = 0.021, effect size: 1.83 SD = 55°). No statistically significant difference was detected at the stage 1 and 3 (p = 0.375 and 0.513).
There was a moderate negative correlation between the TAM and age of surgery (Spearman, γ = –0.570, p = 0.013), however, no correlation between the TAM and power of elbow flexion (Spearman, γ = 0.529), elbow extension (Spearman γ = 0.536, p = 0.116), ratio of elbow flexion/extension (Spearman, γ = –0.285, p = 0.401) and bowstringing grading (Spearman, γ = –0.176, p = 0.253).
The Raimondi score did not show a statistically significant difference between the young and old groups (Table 4).
Shoulder function
The amplitude of active shoulder movement is shown in Table 3. For global assessment of the shoulder function we recorded the Mallet score, which improved by 8.4 (4∼12) in the young group and 6.6 (4∼12) in the old group, with no statistically significant difference between groups (p = 0.360) (Table 4). This improvement was mostly attributable to the nerve transfers around the shoulder, although the FFGT contributed to the ‘hand to mouth’ component of the score.
DASH
Nine patients in the old group returned the DASH questionnaire, the score of which improved the mean of 24.3 (range 6.1∼45.6) (Tables 3 and 4). The mean improvement exceeded the minimal clinically important difference for the DASH of 17 (Smith et al., 2012). The greatest improvements (p < 0.05) involved opening a tight or new jar (question 1), carrying a heavy object weighing more than 10 lb (4.5 kg) (question 11), and putting on a pullover sweater (question 15). Two patients in the young group returned the DASH after they reached 20 years of age, with the scores of 17.2 and 1.2.
Limb length discrepancy in young children
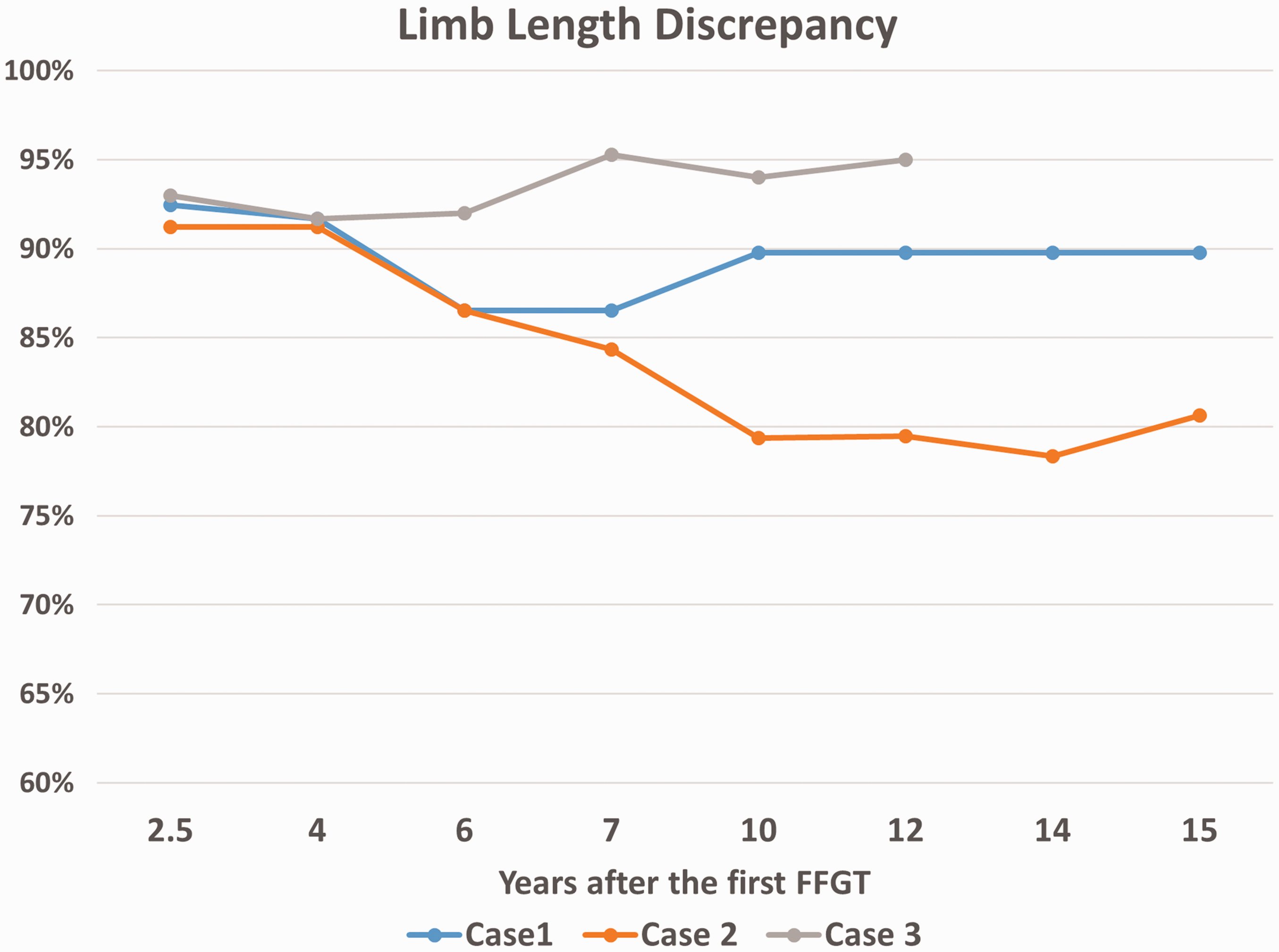
In three patients with the longest follow-up in the young group we measured the total length of the upper limb from the acromion to the middle finger tip and compared it with the contralateral side (Case presentations in Figure 6). We detected limb length differences of 90%, 81% and 95% of the length of the contralateral limb at the final follow-up 16, 15 and 12 years after the first FFGT, respectively. These patients had almost identical background in terms of age at the time of injury, type of palsy, surgical procedures, length of follow-up and postoperative functional recovery. It was interesting to observe the dynamics of developing the limb length discrepancy in these children as in spite of these similarities it varied markedly (Figure 7).
