
Abstract
This study aimed to determine the outcome of free vascularized medial femoral condyle bone grafts in the primary treatment of scaphoid nonunions with scaphoid foreshortening or carpal collapse and intraoperatively documented avascular necrosis. Thirty-two patients (28 male, four female) met the inclusion criteria. Median time from injury to surgery was 70 weeks. Thirty of 32 patients healed at a median of 12 weeks. There was significant improvement from preoperative to postoperative lateral intrascaphoid angle, scapholunate angle, and radiolunate angle. Two scaphoids failed to unite; one patient underwent scaphoidectomy and four-corner fusion 15 months postoperatively after suffering a subsequent injury. Another patient underwent 1,2-intercompartmental supraretinacular artery-based vascularized bone grafting at 4 months postoperatively and then scaphoid excision with four-corner fusion 4 years later. The free vascularized medial femoral condyle bone graft restores scaphoid vascularity and architecture while promoting union in a subset of scaphoid nonunions that has historically been a clinical challenge.
Introduction
Bone grafts have long been recognized as necessary in treating scaphoid nonunions. The use of vascularized or conventional grafts remains a matter of controversy. A meta-analysis of bone grafting techniques demonstrated vascularized bone grafts lead to higher union rates when the proximal pole is avascular (Merrell et al., 2002). Vascularized grafts in experimental canine carpal nonunions proved unequivocally superior to otherwise identical non-vascularized bone grafts (Jones et al., 2008; Sunagawa et al., 2000), not only healing more reliably but also revascularizing and remodelling the avascular proximal bone. In scaphoids with both carpal collapse and proximal pole avascularity, restoration of scaphoid length and thus carpal alignment is as important as improving proximal pole blood flow (Chang et al., 2006; Jones et al., 2008). This requires both a large intercalated bone graft and a means to restore blood flow to improve union rates (Jones et al., 2009). A free vascularized medial femoral condyle (MFC) bone graft fulfils both requirements and has been our preferred method to address this problem.
Previous reports of MFC bone grafts have included many patients with failed prior surgical procedures when carpal collapse and osteonecrosis are present (Jones et al., 2010). We consider the MFC bone graft to be appropriate and desirable for identical nonunions without previous surgery. This study measures outcomes and complications of MFC bone grafts used in previously untreated scaphoid nonunions.
Methods
A retrospective review was undertaken after approval from our institutional review board. All patients with previously untreated scaphoid nonunions treated from June 2006 through October 2016 with MFC bone grafts were identified. Only those with scaphoid foreshortening or carpal instability and proximal pole osteonecrosis were included (Figure 1). Scaphoid foreshortening was defined as a height-to-length ratio of greater than or equal to 0.65 (Bain et al., 1998). Carpal instability was defined as a revised carpal height ratio less than or equal to 1.52 (Nattrass et al., 1994), lateral intrascaphoid angle greater than or equal to 45° (Amadio et al., 1989), or radiolunate angle greater than or equal to 15° (Linscheid et al., 1972). Avascular necrosis (AVN) of the proximal pole was defined as an intraoperative lack of punctate bleeding of the proximal pole after debridement and deflation of the tourniquet (Green, 1985).
