A Genome-Wide Association Study of Carpal Tunnel Syndrome Reveals 13 Novel Susceptibility Loci
Mr Akira Wiberg, Mr Michael Ng, Professor Annina Schmid, Dr Georgios Baskozos, Professor David Bennett and Professor Dominic Furniss
NDORMS, University of Oxford
Time in programme: Thursday 3rd May 2018 09:05
Aim: Carpal tunnel syndrome (CTS) is a complex disease, whereby genetic and non-genetic factors interact to affect overall phenotypic expression. Little is known about the genetic contribution to CTS, and our aim was to discover genetic variants that confer risk to CTS.
Methods: We undertook the first ever genome-wide association study (GWAS) in subjects with CTS using the UK Biobank resource, a prospective cohort study of ∼500,000 who have had whole-genome genotyping undertaken. After quality control, we defined 12,106 participants of white British ancestry with at least one diagnostic code for CTS as our cases, and used the remaining 387,347 white British participants as controls.
Results: We discovered genome-wide significant associations (p ≤ 5×10−8) at 13 loci across the genome. Of the top three associated variants, rs72755233 (p = 9.1 × 10−15) is a missense variant in ADAMTS17, rs62621197 (p = 1.0 × 10−13) is a missense variant in ADAMTS10, and rs3791679 (p = 3.8 × 10−13) is in an enhancer region in an intron of EFEMP1. All three genes are important in extracellular matrix modulation, and we demonstrated expression of these genes in surgically resected tenosynovium from CTS patients. rs72755233, rs62621197 and rs3791679 have been reported in previous GWAS to be associated with human height, and we found that on average, UK Biobank CTS patients are >2 cm shorter than controls.
Conclusion: This study provides novel insights into the biology of CTS. Our findings support the hypothesis that the genetic susceptibility to CTS may arise from aberrant connective tissue architecture or from altered musculoskeletal growth and development, rather than from rendering peripheral nerves intrinsically more vulnerable to increased pressures.
Long-Term Satisfaction Following Syndactyly Correction is Independent of the use of Skin Grafts
Miss Bien Ferrari and Professor Paul M N Werker
University Medical Centre Groningen
Time in programme: Thursday 3rd May 2018 09:12
Aims: Graft-less techniques for syndactyly correction are advocated because of graft-related complications and donor site morbidity. The purpose of this cross sectional study was to compare division with and without skin grafts on complications, long-term results, scar quality and patient satisfaction, to find out if grafting concerns patients too.
Methods: Fifty-five patients (94 webs) with a median follow-up of 10.8 years (IQR:5.2-15.8) were included in this retrospective analysis. Data were extracted from medical files and operation notes. Twenty-seven patients (49 webs) were willing to participate in clinical follow-up. The Patient and Observer Scar Assessment Scale (POSAS), Withey score for post-operative success and a patient satisfaction survey were used outcome measures.
Results: Hypertrophic scarring (p = 0.044) occurred significantly more often in the graft group. Web creep, scar contracture and revision rates were higher in the graft group. There were no significant differences found in POSAS, Withey and satisfaction scores. Observer scar scores differed 7.5 points in favour of the graft-less group. The highest satisfaction score was given for digital function (median:8.7/IQR:7.2-9.4) and worst for nail appearance after synonychia separation (median:5.9/IQR:4.7-8.4). Satisfaction with the donor site was high in the graft group (median:8.5/IQR:7.3-9.5).
Conclusion: This study confirms that graft-less corrections should be preferred over skin grafts, because it has a lower rate of unfavourable outcomes. However, from a patients' perspective, the type of technique does not affect the final degree of satisfaction nor the opinion on scar appearance. This is valuable information when skin grafts are inevitable.
A Randomised Feasibility Trial Comparing Needle Fasciotomy (NF) with Limited Fasciectomy (LF) for Dupuytren’s Contractures
Professor Timothy R C Davis on behalf of the HAND-1 study investigators
Nottingham University Hospitals
Time in programme: Thursday 3rd May 09:19
Aim: To assess the feasibility of a multicentre randomised trial comparing Needle Fasciotomy (NF) with Limited Fasciectomy (LF)for Dupuytren’s contractures (DC).
Methods: A randomised feasibility trial of DC patients aged ≥18 recruited at three clinics in England. Participants were randomised to either NF or LF treatment. Follow-up was at 2, 6 and 26 weeks post surgery. Outcomes were numbers of patients screened, eligible, randomised and followed up, treatment adherence, and identification of a primary outcome Patient Reported Outcome Measure (PROM) for a future trial.
Results: Of 267 patients screened, 153 were eligible and 71 randomised (46%). The commonest reason for ineligibility was previous DC surgery to the same hand (n = 48). 75 eligible patients (49%) were not randomised due to treatment preference. Four participants did not receive their randomised treatment. Median time to treatment was 97 (LF) and 41 (NF) days. Follow-up at 26 weeks was 85%. Participants felt that the MYMOP and PEM PROMS allowed them to better describe the condition of their hands at each of the three post-surgery follow-up timesthan the DASH or URAM.
Conclusions: This study demonstrates that a definitive RCT is feasible. Broadening the inclusion criteria could increase the number of potentially eligible patients, and follow up duration should take surgery waiting time into account. The MYMOP or PEM appear the most suitable for use as the primary outcome.
Trial Registration: ISRCTN11164292
Funding: NIHR RfPB (PB-PG-0613-31083). The views expressed are those of the author(s) and not necessarily those of the NHS, NIHR or Department of Health.
The Non-Surgical Management of Bony Mallet Injuries
Mr Ryan William Trickett, Mr James Brock and Mr David Shewring
University Hospital of Wales
Time in programme: Thursday 3rd May 2018 09:26
Aims: There is no consensus on the optimal management for bony mallet injuries. Large fragments or a subluxated joint may be indications for surgery. However surgery has not been proven to be superior to splinting and is associated with more serious complications. This paper reviews the non-surgical management of these injuries.
Methods: Over a 4 year period 220 mallet fractures in 213 patients were treated using a custom made thermoplastic splint. Fractures were classified according to the Wehbé and Schneider classification. Clinical results were collected prospectively, including VASpain, active range of motion and extensor lag. All patients were later invited to complete a Patient Evaluation Measure (PEM).
Results: There were 132 males and 81 females with a mean age of 42 years (Range 12-93).
Mean splinting duration was 6.8 weeks. Joints were congruent in 160 and subluxated in 58. There were 2 physeal injuries. Less than 1/3 of the articular surface was involved in 94, 1/3 to 2/3 in 100 and over 2/3 in 26 fingers.
At discharge from hand therapy (mean 85 days) mean distal interphalangeal joint active range of motion was 2 to 75°. Overall42 patients had a measurable extension deficit; the mean lag in this group was 10°.
The mean PEM percentage was 22% at a mean of 1.75 years.
Comparing subluxated and congruent joints there were no statistically significant differences in active range of movement or PEM score. There was no significant differences in active range of movement or PEM score depending on the fragment size or the individual Wehbé and Schneider classification.
Conclusions: Conservative treatment in this large cohort demonstrates good outcomes. Splinting is adequate treatment for bony mallet injury regardless of size or subluxation.
Proximal Replantation: Challenges and Outcomes in Limited Resources Hospitals in Developing Countries
Mr Hazem Alfeky, Professor Essam Taman, Dr Ahmed Omran, Dr Mohammed Swilam and Dr Mohammed Elshahat
Whiston Hospital
Time in programme: Thursday 3rd May 2018 09:33
Aim: Proximal hand and forearm amputations are devastating injuries. With thehigh rate of these injuries in developing countries and their limited resources, there are more challenges in the replantation procedures compared to the UK. these are primarily the cost of the procedure and the post-operative rehabilitation.Besides, prediction of the outcomeis always uncertain due to multi factorial risk factors including the mode of injury, level of amputation, presence of contamination and the extent of the damage to the neuro-vascular tree, general patient status and co-morbidities.