Presentation of three cases from the group of young children group. (a) Case 1 has been using his reconstructed limb while working and in daily activities. The discrepancy in upper limb length was 90%. (b) Case 2 is a female patient who initially used the injured limb in everyday life, however upon reaching adolescence became very conscious of its appearance and started to hide it. The eventual difference in limb length was 81%. To address this she requested elongation of the limb purely for aesthetic reasons. (c) Case 3 had the smallest discrepancy in the limb length with only 95% of the uninvolved limb, although his follow-up length is shorter than the first two cases. He is, however, the most active boy who plays football and swims. (d) Comparative data of the three cases are summarized. Time course of developing the limb length discrepancy in cases presented in Figure 6.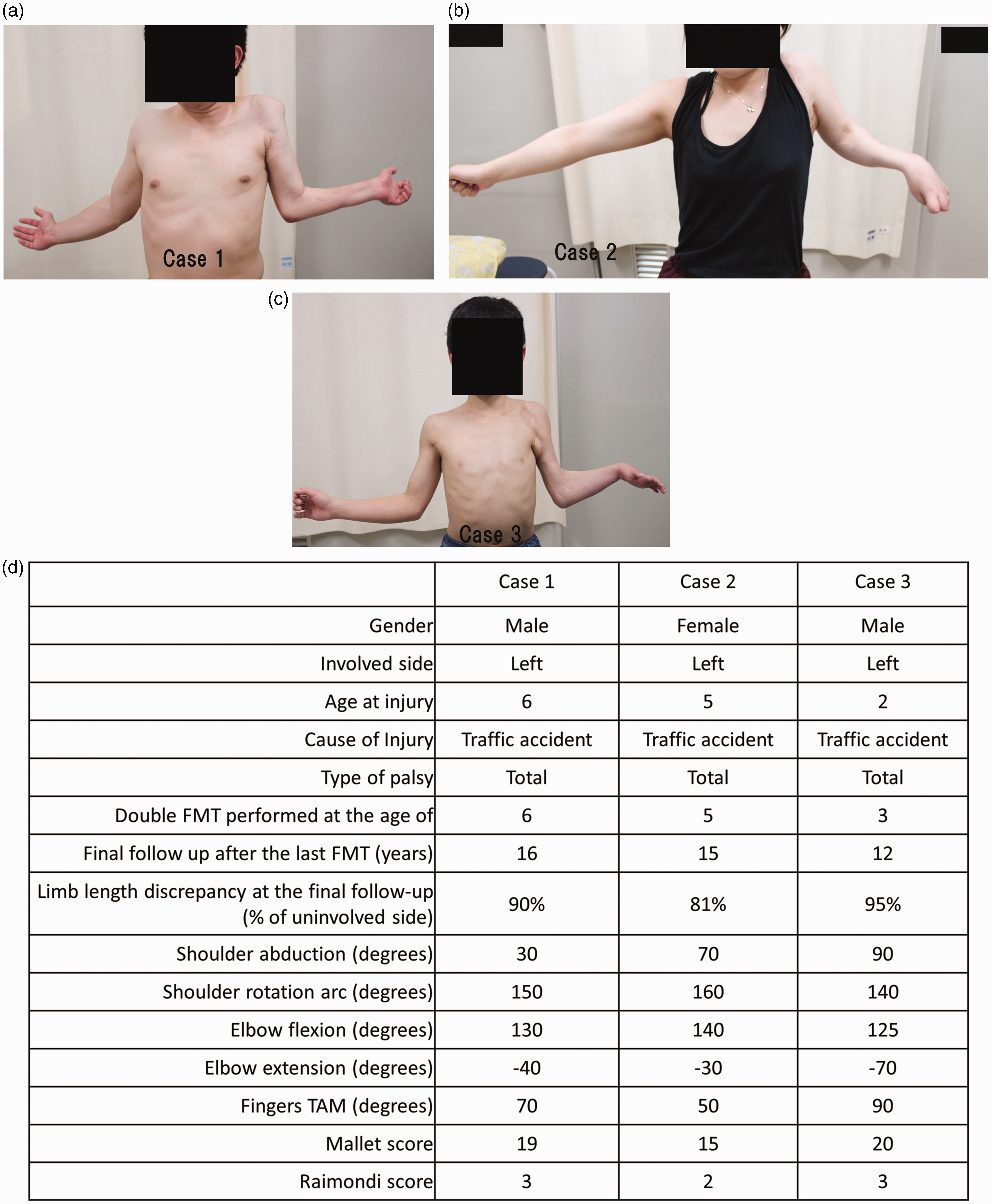
Discussion
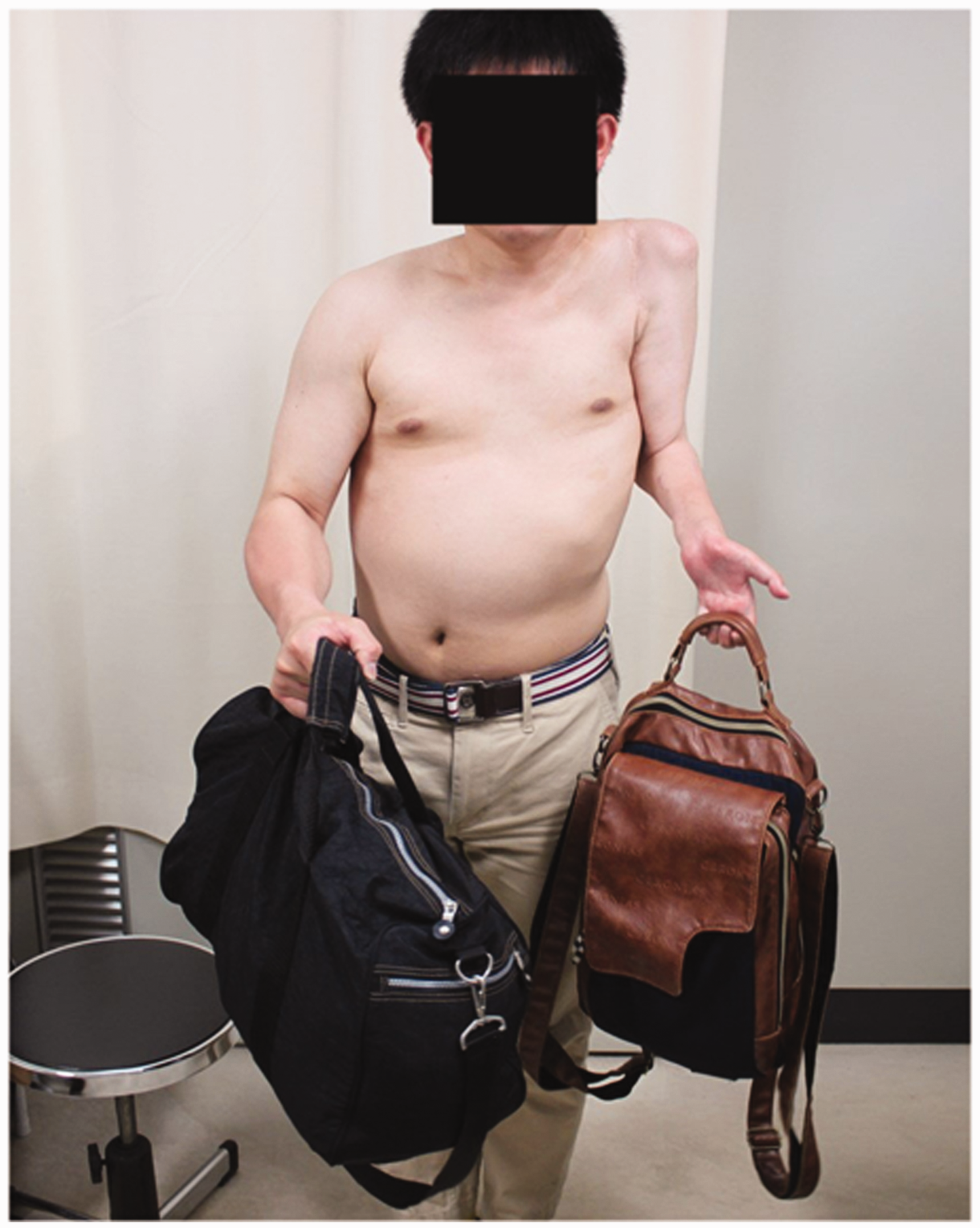
Management of the traumatic BPP in paediatric patients is a very challenging task, especially when the palsy is total. In these situations, the FFGT seems like a very attractive, if not indispensable, option to restore the upper extremity function. The FFGT in children may seem more challenging than in adults, however we did not experience any failure and achieved a higher procedure success rate than in adults (Dodakundi et al., 2013; Doi, 2008). The FFGTs successfully reanimated the flail limb in our patients, allowing for a good control of the whole arm from shoulder to fingers. The results were stable over more than 10 years of the follow-up bringing many of our patients into adulthood. Although the transferred muscles were not able to provide fine finger movements, such as pinch or grasp, it restored a useful hook grip (Figure 8). Together with additional procedures, the FFGT delivered the ability to use the paralysed limb independently (Figure 9) or for bimanual activities. This was reflected by a significant improvement in Raimondi and DASH scores. However, before embarking on the FFGT in a paediatric patient, there are particular points that need to be discussed.
Case 1 demonstrating ability to actively extend and flex fingers 17 years after the double FFGT. The patient (Case 1) demonstrating the ability to hold a bad with his reconstructed hand 17 years after the double FFGT.