Preoperative radiographs of the posterior–anterior view (a) and computed tomography (CT) image (b) demonstrating a previously untreated scaphoid waist fracture.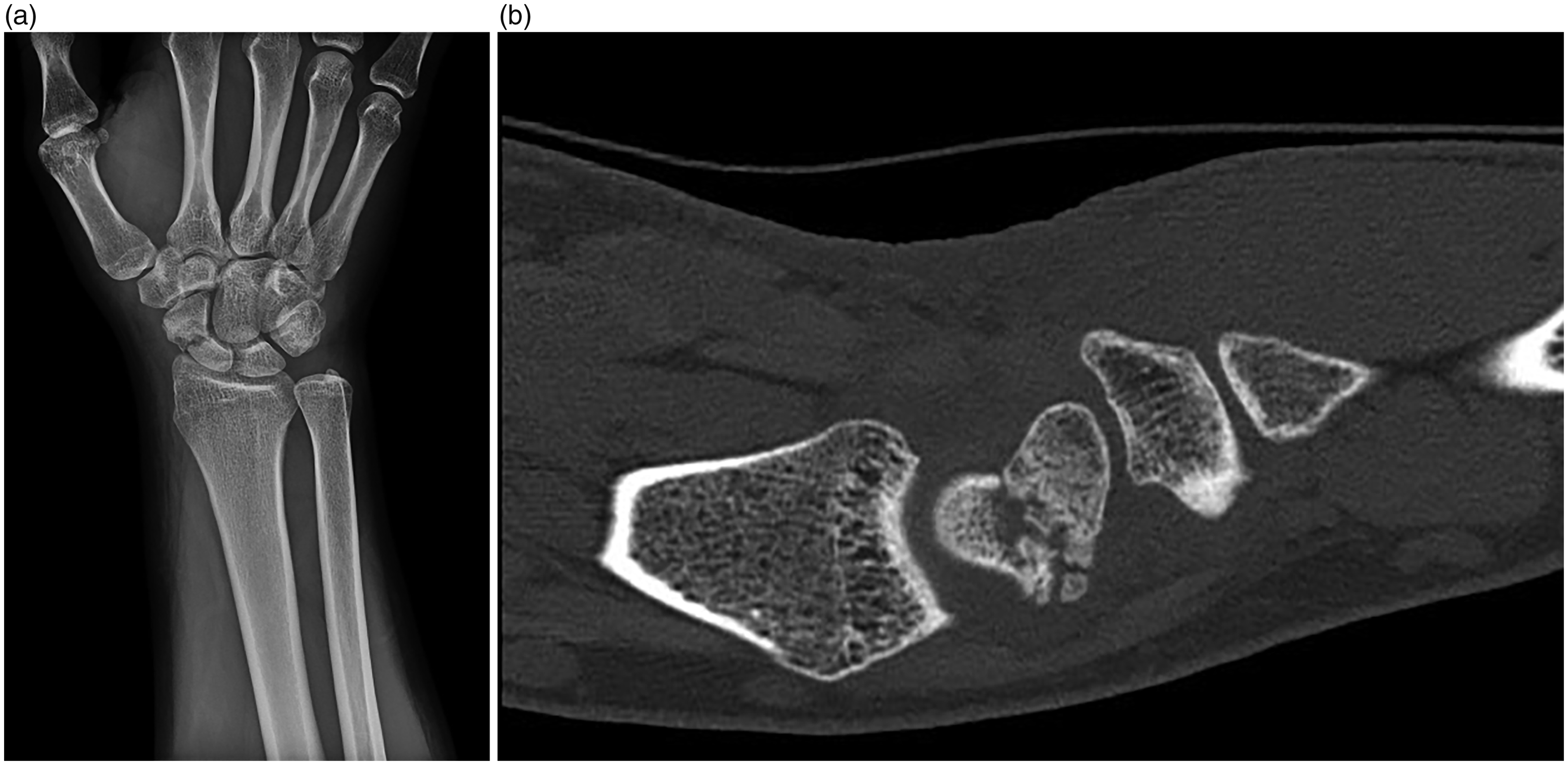
Medical records were reviewed along with pre- and postoperative imaging studies. Measures of revised carpal height ratio, scaphoid height-to-length ratio, lateral intrascaphoid angle, scapholunate angle, and radiolunate angle were made preoperatively and at final follow-up. Operative details including presence or absence of bleeding at the proximal pole, donor vessel, graft size, fixation method, and surgical times were recorded. All surgeries were performed with two teams: one team prepared the scaphoid and vessels at the wrist, and the second team harvested the ipsilateral MFC bone graft. The two teams converged for the insetting, fixation, and microsurgery. Time to union, carpal geometry, complications, and subsequent surgeries were recorded.
