
Abstract
Dear Sir,
A comminuted intra-articular fracture with a central depression of the base of the proximal phalanx is known as a pilon fracture and is relatively rare. Fixation and early motion are needed to prevent pain and stiffness in the metacarpophalangeal (MCP) joint (Dean and Little, 2011). We treated two patients with pilon fractures of the proximal phalanx with screw fixation using a dorsal approach.
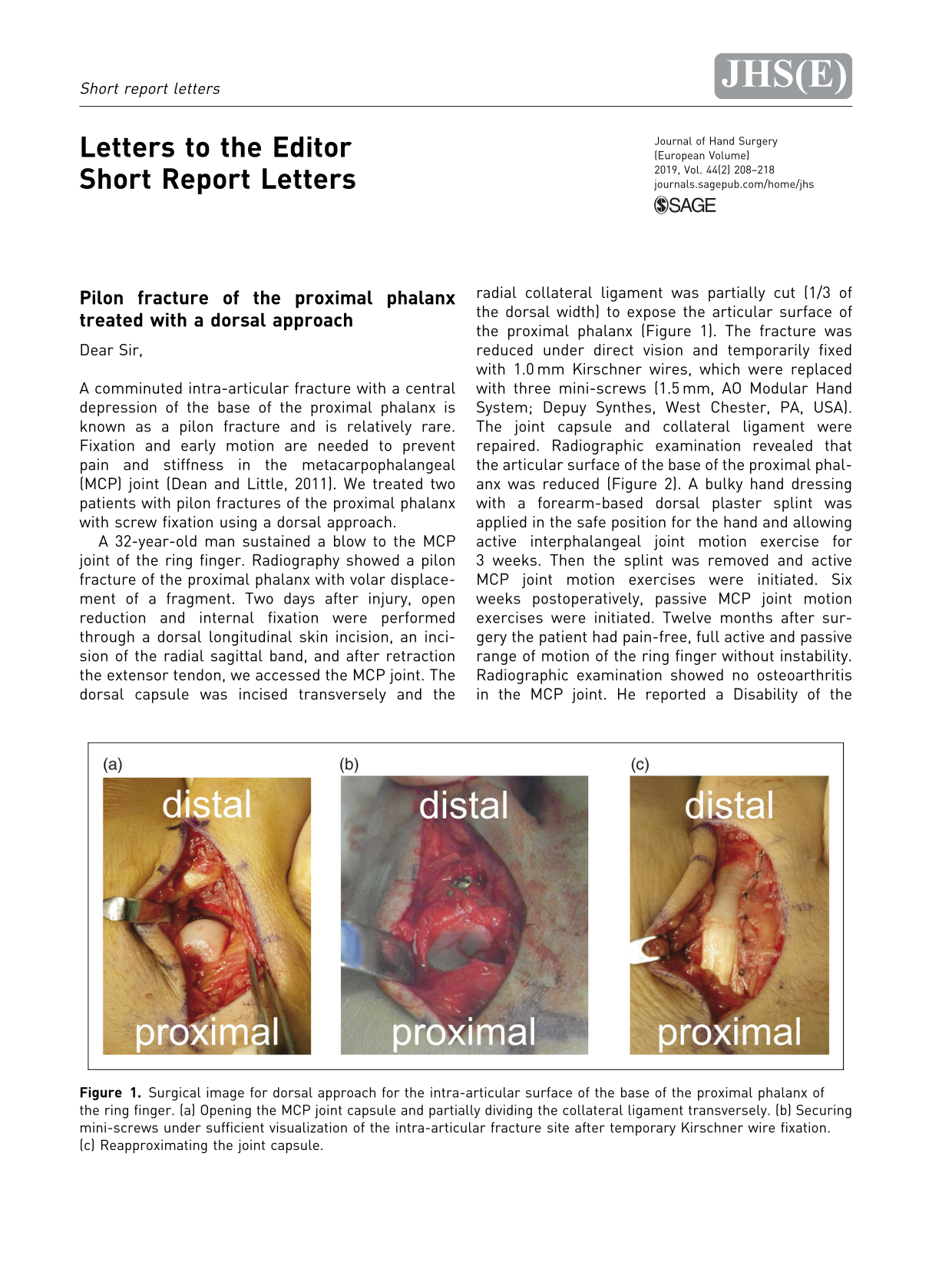
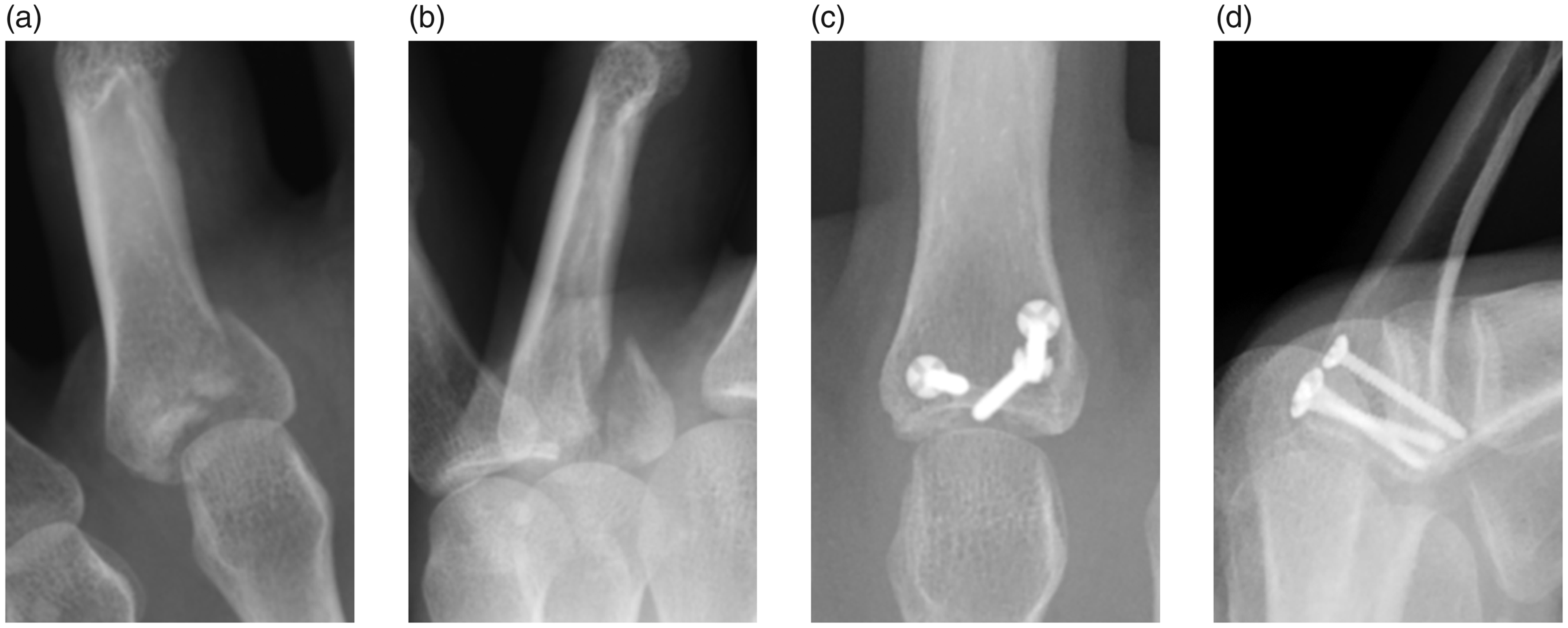
A 32-year-old man sustained a blow to the MCP joint of the ring finger. Radiography showed a pilon fracture of the proximal phalanx with volar displacement of a fragment. Two days after injury, open reduction and internal fixation were performed through a dorsal longitudinal skin incision, an incision of the radial sagittal band, and after retraction the extensor tendon, we accessed the MCP joint. The dorsal capsule was incised transversely and the radial collateral ligament was partially cut (1/3 of the dorsal width) to expose the articular surface of the proximal phalanx (Figure 1). The fracture was reduced under direct vision and temporarily fixed with 1.0 mm Kirschner wires, which were replaced with three mini-screws (1.5 mm, AO Modular Hand System; Depuy Synthes, West Chester, PA, USA). The joint capsule and collateral ligament were repaired. Radiographic examination revealed that the articular surface of the base of the proximal phalanx was reduced (Figure 2). A bulky hand dressing with a forearm-based dorsal plaster splint was applied in the safe position for the hand and allowing active interphalangeal joint motion exercise for 3 weeks. Then the splint was removed and active MCP joint motion exercises were initiated. Six weeks postoperatively, passive MCP joint motion exercises were initiated. Twelve months after surgery the patient had pain-free, full active and passive range of motion of the ring finger without instability. Radiographic examination showed no osteoarthritis in the MCP joint. He reported a Disability of the Arm, Shoulder, and Hand score of 0. We subsequently performed this operation in a second patient with a similar fracture and achieved the same outcome.