Patients and methods: We present our experience of a series of 17 post traumatic proximal hand and forearm replantations over a 5-year period in 2 major trauma centres in Egypt. All patients were operated on in the same theatre environment, received the same postoperative rehabilitation. Follow up ranged between 16 to64 months (Average: 20).
Results: All the 17 cases were successful.Mean age was36.4. Operative time in total 18.5 hours. Average number of secondary procedures is 4.6 procedures. 2case developed wound healing problems and tendon rupture and required extra procedures. Overall patient satisfaction was excellent.
Conclusion: Proximal hand and forearm replantation is awarding procedure. Effictivenessthroughout the whole procedure can cut down the costs while keeping high standard of care. It requires well trained MDT as well as patient willingness to achieve desired outcomes.
Limb Hypoplasia in Obstetric Branchial Plexus Injuries - A Longitudinal Study
Miss Taj Tomouk, Mr Henk Giele, Mr George Wheble and Mr Simon Maciburko
Royal Free Hospital
Time in programme: Thursday 3rd May 2018 09:40
Aims: Upper limb hypoplasia in obstetric brachial plexus injury (OBPI) is not well documented. This study evaluates the degree of upper limb hypoplasia with extent of plexus injury and surgical intervention as well as the inter-rater reliability of the Mallet score classification.
Methods: A retrospective review of OBPI patient case notes between 1998 and 2017. Data comprised patient demographics, Narakas grade, whether primary nerve or shoulder surgery was performed, and measurements of both upper limbs. True and apparent arm lengths were compared and mean percentage differences were calculated between the affected and contralateral upper limbs. Two blinded observers graded patient photographs using the modified Mallet score.
Results: A total of 62 patients were identified and underwent 209 sets of measurements during the study period, two thirds of whom had sequential measurements. The majority of the cohort were females with right sided injuries and a Narakas grade of 1. Approximately one third had primary nerve surgery while almost double (60.7%) underwent a shoulder procedure.
Mean percentage differences between the affected and contralateral upper limbs across the cohort were 9.3% for clavicular length, 7.8% apparent arm length, 7.3% humeral length, 5.9% forearm length, 5.7% hand circumference and 7.8% scapular length. The two raters chose the same Mallet score in approximately three quarters of cases.
Conclusions: This study shows that OBPI leads to quantifiable hypoplasia of the upper limb, and that the Mallet score is a reliable tool for assessment. To our knowledge this is the longest longitudinal study to quantify upper limb hypoplasia secondary to OBPI.
Evolution of Combination Therapy for Upper Limb Spasticity Management: 1500 Limbs Report
Mr Hazem Alfeky and Mr Paul Mcarhur
Alder Hey Children Hospital
Time in programme Thursday 3rd May 2018 09:47
Aims: Upper limb spasticity is a major long-term complication of stroke, cerebral palsy and head injury. Historically managed by physiotherapy/early-active rehabilitation the introduction of focal botulinum toxin injections has assisted with the therapy and improved outcomes. However the need to repeat the injections and the onset of muscle fibrosis are known considerations. Spasticity modifying surgery, including neurectomy, Tendon transfer / lengthening and Arthrodesis, does constitute a large part of the armamentarium upper limb that surgeons have to achieve more long lasting results. Combining all these modalities in a time specific manner based on the individual needs of each patient seems to be the most effective long term guaranteed management.
Methods: We present the senior author 14years’ experience of more than 1200 interventions in cases of upper limb spasticity management and the evolution of the combination therapy over the years through comparing the long-term outcomes and results of single/individual versus combination therapy of upper limb spasticity.
Results: Patients were assessed in a multidisciplinary setting. Hand Therapy, patient, family and carersall contribute to outcome assessment. A combined approach to treatment in parelell provides better outcomes in a more time efficient way rather than the traditional series approach.
Conclusions: Successful management of upper limb spasticity requires more than Botulinum injections. We recommend treating the patients within MDT setting and the early consideration of combination therapy to improve the long-term outcomes.
How to Diagnose a ‘TOS’ser
Ms Roisin Dolan, Professor Henk Giele, Dr Ravi Knight, Ms Jia See and Dr Vivek Murthy
John Radcliffe Hospital
Time in Programme: Thursday 3rd May 2018 09:54
Aims: The aim of this study was to correlate symptoms, pre-operative clinical provocative tests, radiological and neurophysiological studies with findings at surgical exploration, to predict accurate diagnosis of thoracic outlet syndrome (TOS).
Methods: We performed a retrospective review of a prospectively maintained TOS database. All patients were clinically assessed at the Oxford University Hospitals NHS Trust between April 1997 and November 2017. Each patient was assessed as follows: 1. Clinical history 2. Clinical tests for vascular compression (Adson’s manoeuvre, Reverse Adson’s test, Wright’s hyperabduction test, Falconer’s test) and for neural compression (Roos’s test, Spurling’s test, Morley’s compression test and Tinel’s sign). 3. Radiological investigations (MRI of cervical spine and brachial plexus) and 4. Neurophysiological studies.
Results: One-hundred and twenty-five patients (n = 125) underwent thoracic outlet exploration on one-hundred and sixty limbs. There was a female preponderance in this cohort (n = 94, 75%) and age ranged from 22-75 years (mean: 41 years). At latest follow = up (minimum of 3 years), recurrences were noted in n = 18 patients (14%) and n = 99 patients (79%) reported Derkash’s full/good outcomes. Morley’s compression test was the most commonly positive test (82%), MRI demonstrated pathology in 49% of patients and nerve conduction studies were suggestive/positive in 36%. Patients with > 4 pre-operative positive clinical tests demonstrated highest Derkash’s outcome scores.
Conclusions: We identified the quadriad of 1. positive Morley’s test 2. positive NCS 3. positive findings on MRI and 4. presence of cervical rib, associated with highest diagnostic accuracy and resolution of symptoms.
Surgery for Thumb Base Osteoarthritis: The Landscape and Outcomes from the BSSH UK National Hand Registry
Miss Jennifer Lane, Mr Matthew Gardiner, Mr Jeremy Rodrigues, Professor Dominic Furniss and Mr Robert Poulter
University of Oxford
Time in programme: Thursday 3rd May 2018 10:01
Aims: To evaluate the impact of surgical subtype upon patient reported outcomes (PROMs) following surgery for base of thumb osteoarthritis (BTOA).
Methods: The UK National Hand Registry (UKNHR, formerly called the BSSH Audit Database) prospectively collects data from patients undergoing hand surgery as part of an approved national quality assurance process.
This study involved secondary analysis of fully anonymised data from the registry. Exemption from ethical approval was confirmed by University of Oxford Clinical Trials and Research Governance (CTRG) prospectively.
All procedures captured in the UKNHR from inception (May 2011) to January 2018 were included. Procedures were sub grouped by surgical intervention type, and outcome evaluated using EQ5D index, visual analogue score (VAS) and Patient Evaluation Measure (PEM) outcome measures at baseline, 3, 6 and 12 months post-operatively. Regression analyses were conducted with procedure type and gender as factors.
Results: 1298 procedures were included. Simple trapeziectomy with LRTI represented 52% and 43% of cases respectively; which was static over UKNHR’s history.
There was no significant difference in PROMs at baseline between trapeziectomy and LRTI, nor in the change in PROMs at 3 months (EQ5D index p = 0.92; VAS p = 0.34; PEM p = 0.61); 6 months (EQ5D index p = 0.15; VAS p = 0.88; PEM p = 0.66) or at 12 months post-operatively (EQ5D index p = 0.77; VAS p = 0.66; PEM p = 0.56)
Conclusions: Understanding the distribution of surgical procedures for BTOA through the UKNHR, the impact of treatment and factors associated with outcome will benefit the design of future studies in BTOA.