The surgical procedure for scaphoid nonunion reconstruction with a MFC bone graft has been previously described (Doi et al., 2000; Jones et al., 2010; Larson et al., 2007). In brief, the lunate extension was first corrected by wrist flexion with an image intensifier and a temporary radiolunate pin placed to maintain neutral lunate alignment. Through a palmar approach, the nonunion site was debrided, freshening the fracture surfaces with a high speed sagittal saw and minimal bone resection (Figure 2(a)). A lamina spreader improved the mobility of the fragments, permitting insetting of a sufficiently large graft to correct the scaphoid deformity and restore carpal alignment.
Intraoperative photos of (a) debridement of the nonunion site at the scaphoid (*) and preparation to accept the vascularized MFC graft. The proximal pole is indicated by the letter P and distal pole by the letter D. (b) Harvest of the MFC vascularized bone graft. In this case, the medial superior genicular artery was the donor vessel (*). The image is oriented so that anterior is at the top of the photograph and proximal is to the right of the photograph.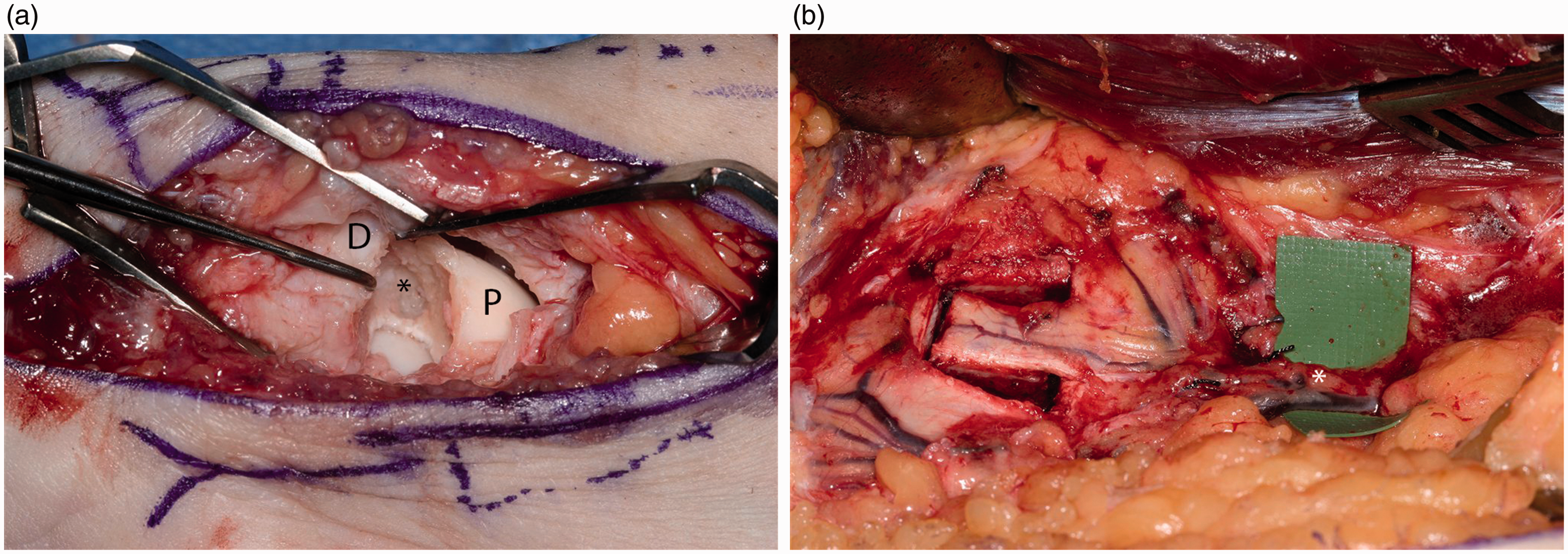
With AVN of the proximal pole established, an ipsilateral free vascularized MFC corticocancellous bone graft was raised, including either the descending or superior medial genicular vessels, based upon relative size (Figure 2(b)). Ipsilateral harvest permits use of a cane or crutch in the opposite hand when necessary. At the wrist, the MFC graft was trimmed as needed and positioned in the defect. It was then secured with a headless compression screw or multiple k-wires depending on adequacy of proximal bone stock.