Chim et al. (2014) used the FFGT in 12 children with the BPP and found that two patients developed elbow flexion contracture, which they, at least partly, attributed to the vascular compromise of their flaps. Although they did not provide any quantification of their observations and their short follow-up prevented them from adequately evaluating the phenomenon, they concluded that the FFGT should be carefully considered in children. We had no postoperative vascular compromise, but we also experienced elbow flexion contracture of more than 50° in three cases in the group of 3–11 year olds. In two of them the contracture was progressively worsening. In the group of 14–17 year olds, the flexion contracture developed as well, albeit the degree of it was milder, and it inversely correlated with the power of triceps. Elbow flexion contracture of more than 30° is not uncommon after obstetric brachial plexus palsy (OBPP) treated without the FFGT (Ballinger and Hoffer, 1994; Ho et al., 2010). It is thought to be caused by an imbalance between elbow flexors and extensors and timing of their recovery (Ballinger and Hoffer, 1994). Such minor contracture (≤30°) is actually useful in FFGT patients as it reduces the biomechanical disadvantage of the FFGT to flex the elbow from full extension. In our rehabilitation protocol we intentionally limit the elbow extension to –30°. However, in some of our patients the contracture worsened over time, so there ought to be other aggravating factors in play. First to consider is a possible discrepancy between the growth of transferred muscle and the growth of upper limb. Indeed, the younger age is the time where the skeletal growth is the most active (de Onis et al., 2009). The average elongation of the long bones in extremities from the age of 3 to 13 are 21 cm for femur, 13 cm for humerus and 10 cm for radius (Maresh, 1955; Smith and Buschang, 2004, 2005). If we presume that the gracilis grows at the same rate as if it was in the thigh, the projected difference in length is not very significant – especially when we know the growth rate of the paralysed extremity is slower than the healthy one. While this factor may be contributing to the elbow contracture, it is clear it cannot act on its own. The second possible explanation is the biomechanical aspect of placing the gracilis across the elbow joint in order to reconstruct movement in more distal joints. Because of a non-anatomical position of the tendon, a degree of bowstringing is likely to develop when the muscle contracts. This pulley insufficiency then leads to a gradual shortening of the muscle to preserve the extent of motion and myostatic contracture develops (Figure 10). The third reason is applicable to the children who did not