Use of Thiel Embalmed Cadavers in Elective Hand Surgery - Exploring Attitudes to Simulated Surgical Training
Miss Sameena Hassan, Mr Ibrahim Natalwala, Ms Kirsty Smith, Mr Paul Stanley, Mr Sanjib Majumder and Mr Richard Pinder
Hull and East Yorkshire Hospitals
Time in programme: Thursday 3rd May 2018 10:08
Aims: To assess the life-like comparability of Thiel embalmed cadavers in upper limb surgical simulation training. We also explore consultant attitudes in using simulated training to achieve indicative logbook numbers.
Methods: Seven consultant plastic surgeons and 11 speciality trainees performed three upper limb procedures [Trapeziectomy & LRTI, radial artery forearm flap (RAFF), and Extensor Indicis (EI) to Extensor Pollicis Longus transfer (EPL)]. The individual steps in each procedure were assessed using a Likert scale [1 to 4], as well as trainee confidence in performing each procedure pre- and post- cadaveric dissection training using Visual Analogue Score (VAS) [0 to 10].
Results: Following the training, trainee confidence in performing the procedures increased by a mean VAS of 2.6 (p = 0.0005) for trapeziectomy, 4.8 (p = 0.0007) for RAFF, and 2.6 (p = 0.002) for EI to EPL transfer. For trapeziectomy, trainees found more than 70% of the steps (10 of 14) to be either satisfactory or life-like (overall mean 3.2/4.0). For the RAFF, only 1 of 12 steps (identifying the septocutaneous perforator) was deemed less than satisfactory by consultants, but the overall mean was still 3.5/4.0. Both trainees and consultants found every step of EI to EPL transfer to be satisfactory or life-like with an overall mean of 3.6/4.0. Interestingly, although consultants were keen on Thiel cadavers for training, and would welcome cadaveric training into the curriculum, they did not feel it was acceptable to use this as an adjunct for indicative logbook numbers.
Conclusions: Thiel embalmed cadavers allow trainees to readily identify fascial planes, neurovascular structures, and manipulate tendons and ligaments and are hence an ideal learning resource.
Arthrodesis for Chronic Carpometacarpal Instability in Elite Boxers
Mr Feiran Wu, Mr Iain McLaughlin-Symon, Mr Ian Gatt, Dr Michael Loosemore and Mr Mike Hayton
Wrightington Hospital
Time in programme: Thursday 3rd May 2018 10:15
Aims: Instability of the carpometacarpal joints [CMCJ] is a common and potentially career ending hand injury in elite boxers. We present the outcomes of a cohort of elite boxers who presented with symptomatic chronic CMCJ instability.
Methods@: Twenty-three elite boxers, 13 professional and 10 amateur, who were unable to compete due to pain and weakness, were treated with primary CMCJ arthrodesis. A total of 64 joints were fused in 26 hands, with a mean of 2.8 joints per patient. Mean symptom duration was 14 months. All patients received non-operative intervention before proceeding to fusion (K-wires: 16 joints, screw fixation: 38 joints, speed staples: 10 joints). Autologous corticocancellous bone graft was used in all cases. All except two hands required fusion of the index and middle finger CMCJ. The mean age at surgery was 25 years.
Results: All except 3 patients (5 joints) united at a mean duration of 10 weeks. Two patients (3 joints) failed to unite and required secondary iliac crest bone grafting and fixation (screw: 1, K-wires: 2). One patient had a partial union that required further bone grafting without fixation. One patient developed dysaesthesia in the distribution of the dorsal ulnar cutaneous nerve that resolved after exploration and neurolysis. No other complications were seen.
All except two boxers returned to competition at a mean duration of 33 weeks post-operatively. All professional boxers returned to competition at a mean of 36 weeks, and remain competing 36 months following surgery. Eight amateur boxers returned to competition at a mean of 24 weeks.
Conclusion: Primary arthrodesis is a reliable and successful treatment for chronic CMCJ instability in boxers, with a low rate of complications and excellent return to competition.
Delayed Primary Flexor Tendon Repairs: How Late is Too Late?
Ms Rehnuma Hossain and Mr Shekhar Srivastava
University Hospital Coventry and Warwickshire
Time in programme: Thursday 3rd May 2018 10:22
Objective: Within the UK, most flexor tendon injuries are repaired within two weeks. There are patients who present beyond that time, and are not given the option of primary repair, as it is deemed “too late”. We present our experiences at one unit in a major trauma centre over the past5 decades of delayed primary repair of flexor tendons.
Methods: We present a series of 7 consecutive patients who had primary flexor tendon repair and discuss their outcome. A systematic review did not find any papers on this subject.
Results: Our consecutive group of 7 patients, aged 24 – 77 years presented from 14to 78 days later. There were a variety of mechanisms of injuries, though most occurred in zone1. In all cases the wound was healed or unidentifiable and the joints were mobile. Exploration of finger showed that in all these cases tendon ends could be dissected and stretched to effect a primary repair using conventional techniques. We used a four strand repair or the Kessler technique. Following repair active mobilisation was used in all cases. No repairs ruptured during therapy. 5 patients in this series achieved good to excellent results. One patient is still in therapy,while another patient had surgery. One patient with a zone 1 injury refused the offer of a tenolysis to attempt to improve DIP flexion.
Conclusion: We recommend that all patients presenting with flexor tendon injury as late as 3 months be explored soon after their presentation to see if a primary repair is possible. In many cases it will be possible to repair the flexor tendon primarily while in very late cases it may be necessary to insert a silastic rod as a first stage of 2 stage tendon reconstruction although we did not have to do it. Additional measures to facilitate a primary repair will be discussed.
Using Electronic PREMs and PROMS to Debunk the Myth of Procedures of Limited Clinical Value
Professor David Warwick, Dr Harry Akerman and Miss Olivia Halliday
University Hospital Southampton
Time in programme: Friday 4th May 2018 08:35
Background:
• Patient related outcome measures (PROMs) and Patient Relevant Outcome Measures (PREMs) allow us to assess the clinical value of the procedures we perform.
• Electronic systems increase the efficiency of data collection.
• Commissioners in England have imposed the pejorative term “Procedures of Limited Clinical Value’ (PLCV) on some hand surgery procedures.
Aim:
• To debunk the term PCLV using an electronic PROM and PREM system.
Methods: 755 Patients undergoing carpal tunnel release (CTR), trigger digit release (TDR), finger ganglion excision (FGE)’wrist ganglion excision (WGE) and fasciectomy (Fas) were assessed with the pre-operative PROMs: QuickDASH, EQ5D and VAS pain. Post-operatively at 6 months the patients were posed by email link (Cellma, Riomed. UK) the same PROMs together with three PREMs on an ordinal scale
PREM 1: “How are your problems related to your hand now prepared to before surgery?”
PREM 2: How pleased are you with the result of your surgery?”
PREM 3: “If you could go back in time, would you still have your hand operation?”
Results:
• In all procedures the EQ5D remained unchanged
• QuickDASH and VAS pain improvedin all procedures
• PREM 1: No problem atall/Much better: CTR 86%;TDR 73%;Fas 79%;FGE 88%;WGE 85%
• PREM 3: Would have the procedure again: CTR 92%;TDR 98%;Fas 83%;FGE 81%;WGE 72%
Conclusion:
• The EQ5D is not sensitive enough to be used as a PROM.
• QuickDASH and PREMs demonstrate the clinical value of various hand surgery procedures
• The term PLCV is not based on evidence. One might conclude that the term is used to mask health care rationing.
Consent: Supported Decision Making – Are We Compliant?