Microvascular repairs of the genicular vessels were performed end-to-side to the radial artery and end-to-end to a radial vena comitans. The donor site was closed over a suction drain in a layered fashion, filling the femoral bone site with graft substitute (Stimulan, Biocomposites, Wilmington, NC, USA; or Osteoset Pellets, Wright Medical Group, Memphis, TN, USA).
Postoperatively, patients were immobilized in a long arm thumb spica splint for 2 weeks. This was followed by a long arm thumb spica cast for 4 weeks and a short arm thumb spica cast until union was confirmed. Immediate knee range of motion was allowed, with full weight-bearing as tolerated. Most patients walked immediately with no ambulatory aid, although a knee immobilizer was often helpful in the immediate postoperative period for confident ambulation. Serial radiographs were obtained until apparent union, always confirmed by a computed tomography (CT) study including coronal, sagittal, and axial scaphoid reconstructions (Figure 3). Union was defined as bridging trabeculae on the CT scan. Cast immobilization was continued and the CT repeated if union was not obvious.
Postoperative radiographs of the posterior-anterior view (a), lateral view (b) and CT slice (c) demonstrating healing of the bone graft at the fracture site.
Paired Student’s t-tests were used to compare pre- and postoperative continuous variables, such as carpal angles and indices. Statistical significance was set at a value of p < 0.05.
Results
Thirty-nine patients were treated with MFC bone grafts for previously untreated scaphoid nonunions during the study period. Two were lost to follow-up after surgery. Five patients had some punctate bleeding from the proximal pole and were excluded. Thirty-two patients met inclusion criteria for the study. There were 28 males and four females, with a median age of 20.5 years (range 15 to 58). Eleven patients were tobacco users. The dominant hand was affected in 18 patients. Eight patients had proximal pole fractures and 24 had middle third scaphoid fractures (Russe, 1960). The descending genicular artery was used as a donor vessel in 80% cases, and the medial superior genicular artery in the remainder. A cannulated scaphoid screw was used in 28 cases and two k-wires in four patients, the average screw length was 26.0 mm. Twenty-three of 28 screws were TriMed Headless Bone Screws or Scaphoid Screws (TriMed Orthopedics, Valencia, CA, USA). Average graft size was 11 × 10 × 10 mm (proximal/distal × palmar/dorsal × radial/ulnar). Average operative time was 2 hours and 44 minutes.
Preoperative and postoperative carpal indices.
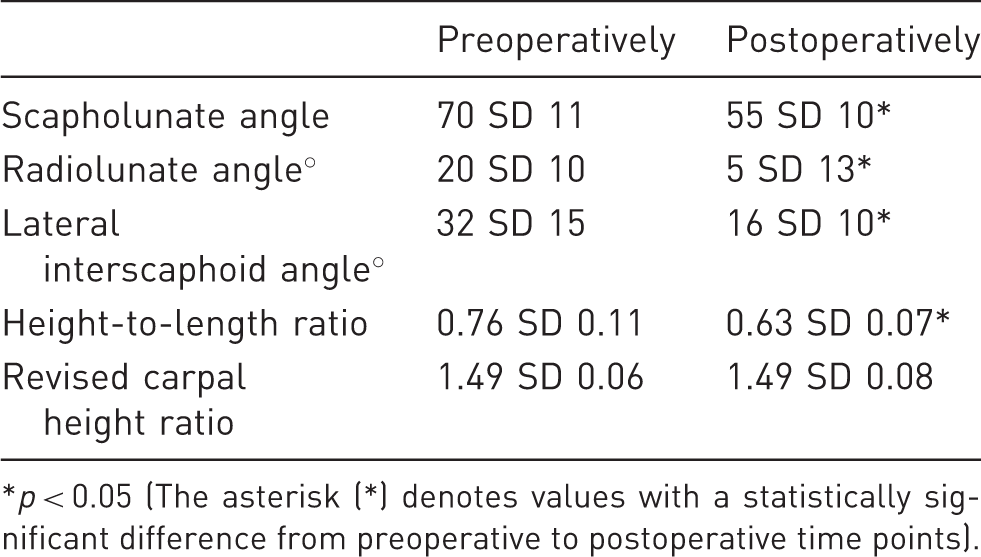
p < 0.05 (The asterisk (*) denotes values with a statistically significant difference from preoperative to postoperative time points).
