
Abstract

Dear Sir,
Because of the similarities between the anatomy of the hand and foot, toes are suitable donors for reconstruction of finger defects (Adani and Woo, 2017; Balan, 2016; Graham et al., 2016). Here, we report the reconstruction of severe composite tissue defects of the hand using a composite second metatarsal flap.
A 22-year-old man was transferred to our hospital, 24 hours after having his left hand severely injured in a car accident. Initial wound assessment indicated that the abductor pollicis brevis, flexor pollicis brevis and opponens pollicis muscle were missing. The palmaris longus, flexor pollicis longus and flexor carpi radialis tendons, as well as the flexor digitorum superficialis tendon of the index finger, flexor retinaculum and median nerve were partially damaged. Almost 2/3 of the first metacarpophalangeal joint, 4/5 of the first metacarpal, most of the trapezium, 2/3 of the scaphoid and part of the radial styloid were lost. The metacarpophalangeal joint, carpometacarpal joint and wrist joint had been fixed with Kirchner wires at a local hospital.
Vacuum sealing drainage treatment was administered until the bruises on the finger pulp and palm were healed. The reconstructive surgery was performed 23 days after injury. A composite second metatarsal flap was designed and outlined on the left foot (Figure 1(a)). The entire second metatarsal, second toe, dorsalis pedis artery and saphenous vein were raised as a flap (Figure 1(b)). The donor site was closed with a skin graft from the abdomen.
(a) Flap design; (b) dissected flap and the recipient site; (c) reconstruction diagram.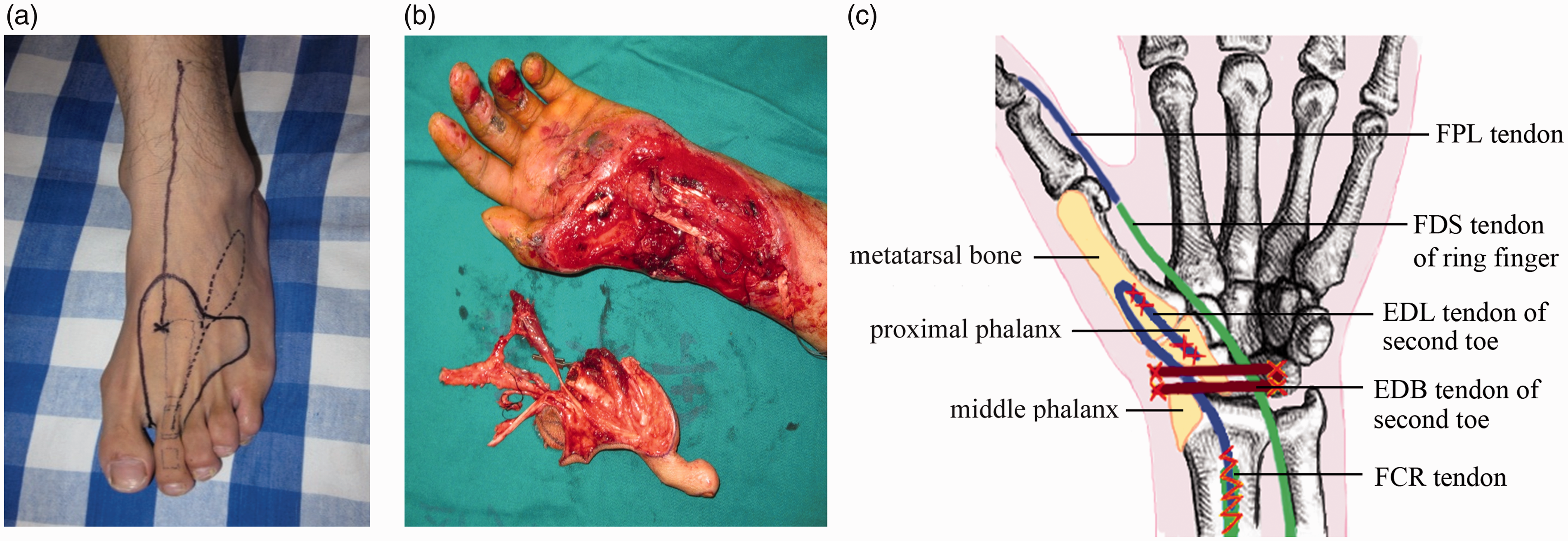
The flap was placed inversely to the recipient site (Figure 1(b)), and the reconstruction work took place as follows.
Joint reconstruction. Part of the metatarsal and 1/3 of its cortex was excised with an electric saw and then attached to the remnant metacarpal inversely by wire suture. The proximal phalanx of the toe was fixed to the remnant scaphoid using a Herbert cannulated screw. The middle phalanx was fixed on radial styloid with cortical bone anchors, and the distal phalanx was amputated (Figure 1(c)). Tendon reconstruction. The proximal end of extensor digitorum longus tendon of the toe was turned back and attached to the flexor carpi radialis tendon using a Bunnell suture. The extensor digitorum brevis tendon of the toe was used to repair the injured flexor retinaculum, and the flexor digitorum superficialis tendon of the ring finger was transferred and attached to the flexor pollicis longus tendon using a Kessler suture (Figure 1(c)). Vascularization. The dorsal pedis artery and two accompanying veins were anastomosed to the radial artery and veins, respectively. The saphenous vein was anastomosed to the tributary of cephalic vein. Nerve reconstruction. The dorsal cutaneous branch of the superficial peroneal nerve was connected to the superficial branch of the radial nerve. The plantar digital intrinsic nerve was connected to the recurrent branch of the median nerve.
The skin was closed loosely. The patient received anticoagulant, anti-inflammatory and antispasmodic therapy for 7 days and kept his hand and foot elevated. The hand was immobilized for 3 weeks, followed by progressive physical therapy.
The flap survived completely (Figure 2(a) and (b)). By 8 months after surgery, the pinch function of the thumb was partially restored, as the thumb could touch the tips of the index, middle and ring fingers effortlessly (Figure 2(c)). The two-point discrimination on the flap was 12 mm and on the thumb pulp was 6 mm. The donor site also recovered well (Figure 2(d)). The patient was satisfied with the functional and cosmetic results.
(a) Post-operative appearance of the flap; (b) radiographs after reconstruction; (c) pinch function of thumb; (d) post-operative appearance of donor site.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for the publication of this case report together with the accompanying images.