Mr Abdulla Ibrahim, Mr Stephen Ali and Mr Thomas Wright
Southmead Hospital
Time in programme: Friday 4th May 2018 08:39
Aim: Following the Montgomery case there has been a move from traditional paternalistic approaches of consent towards those of a patient-centered focus. Here, we evaluate the consent process within the plastics trauma setting and discuss beneficial educational interventions.
Method: A prospective audit cycle was undertaken of all acute adult plastic surgery patients that underwent surgery over eight weeks spanning February and September 2017 within a major trauma centre. All clinical notes and consent forms were reviewed. Within this period, educational interventions were undertaken to improve compliance against the Royal College of Surgeon’s standards. Exclusions included missing notes/consent, and patients who were unable to consent or declined surgery.
Results: 186 patients were included in the audit cycle; 102 in the first, and 84 in the second loop. Following intervention, the following standards improved; black ink use (100% vs 92%), legibility (100% vs 92%), avoiding abbreviations (81% vs 74%), consent discussion (65% vs 9%), and confirmation of consent (18% vs 4%). Whilst all cases had correct patient demographics, no patients received a copy of their consent.
Conclusions: In the current healthcare climate, surgeon education can help meet the necessary legal and regulatory requirements and protect patients’ rights to make informed decisions regarding their treatment.
The Impact of Education and Guideline Implementation on Antibiotic Prescribing in Acutely Infected or Contaminated Hand Wounds and Bites
Dr Alice Wignall, Dr Gavin Barlow and Mr Richard Pinder
Hull Royal Infirmary
Time in programme: Friday 4th May 2018 08:43
Aims: Inappropriate prescribing contributes to antibiotic resistance, one of the three most important public health threats. We recently developed consensus antibiotic guidelines for use in acutely infected or contaminated hand wounds and bites. This study aimed to assess the impact of the implemented guidelines on antibiotic prescribing.
Method: A multidisciplinary collaboration developed antibiotic guidelines to align prescribing with local and national stewardship and resistance agendas. Before implementation, data on all patients presenting with traumatic or infected hand wounds over a 2-week period were gathered. Following education and implementation, further data were collected.
Results: Data were analysed for 110 patients (51 before, 59 after). Following education and implementation, correct decisions regarding indication for antibiotics increased in both the referring centres (RC) (59% to 69%) and the specialist trauma clinic (STC) (71% to 80%). Adherence with guideline antibiotic recommendations rose in both the RC (28% to 60%) and the STC (39% to 67%). This resulted in a reduction in the prescription of broad-spectrum antibiotics.
Conclusions: Following implementation there was a notable decrease in broad-spectrum antibiotic prescribing. While education and guidelines can help ensure appropriate narrow spectrum antibiotics are prescribed, there is room for further improvement with ongoing education and feedback necessary to ensure improvement is sustained.
Management of Paediatric Trigger Thumb (PTT) – Results From a UK-Wide Survey of Current Practice
Miss Jessica Harvey and Mr Chris Bainbridge
The Pulvertaft Hand Centre, Royal Derby Hospital
Time in programme: Friday 4th May 2018 08:47
Aims: The BSSH paediatric SIG endorsed our aim to establish the normal UK management of paediatric trigger thumb (PTT). Secondly we aimed to assess the feasibility of a multi-centre trial of conservative management.
Methods: An online survey was distributed to all BSSH members in January 2018.
Results: 194 BSSH members responded, 117 of these treat PTT. These included 63 orthopaedic and 41 plastic hand surgeons. Primary management was conservative for 50% and surgical for 35%. The remaining 15% nuanced their treatment depending on the age of presentation.
48% declared they would monitor for up to 6 months, 29% for up to 1 year and 19% for up to 2 years. We had 88 free-text responses expanding on the reasoning for their primary management choice and the key points made were the importance of involving the parents in the decision making. 56% were interested in a multi-centre trial.
Conclusions: There is a lack of consensus regarding management of this condition. Half of the surgeons recommended conservative therapy but most did so for a short period of time (6-12 months) with shorter periods in older patients.
The literature (USA and Korea) suggests that 80% of PTT cases will improve to grade 0 with up to 60 months of conservative management. We believe a pragmatic trial of conservative management for paediatric trigger thumb is feasible to establish the duration and outcome of conservative management in the UK and the development of suitable information for parents.
Apert's Hand Revisited: A New Classification System
Mr Hazem Alfeky and Professor Paul McArthur
Alder Hey Children's Hospital
Time in programme: Friday 4th May 2018 08:51
Aim: Acrocephalosyndactyly or Apert’s hand is a rare syndrome occurring once in every 45000 live births. It has been well described and classified by Upton into 3 types based on the configuration of the first web space with type 3 as the most severe form. The challenge in Acrocephalosyndactyly is often more than a first web space issue. The pattern of the proximal and distal synostosis is one of the key factors that determines the management and outcome.
Patients and methods: 42 Apert’s hands have been assessed and managed within MDT setting. All hand procedures were performed by a single surgeon over a period of 10 years. A new proposed classification system is presented. Follow up period ranged between 4 and 13 years. Outcomes were assessed by the hand therapy team as well as patient and family satisfaction.
Results: The difficulty in operating on Apert’s hand, and consequently the predicted outcomes, relates more to the degree and level of the synostosis, status of MCPs and absence or coalescence of the osseous elements of the hand more than the status of the first web space.
A new classification system, based on clinical and the x ray findings, is proposed to help planning and predicting the outcomes of the surgery in Apert’s hand, in particular a realistic prediction of number of digits achievable.
A Palmar Bilobed Flap for the Correction of Radial Dysplasia
Ms Ciara Deall, Professor Henk Giele and Ms Roisin Dolan
John Radcliffe Hospital
Time in programme: Friday 4th May 2018 08:55
Aims: The correction of radial dysplasia can be performed using a palmar bilobed flap that leaves less visible scar than a dorsal approach.
Methods: This novel modification of the David Evans dorsal bilobed approach is presented, demonstrating the excellent access, re-distribution of the ulnar skin, and reduced scar visibility. A review of 20 cases performed through the palmar bilobed approach is presented. The aesthetic visibility of the palmar approach scar was compared to the scar in 20 previous cases performed through the dorsal bilobed or dorsal curved incision by collating interobserver scores in blinded post-operative photos of the cases.
Results: Successful completion of all radial dysplasia corrections either radialization or centralizations, with successful healing of all bilobed flaps. Two cases out of twenty palmar bilobed flaps had tip necrosis of one of the flaps requiring dressings until healed, but no operative intervention was required. All observers noted the lack of visible scarring on dorsal views of the wrist in the palmar bilobed approach compared to the visible scars with the other approaches.
Conclusion: We describe a novel modification of the Evans dorsal bilobed incision for radial dysplasia correction that reduces the visible scarring and improves the palmar access.
Poor Surgical Outcomes in Camptodactyly Using Total Anterior Teno-Arthrolysis or Osteotomies
Miss Michelle Baker, Miss Roisin Dolan and Mr Henk Giele
John Radcliffe Hospital
Time in programme: Friday 4th May 2018 08:59
Objectives: The surgical management of camptodactyly is poorly described with little data to support a variety of surgical techniques. The aim of this study is to correlate functional results of total anterior teno-arthrolysis (TATA) or osteotomies for camptodactyly correction.
Methods: We performed a retrospective review of all patients presenting consecutively to a tertiary centre for paediatric hand surgery for the surgical managment of camptodactyly. All patients were assessed by the senior author at the John Radcliffe Hospital between 1997 and 2012. Duration and severity of symptoms, previous failed treatment includin splinting and surgery, x-ray changes were considered when deciding the optimal procedure for each patient. Starting mean contracture, improvement of contracture (extension angle), loss of flexion and complications were assessed.