There were no infections or other immediate postoperative complications. Eight patients underwent subsequent surgeries, including four planned k-wire removals. Four screws were removed, one with bone grafting and three without, for various reasons including joint penetration, loss of fixation, and nonunion. One patient underwent a scaphoidectomy and four-corner fusion at 15.2 months postoperative for a persistent nonunion with resorption of the bone graft. Another patient underwent 1,2-intracompartmental supraretinacular artery (1,2-ICSRA) based bone grafting 4 months after the index procedure owing to failure to heal. The scaphoid ultimately healed but developed scaphoid nonunion advanced collapse Stage III arthritic changes and subsequently underwent a scaphoidectomy and four-corner fusion 46.8 months after initial fixation. Both failures were fixed with cannulated headless compression screws. Four patients complained of donor site numbness in the saphenous nerve distribution, three of whom had spontaneous resolution prior to final follow-up.
Discussion
Scaphoid nonunion occurs in approximately 5%–15% of scaphoid fractures (Kuschner et al., 1994; Steinmann and Adams, 2006). Risk factors for nonunion include fracture displacement, proximal location, carpal instability, and osteonecrosis of the proximal segment. Osteonecrosis may occur in 13%–50% of fractures (Steinmann and Adams, 2006; Szabo and Manske, 1988) Treatment is further complicated by delay in diagnosis, misdiagnosis, or delay in presentation (Wong and von Schroeder, 2011). Unstable scaphoid fracture nonunions often develop a flexion or ‘humpback deformity’ resulting in a dissociative carpal instability that further increases the risk of nonunion, malunions with poor functional outcomes, and wrist arthritis (Lindstrom and Nystrom, 1992; Mack et al., 1984; Ruby et al., 1985).
Several options exist to address a nonunited scaphoid and successful treatment is predicated on matching the procedure to the specific characteristics of the nonunion (Smith and Cooney, 1996). For well-aligned scaphoid nonunions without excessive sclerosis or bone loss, minimally invasive techniques, such as arthroscopically assisted percutaneous, fixation is an option (Slade et al., 2003). Fracture of the scaphoid with mid-carpal instability leads to a flexion deformity of the scaphoid and palmar bone resorption, often resulting in progressive ‘humpback’ deformity and eventually arthritis. Fisk recognized that the geometry of the scaphoid must be restored in order to restore normal wrist kinematics. He favoured anterior wedge grafting from the radial styloid to restore normal scaphoid length, restore tension to the palmar radiocarpal ligaments, and, in turn, correct the pathologic rotation of the lunate (Fisk, 1970). Fernandez used an iliac crest wedge graft with internal fixation (Fernandez, 1984). While anterior wedge grafting produced improved outcomes compared with the Matti-Russe technique, AVN at the proximal pole has remained an independent risk factor for a poor functional outcome (Steinmann and Adams, 2006; Szabo and Manske, 1988).
To address AVN, the use of several vascularized bone grafts has been reported. The majority of these grafts have traditionally been rotational flaps based on arteries from the distal radius, which avoids the need for microsurgical vessel anastomosis (Kawamura and Chung, 2008; Zaidemberg et al., 1991). Most commonly, the 1,2-ICSRA bone graft is used (Steinmann et al., 2002). Union rates range have been reported as high as 80% to 100% (Chang et al., 2006; Malizos et al., 2007; Straw et al., 2002).
Two recent reports have called into question whether AVN is truly predictive of failure in scaphoid nonunion surgery. A recent study reported a 91% union rate with non-vascularized iliac crest bone grafting (Kim et al., 2018). All nonunions had established AVN intraoperatively via the Green method. Cancellous bone grafting was used in well-aligned nonunions and the Fisk–Fernandez technique in scaphoids with humpback deformity. However, the authors did not distinguish between primary and revision fractures. Though improvement of humpback deformity, as measured by height-to-length ratio, was statistically significant (p < 0.01), the minimal improvement of 0.03 may not have been clinically significant. Another study prospectively followed 35 scaphoid nonunions treated with non-vascularized bone grafting (Rancy et al., 2018). Vascularity was measured by magnetic resonance imaging (MRI), intraoperative bleeding, and histopathological analysis. Thirty four of 35 scaphoids went on to union, and avascularity established by any method was not found to correlate with healing. Both structural and non-structural bone graft was used based on whether a humpback deformity was thought to be present. However, the authors do not provide details of any carpal indices to determine whether the anatomy had been re-established, and functional outcomes were not reported.