Surgical image for dorsal approach for the intra-articular surface of the base of the proximal phalanx of the ring finger. (a) Opening the MCP joint capsule and partially dividing the collateral ligament transversely. (b) Securing mini-screws under sufficient visualization of the intra-articular fracture site after temporary Kirschner wire fixation. (c) Reapproximating the joint capsule. (a) Preoperative radiograph showing the anteroposterior view of the proximal phalanx of the ring finger. (b) Preoperative radiograph showing the lateral view. (c) Postoperative radiograph showing the anteroposterior view. (d) Postoperative radiograph showing the lateral view.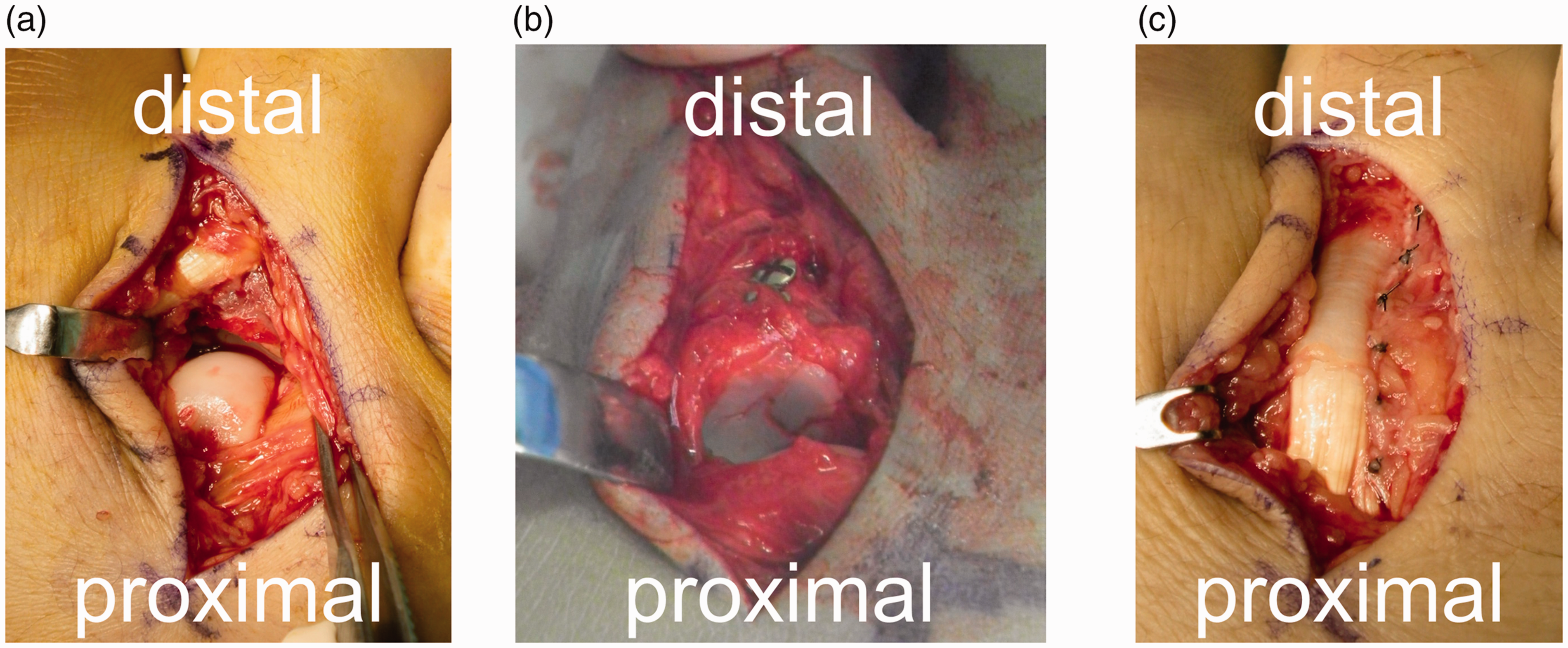
Treatment strategies for middle phalangeal pilon fractures have been well studied (Henry, 2017). The use of smaller sized locking plates instead of external fixators offers stability during early motion therapy. However, plate fixation might lead to attrition of the overlying tendon. Mini-screw fixation used in this case is less compromising to the tendon.
For open reduction and internal fixation of a pilon fracture of the proximal phalanx, the options of volar and dorsal approaches are available. Oftentimes a volar approach is used to manipulate the intra-articular volar fragment. Hattori et al. recommended volar buttress plating for an intra-articular fracture of the base of the proximal phalanx through a volar A1 pulley approach (Hattori et al., 2007). However, this approach is potentially harmful to the flexor tendon and joint and demands meticulous surgical technique. Because a partial release of the A2 pulley is required and the volar plate must be divided for volar buttress plating, flexor tendon bowstringing and dorsal instability of the MCP joint can occur. Kaneshiro and Hidaka (2014) reported numbness in the finger pulp caused by traction on the digital nerve during surgery in two of six cases using the volar A1 pulley approach. The risk of iatrogenic neurovascular bundle injury should be less in the dorsal approach than in the volar approach.
The dorsal approach provides sufficient visualization of the intra-articular fracture site. The combination of the dorsal approach and mini-screw fixation is minimally invasive and less technically demanding than the volar approach.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient consent
Consent to report these two cases in its entirety were obtained from the patient prior to its publication.