Results: 28 patientsunderwent TATA or osteotomies for camptodactyly correction. 16 had an isolated little finger camptodactyly. The mean starting contracture was 81o (60-100o). 24 (86%) had an improvement in extensionangle but 22 (79%) had a loss of flexion. 8 (29% patients (or parents of patients) found there was no improvement in camptodactyly. Complications were common including 6 with pinsite infection, 2 wound infection, 4 wire loosening, 2 bone loss, 8 bone stiffness.
Conclusions: Camptodactyly is a complex mulitfactoral problem with a range of affected biology. Our outcomes are worse than in the reported literature, but mean starting contracture was larger. There's an observed change in function from a predominately flexor grip to greater extensor strength in the operated finger. A single surgical solution is not suitable, and an indivisualised approach must be considered.
The Outcome of Dermofasciectomy for Dupuytren’s Disease – A Systematic Review and Comparison with Results From our Regional Hand Unit
Miss Olivia Sharp and Wing Commander Ankur Pandya
Queen Alexandra Hospital
Time in programme: Friday 4th May 09:03
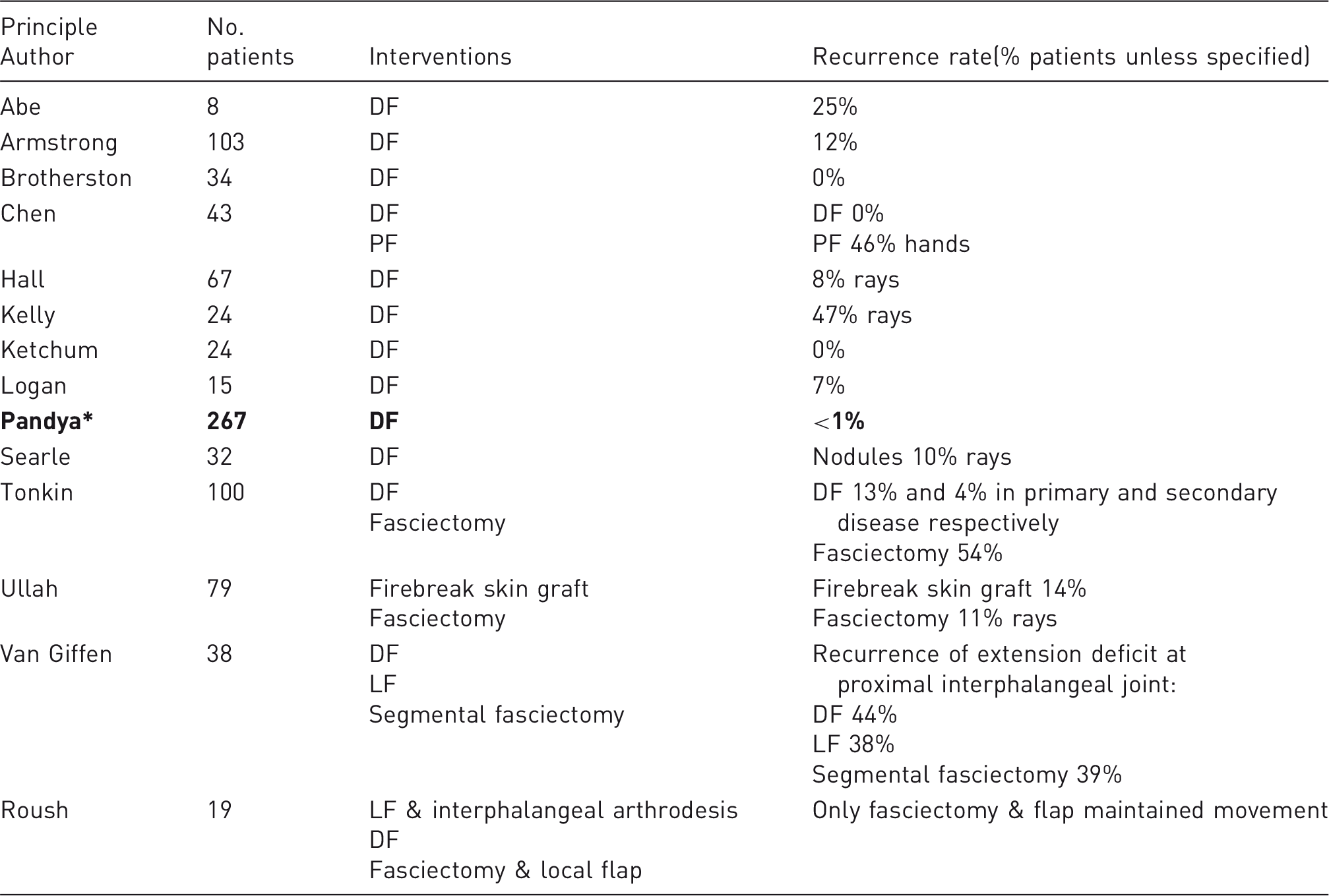
Aims: This systematic review evaluates the rates of recurrence and complications after dermofasciectomy.
Methods: Databases were searched and a PRISMA chart created. 56 non-duplicate citations were screened, of which 13 met our inclusion criteria. Comparison was made with our local results.
Results: See table 1. There was considerable variability in scoring systems, definition of recurrence and reporting of complications. Recurrence rate and follow up ranged from 0- 47% and 24 - 156 months, respectively.
Conclusion: Due to heterogeneity in the definition of recurrence and contrasting results between studies, no definite conclusion regarding the superiority of dermofasciectomy was possible. In our unit, the recurrence rate is low at <1%. We emphasise the use of 1) a minimum data set and 2) both patient reported- and objective measurements of hand function in future studies.
The Anatomical Relationship Between the Lunate and Distal Radius: An Analysis of Computed Tomography Scans of the Normal Wrist
Miss Adeline Clement, Dr Duncan Stickle and Professor Alan Johnstone
Aberdeen Royal Infirmary
Time in programme: Friday 4th May 2018 09:07
Aim: The aim of the study was to use CT scanning to determine the anatomical relationship between the lunate and distal radius as previously identified in MRI studies, enabling assessment of distal radius fracture reduction where inadequate radiographs are taken.
Details of included studies.
Principle Author
No. patients
Interventions
Recurrence rate(% patients unless specified)
Abe
8
DF
25%
Armstrong
103
DF
12%
Brotherston
34
DF
0%
Chen
43
DF PF
DF 0% PF 46% hands
Hall
67
DF
8% rays
Kelly
24
DF
47% rays
Ketchum
24
DF
0%
Logan
15
DF
7%
Pandya*
267
DF
<1%
Searle
32
DF
Nodules 10% rays
Tonkin
100
DF Fasciectomy
DF 13% and 4% in primary and secondary disease respectively Fasciectomy 54%
Ullah
79
Firebreak skin graft Fasciectomy
Firebreak skin graft 14% Fasciectomy 11% rays
Van Giffen
38
DF LF Segmental fasciectomy
Recurrence of extension deficit at proximal interphalangeal joint: DF 44% LF 38% Segmental fasciectomy 39%
Roush
19
LF & interphalangeal arthrodesis DF Fasciectomy & local flap
Method: The reformatted images of computed tomography (CT) scans of 19 normal wrists were examined firstly in the central/neutral axis and thereafter in increments of 5°of the central axis up to 30° in both directions from the central axis on the true lateral. To obtain a measurement, a line is drawn continually from the dorsal cortex of the distal radius to the carpal region. Then the distance from the superior pole of the lunate to this line is measured (SL-DC). The lunate height (LH) is measured and the SL-DC: LH ratio calculated. The ratios were calculated for each degree of rotation by two individual observers, the interobserver reliability calculated using a Bland-Altman plot and a repeat-measures ANOVA analysis applied to the results.
Results: The superior pole of the lunate was always volar to the dorsal radial line through the range of ±30° which is consistent with the previous MRI studies. There was a good degree of interobserver reliability on the full dataset, as well as the isolated data, with only 4% of the data points outside the limits of agreement.