Small graft size and relatively weak radial styloid bone often fail to restore scaphoid length. In one study, a preoperative humpback deformity and/or dorsal intercalary segment instability (DISI) were risk factors for 1,2-ICSRA bone graft failure (Chang et al., 2006). Free vascularized iliac crest bone grafts have also been used for avascular collapsed scaphoids (Arora et al., 2010; Gabl et al., 1999; Harpf et al., 2001). Alternatively, a conventional iliac crest graft may be combined with an arteriovenous bundle implanted in the proximal pole (Fernandez and Eggli, 1995). Union rates for these procedures range from 71%–91%. However, pre- and postoperative radiographic carpal measurements are often not reported.
Free vascularized MFC bone grafts are increasingly utilized. We have previously compared our initial experience with MFC bone grafts to pedicled distal radius bone grafts (Jones et al., 2008). MFC bone grafts in this initial experience were uniformly successful in scaphoids with both humpback deformity and AVN, as compared with only 40% with 1,2-ICSRA bone grafts. Lateral intrascaphoid angle was demonstrated to be significantly improved in the MFC group compared with those treated with a 1,2-ICSRA bone graft (32 versus 48°, p < 0.01). Other carpal measures, such as scapholunate and radiolunate, angles were significantly improved postoperatively in the MFC group (Bain et al., 1998). However, nine of the 12 patients had previously failed surgical management. The role of an MFC bone graft in primary scaphoid reconstruction for nonunions with AVN and carpal collapse has remained unclear.
Our indications for a free vascularized MFC bone flap include carpal malalignment, AVN of the proximal pole, and no more than scaphoid nonunion advanced collapse Stage I arthritic changes (Vender et al., 1987). Preoperative radiographs and CT scans are used to assess carpal alignment, scaphoid deformity, proximal pole size, fragmentation, and arthritic changes. As MRI has not been shown to be a reliable method for assessing proximal pole vascularity, it is not routinely ordered (Willems et al., 2011). Instead, we rely on an intraoperative assessment of proximal vascularity as described by Green (1985). Vascularized bone grafting is indicated in cases of AVN as this improves union rates significantly (Gabl et al., 1999). For AVN without significant scaphoid height loss or distortion of scaphoid geometry, we will typically perform an inlay graft, such as the 1,2-ICSRA bone graft. In cases of a fragmented proximal pole or pre-existing mid-carpal arthritis, we will perform a salvage procedure, usually scaphoidectomy with limited wrist fusion.
We recognize the limitations of a retrospective case series, including the potential for selection bias in our patient population as well as the lack of a control group. This may limit any conclusions that may be drawn regarding comparative efficacy of this graft to produce union or restore carpal parameters relative to other available grafts. Similarly, we have limited our report to results of the two senior authors who each have greater than 10 years’ experience performing this operation at a tertiary referral centre, which may limit generalizability of our results. Additionally, due to our short clinical follow-up, we were unable to make any statistical inferences regarding clinical outcomes, such as wrist range of motion and grip strength.
These limitations notwithstanding, we have reported excellent radiological results in a difficult patient population, those with scaphoid nonunion with deformity and AVN. The importance of restoring both appropriate scaphoid geometry and vascularity are well established as these patients are at high risk of going on to further complications, such as advanced carpal collapse and arthritis (Amadio et al., 1989; Fisk, 1970; Merrell et al., 2002 Vender et al., 1987). A free vascularized MFC bone graft is an option that can achieve both goals of restoring scaphoid geometry and vascularity with high rates of union.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This research was reviewed and approved by the Mayo Clinic Institutional Review Board. IRB# 12-008321.