regularly use their reconstructed extremities in everyday activities. Their elbows were held in slight flexion most of the time, with the elbow flexion power superior to extension, following which a habitual flexion contracture ensued. We realize that this conclusion is purely based on our observation, as at the time when this study was carried out there were no tools to reproducibly quantify involvement of extremity in daily activities in young children. Finally, we might have failed to detect the correlation between the triceps power and elbow extension be due to a small sample.
Mechanism of developing elbow flexion contracture secondary to bowstringing of the transferred gracilis over the elbow joint. The gracilis transfer was used to reconstruct the finger or wrist function with a pulley created at the elbow, under the brachioradialis and radial wrist extensors or under the pronator teres. The gracilis tendon was then sutured to the finger flexors or extensors in the forearm. Strong contraction of the gracilis muscle produced the pulley insufficiency and resulted in bowstringing of the gracilis (black arrow). The elongated moment arm of the gracilis (black line to red line) decreased the amplitude of the gracilis contraction (pink to red arrows) and produced myostatic contracture, which was further aggravated by the weak triceps muscle.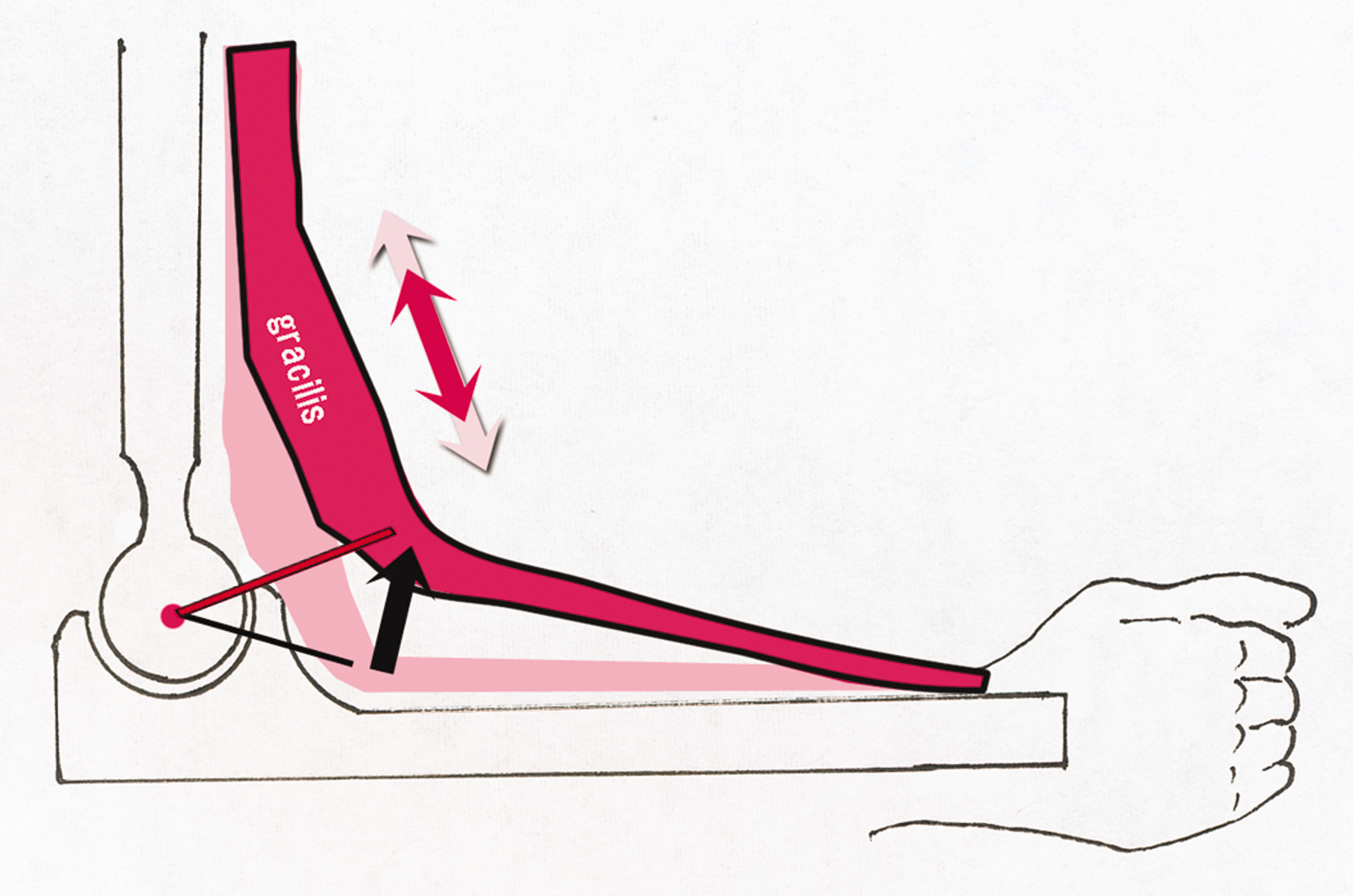
Another point to discuss is the limb growth disturbance. Three young children developed 90%, 81% and 95% of the length of the contralateral limb at the final follow-up ranging from 12 to 16 years post FFGT. We compared the limb length differences of our patients with the literature data in the obstetric BPP treated without the FFGT (Bain et al., 2012; Gosk et al., 2014; Terzis and Kokkalis, 2010) and we did not detect any difference, although we recognize that the groups were not matched in terms of aetiology and severity of the palsy (the control group consisted of patients with birth-related palsy mostly limited to upper roots). Although our small sample precludes us from making any firm conclusions, we have no reason to believe that the FFGT further aggravates the already-disturbed growth of the paralysed extremity.
When embarking on the FFGT in a paediatric patient, one needs to adopt approaches to prevent elbow flexion contracture, which include long-term use of elbow-extending splints during the night and selecting a strong nerve donor for triceps reinnervation. As in all BPP treatment, the ultimate aim needs to be using the injured extremity in everyday life, with targeted occupational therapy to achieve this goal.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Institutional Review Board of Ogori Daiichi General Hospital no. 2014-03.