Conclusion: The results reaffirm the hypothesis that the SL-DC relationship is maintained through a range of rotation up to 30° away from the true lateral view. In addition, the lunate reliably sits below the dorsal cortical line of the distal radius, echoing the results of previous work on the topic. This allows for better assessment of distal radius fracture reduction in the presence of poorly obtained lateral plain radiograp.
Association Between Loss of Finger Extension and Patient Reported Outcome Measures (PROMs) in Dupuytren’s Contracture in the HAND-1 Trial
Mr Wei Tan, Professor Tim Davis, Mrs Trish Hepburn, Mrs Kirsty Sprange, Mrs Eleanor Harrison, Ms Amanjeet Dahaley, Mr Gregory McConaghie, Miss Alexia Karantana, Dr Nicola Mills and Professor Alan Montgomery
University of Nottingham
Time in programme: Friday 4th May 2018 09:11
Background: Correction of extension deficit is used to determine the success of Dupuytren’s surgery, but it is uncertain how well this reflects patients’ perceptions of outcome.
Aim: To assess the association between changes following treatment in a) linear loss of active finger extension (LLAE); b) angular finger deformity (AFD); and c) four patient reported outcome measures (PROMs).
Methods: Patients with a Dupuytren’s contracture >30° in one or more finger(s) treated by either limited fasciectomy or needle fasciotomy as part of a randomised trial, underwent linear and angular measurements of finger extension loss and completed 4 PROMs (URAM, MYMOP, DASH, PEM) pre-operatively and 6 month post-surgery. LLAE measurements were assessed via a bespoke device which maintained the hand in a standard position; the AFD measurements were obtained using a goniometer.
Results: Postoperative changes in LLAE and AFD were moderately correlated (CC = 0.549). Both change in LLAE and AFD correlated better with the MYMOP and URAM, than with the DASH and PEM.
Correlation coefficients
MYMOP
URAM
PEM
DASH
LLAE (n = 29–30)
0.580
0.526
0.378
0.255
AFD (n = 40–42)
0.598
0.507
0.382
0.387
Conclusion: Linear loss of extension offers an alternative to angular measurement of finger extension. Both were associated with changes in PROMs, but the observed associations were not strong, and may result from pain, numbness or stiffness not captured when measuring joint angles.
Trial Registration: SRCTN11164292
Funding: NIHR RfPB (PB-PG-0613-31083). The views expressed are those of the author(s) and not necessarily those of the NHS, NIHR or Department of Health.
The Scratch Collapse Test: A Systematic Literature Review
Dr Urška Cebron and Dr Catherine Curtin
Stanford University
Time in programme: Friday 4th May 2018 09:15
Aims: The ‘Scratch Collapse Test’ (SCT) has emerged as a new provocative test to assist in the identification of the level peripheral nerve compression. This study aims to review the data on the reliability of the SCT as a diagnostic test for entrapment neuropathy through a systematic literature review.
Methods: A literature search of all years was conducted using PubMed and Google Scholar databases. Case reports, articles not citing primary data and articles in languages other than English, Spanish and Italian were excluded. 10 publications matched our criteria: 1 in Spanish and 9 in English, and all were included in the review.
Results: 3 of the papers studied the SCT as a diagnostic test exclusively for ulnar nerve entrapment, 5 of them studied it as a diagnostic test for median nerve entrapment, 1 looked at it to diagnose both ulnar and median nerve entrapment and 1 paper examined the SCT as a tool to diagnose peroneal nerve entrapment.
We found that the PPV and specificity values were high in all studies: between 0.71 and 0.99 and 0.6 and 0.99 respectively, while other values were very variable among studies: individual NPV values ranged from 0.15 to 0.92 and the sensitivity values ranged from 0.24 to 0.77
Conclusions: The SCT is a potentially useful tool in the clinical diagnosis of entrapment neuropathy as it can be performed on most peripheral nerves. However, SCT is one tool of many and should not be used as a sole diagnostic method of a compression neuropathy but as an addition to a surgeon’s diagnostic repertoire. Importantly, there is a paucity of studies on the reliability of the SCT as a diagnostic tool. The biggest hurdle separating the SCT from mainstream use is its difficulty to be learned and correctly performed by novice users.
The Free Vascularized Pedicled Nerve Functioning Muscle Transfer: A Novel Concept for Brachial Plexus Reconstructionn
Ms Roisin Dolan and Professor Henk Giele
John Radcliffe Hospital
Time in programme: Friday 4th May 2018 09:25
Aims: Free functioning muscle transfers are limited by the availability and regeneration of neural donors.We explore the novel concept of a free vascularized but pedicled nerve muscle transfer (using the rectus abdominus muscle) that overcomes the need for neural regeneration and adds to the reconstructive options in brachial plexus pathology.
Methods: Anatomical dissection of the nerve and blood supply of six rectus abdominus muscles in three cadavers showed that it was possible to elevate the rectus abdominus on its intercostal nerve supply and dissect these to the mid-axillary line allowing the muscle to be pedicled on its nerve supply to the arm. We present five clinical cases of reconstruction of elbow flexion in four cases of complete traumatic brachial plexus avulsion injuries (C5-T1) and one case of poliomyelitis.
Results: The cadaveric study demonstrated that neural dissection of the intercostal nerves supplying rectus abdominus was possible to the axilla, and therefore transferable. Five clinical cases were performed using this technique. There were no perioperative complications. Surgical outcomes demonstrated good elbow flexion with M4- power and shoulder stability regained in 4 out of 5 cases. Two patients developed post-operative abdominal wall hernias secondary to denervation requiring subsequent mesh repair.
Conclusions: We describe a novel reconstructive concept of a free vascularized pedicled nerve reconstruction adding to our armamentarium in the reconstruction of brachial plexus pathology.
Efficacy of Ultrasound vs. Fluoroscopic Guided Steroid Injections of Small Joints in the Hand: Patient Pathways, Clinical Outcomes and Cost
Miss Vi Vien Toh, Miss Victoria Teoh, Dr Muthusamy Chandramohan and Mr Zakir Shariff
Bradford Teaching Hospitals NHS Trust
Time in programme: Friday 4th May 2018 09:29
Aim: To perform a cost analysis and service evaluation of patients receiving steroid injections of small joints of the hand, comparing an ultrasound-assisted technique, performed by a musculoskeletal radiologist (non-surgical group) and fluoroscopic-guided injection performed by hand surgeons in an operating theatre (surgical group). Secondary outcome measures included elapsed time from point of ‘decision to treat’ to the delivery of treatment and patient experience.
Method: A retrospective evaluation of activity across a single financial year, Healthcare Resource Group codes and tariffs for both study arms was conducted through data derived from an electronic radiology outpatient booking system and theatre procedure logs.
Results: 68 patients involving 72 joints were identified in the non-surgical group. 15 patients involving 18 joints were identified in the surgical group. The cumulative tariff of steroid injections performed surgically was significantly greater than that performed in the radiology department. The average time from point of ‘decision to treat’ to the delivery of treatment was 82 days (23-216) in the surgical group compared to 66 days in the non-surgical group (30-97).
Conclusion: Ultrasound-assisted steroid injections performed in the outpatient setting currently provide a better patient experience and can be a solution to surgical waiting times for elective hand procedures. It offers significant cost savings, in a climate of a resource-depleted NHS.
Postcode Lottery - Do Commissioning Groups Differ in Funding Elective Hand Surgery?
Miss Kirsty Smith and Mr James Haeney
Hull Royal Infirmary
Time in programme: Friday 4th May 2018 09:33
Aims: To determine if there are regionaldifferences in CCG funding of elective hand surgery.
Methods: Welooked at each of the 207 English CCG commissioning policiesto review publishedcriteria for routinely commissioned elective hand surgery. We specifically reviewed funding availability for surgical treatment of Carpal tunnel syndrome, trigger digit, Dupuytren's andganglion.
Results: Referral criteria forsurgical release oftrigger finger was the most consistent area with the majority of CCGsprovidingfunding for a fixed flexion deformity or after failed conservative management of symptomatic triggering.However the type and length of conservative management differed greatly.
Referral criteria forDupuytren's diseasevaried greatly. Some CCGs allow treatment of any Dupuytren's whereas others specify angles of joint contracture.
MostCCGs fund carpal tunnel decompression in severe disease with muscle wasting and sensoryblunting, but availability of treatment for less severe disease is more variable. The length and typeof recommended conservative treatment formoderate symptomsranged considerably.
Ganglion surgery is not routinely funded by the majority of CCGs. In some areas treatment is available on an IFR basis only whereas other CCGs publish specific criteria for mucous cysts, seed ganglia and functional impairment.
Conclusions: Significant differences exist in the regional CCG funded availability of elective hand surgery in England.
Hand Trauma in England: An Analysis of HES Data
Mr Oliver Manley, Mr Justin Wormald and Prof Dominic Furniss
Stoke Mandeville Hospital
Time in programme: Friday 4th May 2018 09:37
Introduction: Hospital episode statistics provide a method to study changes in the incidence of hand injuries over time that can be used to target resources and identify research targets.
Methods: We analysed freely available hospital episode statistics between 1998 and 2014 for hand and wrist fractures, tendon, nerve and blood vessel injuries, nail bed injuries, and traumatic amputations. The incidence of each injury type was calculated by age group using population data from the Office for National Statistics.
Results: There were a total of 845890 hand injuries recorded over the 17-year period studied, of which 76% occurred in men. The incidence of hand injuries each year increased from 70 to 110 per 100 000. Hand fractures were the most common injury, 51% of the total, and the injury with the greatest rise in incidence. Notably, the incidence in the over 75 age group doubled over the period studied. There was also a large rise in the number of nail bed injuries, particularly in the paediatric population, where the incidence tripled.
Conclusion: This study describes the trends in burden of hand trauma in England, and can be used to predict future resource need for hand surgery services. The large rise in hand fractures in the elderly and of nail bed injuries in children are notable and require further study.
Minimally Invasive Reconstruction of the Anterior Oblique and the Dorsoradial Ligaments of the Painful Subluxated Carpometacarpal Joint of the Thumb
Professor Ethan Wiesler, Dr David Luo and Dr Mark Warburton
Wake Forest Univ., Baptist Medical Center
Time in programme: Friday 4th May 2018 09:41
The purpose of this study is to assess the success of a new minimally invasive surgical technique that functions to anatomically restore the CMC joint using palmaris longus (PL) tendon autograft to augment the anterior oblique ligament (AOL) and dorsoradial ligament (DRL).
We retrospectively reviewed 45 patients with subluxated CMC joints of Eaton stage I or II who were treated with preservation of trapezium andautologous PL tendon transfer. Pre and post op mean grip and pinch strength were assessed in a standard manner with Jamar dynamometer, and DASH questionnaire scores recorded. Pre and post-op stress radiographs were compared to calculate changes in joint stability as evidenced by the CMC subluxation ratio. Descriptive statistics including mean values with standard deviation were performed on all data collected.
In all 45 patients, grip improvedfrom pre to post-op, with measurements increasing from 38 and 11.7 pounds to 55 and 14.7 pounds respectively. CMC subluxation ratios decreased from 0.69 to 0.46 after surgery, showing enhanced stability of the CMC joint. All patients reported significant subjective improvement in pain after surgery and were able to return to previous levels of work. A decrease in mean DASH scores from 42 pre-op to 10.6 post-op were seen among all patients.
We consider this minimally invasive reconstruction of the CMC joint to provide satisfactory outcomes in patients with Eaton stage I or II CMC OA as evidenced by improved subjective and functional results. Given its minimally invasive nature, future treatment options such as a conversion to LRTI or a joint replacement arthroplasty are still available if needed.
Antibiotics in Hand Trauma: Cutting Down the Cost and Maximising Patient Safety
Dr Bismark Adjei, Mr Hazem Alfeky, Miss Lucy Homer, Miss Salma Mohamed, Mr Irfan Khan, Mr Christian West and Mr David Bell
Whiston Hospital
Time in programme: Friday 4th May 2018 09:45
Introduction and Aims: The World Health Organisation recently raised an alarm concerning moving towards a world without effective antibiotics (The post-antibiotic era) urging medical specialities to review their practice and, where appropriate, change them to stem the tide. Prophylactic antibiotics are frequently used by plastic surgeons in hand trauma as a prophylaxis. However, there is no solid evidence for that. The aim of this audit is to review the current practise and measure it to the guidelines.
Material and Methods: A review of 300 hand soft tissue laceration cases were included. All open fractures and complex soft tissue injury were excluded. The antibiotics prescription was measured against the guidelines and the recommendations of a two recent meta-analysis studies to define the role of prophylactic antibiotics in upper limb lacerations.
Results: In two recent meta-analyses, Jennifer Lane et al. and Murphy et al, showed that prophylactic antimicrobial use has no significant effect on the infection rate compared to placebo or no antibiotics in patients with small soft hand lacerations. Our current practise shows that there is a trend to prescribe prophylactic antibiotics where there is no clear indication.
Conclusion: Not withstanding current evidence, there is a trend to routinely supply simple hand laceration patients with prophylactic antibiotics. There is a need to review our practise and define a clear guidance on the role of antibiotic prophylaxis in hand trauma patients.
Rapid Microbial Diagnosis in Hand and Upper Limb Infections
Dr Andrew McKean, Mr Shakeel Rahman, Mr Peter Macneal and Mr Maxim Horwitz
Chelsea and Westminster Hospital NHS Foundation Trust
Time in programme: Friday 4th May 2018 09:49
Aims: Microbiology diagnostics have benefited following advancements in multiplex PCR technology, which is currently available to provide pathogen diagnosis and antimicrobial sensitivities within ninety minutes. We aimed to review the existing evidence for multiplex PCR in clinical microbiology and to discuss its potential role in managing patients with hand & upper limb infections at our tertiary hand unit.
Methods: Comprehensive literature review was undertaken using Medline and EMBASE. Search terms included: ‘multiplex PCR’, ‘hand surgery’, ‘hand infection’, ‘upper limb infection’ and ‘clinical microbiology’. Relevant literature was then identified and considered.
Results: There is no published literature examining the use of multiplex PCR in patients with hand & upper limb infections. Multiplex PCR has been used in other specialties including: gastroenterology, respiratory, neurology, trauma & orthopaedics and burns. Related literature has shown benefits in time to results of antimicrobial sensitivities in comparison to traditional culture techniques. Utilising such technology in severe hand & upper limb infections has clear clinical implications: quicker identification of resistant organisms and administration of appropriate antibiotic therapy, reduced inpatient stay and less return to theatre.
Conclusions: There is no published literature considering the role of multiplex PCR in patients with hand & upper limb infections. Following the introduction of this technology at our unit, we shall publish our audit data on the change and improvement to rapid diagnosis and its impact on clinical outcomes. The benefits of using multiplex PCR in this setting are clear and need to be explored further in all specialities.
Hand Trauma Service at a Rural District General Hospital. Challenges of Meeting the BSSH 2007 Hand Trauma Standards
Mr David Izadi, Mr Alasdair Barrie, Mr Kevin Williams, Mr Vikram Devaraj, Mr Andrew Watts and Mr Christopher Wallace
Royal Devon and Exeter Hospital
Time in programme: Friday 4th May 2018 09:53
Aims: In 2007, the British Society of Surgery of the Hand established minimum standards for hand units treating patients with hand trauma in the UK. An audit of the hand trauma service at the Royal Devon and Exeter Hospital in 2016 demonstrated a gross failure to comply with these standards. We thus sought to introduce new measures to improve the service.
Methods: The new measures implemented in 2016 restrictedA&E’saccess to week dayhand trauma clinics andinstead introduced a virtual triage clinic run by the on-call consultant every morning. The hand trauma clinic was relocated next to the hand therapy clinic; new hand trauma patients needing hand therapy were seen on the same day as their hand trauma clinic appointment; new patientscould be placed directly with hand therapists; dedicated hand trauma onlyday case operating lists were established. One year after the first hand trauma clinic audit, the same audit was repeated for the same period in 2017.
Results: Following implementation of the above changes, 15 additional new, and 15 additional follow-up patients were seen in the hand trauma clinic each month, and 13 additional hand trauma patients were operated on each month, increasing thehand trauma generated incomeby £29,000 per month. There was a 50% improvement in the number of patients seen in the hand trauma clinic within 5 days of their referral, a 35% improvement in the number of patients waiting less than 5 days for their surgery.
Conclusions: This audit loop demonstrates how the introduction of a series of simple interventions can significantly improve the service delivered to hand trauma patients with a significant increase in the revenue generatedby this service.Weaim to re-audit this service again to continue making further improvements.
Current Opinions Regarding the Management of Pyogenic Flexor Tenosynovitis
Miss Laura Bolton and Mr Chris Bainbridge
Nottingham City Hospital
Time in programme: Friday 4th May 2018 09:57
Aims: We aim to assess the management of pyogenic flexor tenosynovitis(PFT) amongst attendees at the British Society for Surgery to the Hand (BSSH) meeting in order to guide further research.
Method: An electronic survey was distributed to attendees at the BSSH meeting. The survey was compiled by a group of hand surgeons and piloted in a tertiary unit prior to dissemination. Questions focused on three clinical vignettes describing PFT of increasing severity. Responses were analysed using Surveymonkey.
Results: Almost 50% of respondents would proceed to surgical decompression and washout even in patients diagnosed within a few hours of onset. This increased to 88% when treating a patient who had symptoms for several days and failed a trial of oral antibiotics. The majority of respondents would not consider flexor sheath aspiration regardless of clinical scenario. For those advising surgery, the majority felt this should be performed within 24 hours in all three scenarios. More than 50% would advocate active mobilisation either immediately or as soon as possible regardless of severity of the infection. Almost all of the respondents would use either general or regional anaesthesia for the procedure and a 2 incision technique with catheter irrigation.
Conclusions: Our survey demonstrates huge variation in the management of pyogenic flexor tenosynovitis. Advice from the pre-antibiotic era of emergent surgical debridement continues to be followed; a proportion continue to use an open technique. The importance of immobilisation is stated throughout the literature but many advocate early active mobilisation. Further study into the management and outcomes of PFT is required to establish best practice for this potentially devastating condition.
Defining Displacement Thresholds for Surgical Intervention for Distal Radius Fractures – A Delphi Study
Mr Nick Johnson, Dr Paul Leighton, Mr Distal Radius Study Group, Professor Charles Pailthorpe and Dias Joseph
University Hospitals of Leicester
Time in programme: Friday 4th May 2018 10:01
Aims: This study had three aims; to identify which radiographic parameters in distal radius fractures are clinically important; quantify the threshold of displacement at which intervention should occur and investigate which patient factors influence the threshold of the decision to intervene.
Methods: A modified three round Delphi study was carried out and responses were qualitatively analysed.
The panel was composed of 3 groups of national and international expert surgeons:
• Hand and wrist surgeons.
• Trauma surgeons.
• International researchers
46 participants initially agreed to take part. 43 completed the first round and all then completed three rounds.
Participants were asked questions based around case vignettes in patients of three ages (38, 58, 75 years).
Results: For all age groups ulnar variance was ranked as the most important extra-articular parameter followed by dorsal tilt, step was ranked as the most important intra-articular parameter.
Agreed thresholds were the same for all parameters for patients aged 38 and 58. Surgeons would intervene in patients aged 38 and 58 with +2 mm ulnar variance, 10 degrees dorsal tilt, 2 mm step and 3 mm gap. In patients aged 75 the agreed thresholds were 20 degrees dorsal tilt, 3 mm step and 4 mm gap, consensus was not achieved for ulnar variance.
Conclusions: Our findings provide useful advice about which parameters should be measured and radiographic thresholds for intervention. These thresholds may then be modified depending on important patient factors. This information can help guide clinicians with management decisions and reduce variation.
Scaphoid Fractures - Not Just for the Young and Reckless
Mr Adam Sykes, Mr Nick Riley, Mr Tamas Szabo, Mr Ian McNab and Mr Christopher Little
Nuffield Orthopaedic Centre
Time in programme: Friday 4th May 2018 10:05
Aims: While previous studies have found scaphoid fractures to be injuries of young, male adults, we have noted an increasing proportion of older patients presenting with such injuries. We aimed to determine the age distribution of these patients, and to evaluate potential causative factors.
Methods: We prospectively collected patients with scaphoid fractures over a two year period for analysis of their demographics, mechanism of injury and imaging. The sub-group of patients over the age of 50 was compared to age- and gender-matched controls who had sustained distal radius fractures to look for potential differences in the mechanism of injury, bone density, and extent of carpal degenerative change.
Results: 198 scaphoid fractures were identified in 153 male and 45 female patients. The age range was 15-84 years (mean age 35 years); the mean age in females of 47 years (range 16 to 84 years) was significantly higher than in males (mean 31 years, range 15 to 76 years, p < 0.00001, Mann Whitney U test). 41 fractures occurred in patients over the age of 50 (21%).
There was no difference in the extent or distribution of pre-existing carpal degeneration, the energy of injury, or the patients' bone density (measured by the metacarpal index) when comparing patients over 50 years old with scaphoid fractures with control patients who had fractured their distal radius.
Conclusions: Scaphoid fracture should be suspected in patients who sustain a wrist injury irrespective of their age to avoid missing a scaphoid fracture. We were unable to identify any particular factors in patients over 50 years old to explain the observed increased scaphoid fracture frequency in our cohort in comparison with the low frequency reported in historical studies.
The NeuFlex Metacarpophalangeal Joint Implant: Does it Fracture and if so Where? An Analysis of 30 Retrieved Implants
Professor Grey E B Giddins and Professor Tom Joyce
RUH
Time in programme: Friday 4th May 201810:09
Aims: To better understand the reasons for implant failure we assessed explanted NeuFlex metacarpophalangeal (MP) joint prostheses to identify position of fracture.
Methods: Following revision MP joint surgery for symptomatic failure the implants were cleaned and photographed. The position of fracture, if any, was noted. Patient demographics were recorded.
Results: Thirty NeuFlex MP explants were analysed. Seven (23%) were not fractured. Eleven explants (37%) had fractured at the hinge; nine (30%) had fractured at the junction of the distal stem and hinge; and three (10%) had fractured at both the hinge and distal stem. Age at revision ranged from 43 to 81 (median 58) years. Time in vivo ranged from 6 to 120 (median 58.5) months. Discolouration of some explants had occurred; other explants appeared to show no colour change.
Conclusions: This appears to be the first report of the position of fracture of NeuFlex explants. It is also the largest report of silicone arthroplasty explants. The majority (77%) had fractured. Nine (30%) NeuFlex explants had fractured at the junction of the distal stem and hinge; the typical position seen with Swanson and Sutter/Avanta MP joint explants. Eleven (37%) fractured across the hinge; this has not previously been reported although has been seen in in vitro testing. Intriguingly, 3 (10%) NeuFlex explants suffered fractures both at the hinge and at the junction of the distal stem and hinge which has also never been reported previously.